The number of coordinated specialty care (CSC) programs has recently increased across the United States. In 2008, two states (Oregon and California) reported using federal funds to support 12 CSC programs (
1,
2). Today, the National Early Psychosis Directory of the Early Assessment and Support Alliance (EASA) notes that 344 CSC programs have been established, including programs in every state and four U.S. territories. The multibillion-dollar federal investment through the National Institute of Mental Health’s (NIMH’s) Recovery After an Initial Schizophrenia Episode (RAISE) project and the Mental Health Block Grant (MHBG) set-aside funds for early psychosis likely prompted, in part, the proliferation of CSC programs across the country (
3).
CSC is a team-based program that includes a set of evidence-based outpatient services designed to address the needs of individuals experiencing early or first-episode psychosis (FEP) (
4–
9). Through early intervention, CSC is used to prevent the onset of serious mental illnesses and improve quality of life (
6,
7). Although models of CSC (e.g., OnTrack, EASA, and NAVIGATE) vary, NIMH has identified common service components for CSC programs (
10,
11). The components include having a designated team lead and the provision of the following evidence-based services: case management, individual or group psychotherapy, supported employment, supportive education, family psychoeducation, family support, and psychopharmacology.
The rapid growth of CSC is unique compared with growth of other evidence-based interventions. A major difference between most behavioral health treatment programs and CSC is that, in 2014, states received federal MHBG set-aside funds for the treatment of people with FEP (
11). The MHBG program is a formula-based state grant program in which federal funds are distributed to states and territories, with the amount varying according to specified economic and demographic factors. In 2014, Congress included a 5% set-aside in the MHBG to support states in developing early intervention services for psychosis, including CSC (
11). States could provide funding to existing CSC programs or fund new CSC programs. There were no requirements regarding the type of provider organization the funds could go to or whether the organization had previously received federal funding. In 2016, the 21st Century Cures Act increased the set-aside to 10% and included a supplement (
12). The 2016 federal guidance noted, “States can implement models which have demonstrated efficacy, including the range of services and principles identified by NIMH via its [RAISE] initiative” (
12). Although federal guidance encouraged states to implement the range of services and principles outlined in RAISE (
11–
14), states were not required to do so. States were also given freedom to select the CSC model to implement, the types of services and training activities to fund, and the criteria to require for admission. No services were required, and there was no penalty for failing to offer a minimum number of CSC services.
By 2018, the MHBG set-aside was funding 244 CSC programs in the United States (
3). Although past reports have described these programs (
3,
15), no studies to date have surveyed program leadership from the entire national sample of MHBG-funded CSC programs. Additionally, existing information about CSC programs was gathered in part through interviews with state mental health authorities (SMHAs), who may not have had access to detailed information about CSC program characteristics. Therefore, little is known about the implementation of these programs. As more outcome data become available and states increase support for CSC expansion, understanding program characteristics and their correlates will likely have implications for the ongoing expansion and quality of CSC programs. Examining aspects of CSC programming is timely, given the influx of 2021 funding to states through the COVID-19 Relief Supplement and increased MHBG set-aside funding, which will once again double to support the implementation of CSC. Questions that require consideration include whether programs are providing evidence-based services and whether federal support for CSC implementation is a viable approach for disseminating important mental health programs nationally. This study reports the results of a 2018 survey of CSC programs funded by the MHBG set-aside for the treatment of people with FEP in that year.
Methods
Design, Sampling, and Procedure
As part of a multimethod study examining CSC programs receiving MHBG set-aside funds, we collected data by using a 28-item online survey assessing CSC program characteristics such as size, client capacity, duration of care, referral sources, services offered, and outcomes. Because the MHBG set-aside funds are administered by states, CSC programs were identified by SMHAs as part of their federal reporting (
3). SMHAs identified programs that received set-aside funds and used at least 1% of the MHBG set-aside funding to cover CSC program costs. Additional funding sources used by CSC programs could include Medicaid, private insurance, other state funds, local funding, endowments, or grants. In rare instances, study staff spoke directly with SMHA staff members to clarify CSC program eligibility for the study and to confirm that program costs were supported by MHBG funds.
We collected data between February and June 2018. Respondents were program leaders at 244 MHBG-funded CSC clinics identified by SMHAs (
3). Of the 244 CSC programs recruited, 215 (88%) completed the survey. Programs in this sample were located in 44 states, the District of Columbia, and three U.S. territories. Participants indicated informed consent before initiating the survey. To minimize reporting bias, the informed consent notice and letter of invitation to CSC program leadership emphasized that data would be reported at the aggregate level and that SMHAs would not see the individual survey responses by CSC program staff. Summary statistics and descriptive analyses, conducted in SAS, version 9.4, were used to describe characteristics and patterns of CSC programming. Responses to survey items addressed the time frame for the start of the CSC program, services offered, training, program capacity, current client enrollment, and enrollment criteria. All aspects of this study were reviewed and approved by the Westat Institutional Review Board.
Results
Initiation of CSC Programs
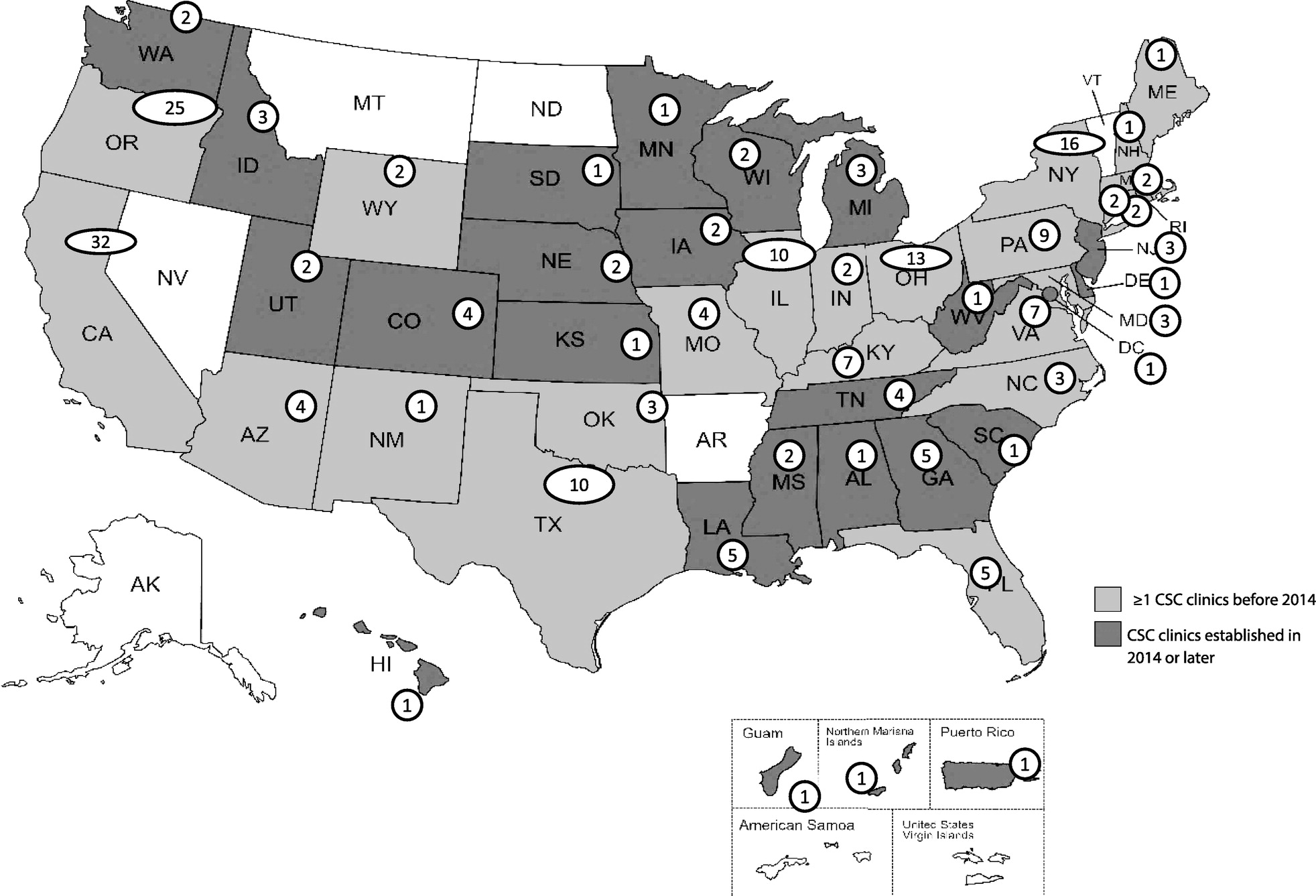
As shown in
Figure 1, the survey included 215 CSC programs across 44 states, the District of Columbia, and three U.S. territories. About one-third of CSC programs in the study (N=67, 31%) reported providing services for clients with FEP before 2014, when the MHBG set-aside funds were allocated. Most CSC programs (N=148, 69%) were initiated in 2014 or later. Among the 148 programs that began after 2014, more than half (N=83, 56%) were initiated in or after 2016, when the MHBG set-aside funding doubled.
Services Provided by CSC Programs
Most programs reportedly offered core components of CSC as defined by NIMH guidance to states (
Table 1), including having a team lead and offering case management, family education and support, low-dose antipsychotic medication treatment, supported employment, and supported education (
11). A majority also reported offering additional services, including crisis intervention services, peer support services, primary care coordination, and co-occurring substance use services.
Training on CSC Service Delivery
Leadership of CSC programs (N=211) reported receiving technical assistance and training on various CSC models, including OnTrackNY (N=56, 27%), NAVIGATE (N=34, 16%), EASA (N=32, 15%), FIRST (N=19, 9%), PIER (N=7, 3%), other programs (N=28, 13%), or a combination of two or more (N=23, 11%); 6% (N=12) received no technical assistance or training.
Client Enrollment
Across all CSC programs, the total capacity for enrollment was 8,255 clients. The programs most commonly noted that their maximum client capacity was between 21 and 30 clients (N=57 of 214, 27%) or between 41 and 100 clients (N=56 of 214, 26%). Respondents reported that the number of enrolled clients at the time of the survey was lower than capacity, with 29% (N=63 of 214) of the programs reporting current enrollment of <10 clients. Only 14% (N=29 of 214) of programs were at full capacity, nearly one-third (N=66 of 214, 31%) were at ≤50% capacity, and about one-tenth (N=24 of 214, 11%) were at ≤25% capacity.
Enrollment Criteria
CSC program leadership reported enrolling clients with a diagnosis of schizophrenia (N=207 of 210, 99%), schizoaffective disorder (N=200 of 210, 95%), psychotic disorder not otherwise specified (N=194 of 210, 92%), schizophreniform disorder (N=167 of 210, 80%), affective disorders with psychotic features (N=120 of 210, 57%), delusional disorder (N=104 of 210, 50%), and posttraumatic stress disorder (N=53 of 210, 25%). Overall, 19% (N=41 of 214) of programs had an enrollment criterion about whether clients had been prescribed antipsychotic medication before enrollment. Most programs (N=179 of 214, 84%) had client enrollment criteria that included a measure of duration of untreated psychosis (DUP), and nearly half (N=85 of 179, 47%) indicated that their inclusion criterion for DUP was 13–24 months. Client age for inclusion in CSC clinics ranged from 10 to 65 years (
Table 2).
Discussion
More than 340 CSC programs have been established, including in every state in the United States. Before receiving the MHBG set-aside funding in 2014, treatment programs for FEP were slow to develop because public policy prioritized services for individuals who were already disabled by mental illness. CSC emerged as a federal priority because of growing scientific evidence accumulated from other countries (e.g., Australia, Canada, and the United Kingdom) suggesting the importance of reducing DUP and treating FEP with evidence-based services using a team-based approach (
6).
Information regarding the growth in the number of U.S. CSC programs over time remains limited. In 2008, two states supported CSC programs (
1,
2). By 2014, 25 states had CSC or early psychosis programs, and among them, 20 were involved in the NIMH RAISE studies (
11). Subsequent reports came from the Substance Abuse and Mental Health Services Administration–funded State Snapshots series that collects information from the SMHAs within each state and U.S. territory (
3,
15). The current survey was the first to contact and collect information directly from the programs receiving MHBG set-aside funds and to document program-level data.
The development of CSC programs in U.S. academic settings, positive results from RAISE, and increasing congressional concern about psychotic disorders among young people led to legislation expanding the MHBG and creating the set-aside. As was the case with earlier efforts in federal mental health policy, such as the community mental health legislation of the 1960s or the community support reforms of the 1980s, the expansion of CSC programs in the United States reflects how federal leadership can balance state and local innovation with federal incentives to shape service delivery (
16).
This study examined the characteristics of 215 federally funded CSC programs. The programs surveyed were identified by SMHAs as receiving MHBG set-aside funds in 2018, and they represented a unique group of service organizations that were defined within this study by the funding mechanism that supported them. The findings of this study strongly suggest that the MHBG set-aside funding played an important role in stimulating the emergence of CSC programs in the United States. One-third of the CSC programs, including programs in 23 states, predated the 2014 MHBG set-aside, suggesting that, although they received MHBG set-aside funds at the time of the survey, they were not created as a result of the funds. This finding is consistent with NIMH state data that show that CSC programming was available in approximately 25 states before the availability of the MHBG set-aside funding (
11). In this study, nearly 70% of CSC programs were started in 2014 or later, after the initial MHBG set-aside allocation. Of the programs that began in 2014 or later, >50% started after 2016, when the MHBG set-aside funds were increased.
Although this study did not directly test whether the MHBG set-aside funding led to the expansion of CSC programs within the United States, our results suggest that set-aside funds were influential in the initiation of these programs. Furthermore, the literature shows that the lack of cohesive funding mechanisms that cover CSC’s intensive, comprehensive, individualized, team-based, and multiservice approach poses a challenge to initiating programs in the United States (
17–
19). For example, Medicaid and private insurance do not fund many components of CSC programs, such as team meetings, supported education, and family education. The MHBG set-aside funds enable provider organizations to conduct start-up activities, such as staff training and community outreach to identify potential clients, and to provide the full array of CSC services. This funding, along with the federal mandate, likely influenced the proliferation of these programs.
Conformity With Federal Guidance
Respondents noted that their programs implemented CSC at the time they completed the survey, but no CSC fidelity assessment was conducted to confirm this designation. Despite this limitation and the risk for social response bias, the CSC programs funded by the MHBG set-aside exhibited many similarities. Although states’ conformity with the federal guidance was not required, the guidance was likely effective in shaping the CSC programs. For example, states received access to materials developed through the NIMH-funded RAISE initiative, which included listings of CSC core services. More than 90% of CSC programs reported providing each of these core CSC components. Also consistent with federal guidance, most of the CSC programs had client enrollment criteria that included a measure of DUP before entering the program (
10). Most programs also reported offering crisis intervention services, peer support services, primary care coordination, and co-occurring substance use services. The reason for providing these additional services is unclear. Certainly, CSC components such as supported employment, family education, and peer support services are available in most states, independently of CSC programs. A majority of states may have already been placing high priority on these services, and thus incorporating these services as part of CSC may have been easier. Alternatively, the survey question may have been misinterpreted, such that respondents included the availability of services offered by the outpatient clinic associated with the CSC program, rather than the CSC program itself. Future studies should further investigate the role of the state in influencing the availability of these service components.
Variation Among Programs
Where federal guidance was less prescriptive, CSC programs differed in program format and client characteristics. For example, federal guidance did not specify which CSC program model to adopt (e.g., NAVIGATE, EASA, or OnTrackNY). As such, states and programs had flexibility in selecting the type of technical assistance and training that staff members of clinics received. No more than one-third of the CSC programs selected the same model, with the OnTrackNY model being used by most CSC programs; 11% of the CSC programs had training in multiple models. Similarly, client age for inclusion in CSC programs varied, with ages ranging from 10 to 65 years. Approximately half of the CSC programs had a minimum age for clients of 14–15 years. Most of the clinics reported that their maximum enrollment age was between 30 and 39 years. It should be noted that the age range of ≥40 years falls outside of the typical range for which CSC has been reported as effective in clinical trials and systematic reviews (
4,
11,
20).
Broader Applicability of Set-Aside Funding
Regardless of the aforementioned heterogeneity among the CSC programs, it appears that the use of MHBG set-aside funds that are administered by states is an effective approach to promulgate specific mental health interventions nationally. Admittedly, use of federal funding to increase the availability of mental health treatment is not new; federal funds have been in place since the 1960s, when the federal Community Mental Health Centers program was launched and grant funding was provided directly to centers willing to deliver essential services, as defined by NIMH (
17,
21). Since the 1980s, states have taken a larger role in shaping mental health services, guiding availability of services through state Medicaid plans, determining benefit design and reimbursements, and administering the MHBG. Recent examples of federal policy influence include the government’s role in defining the essential services within the Affordable Care Act, the rollout of the Certified Community Behavioral Health Center programs, and most recently the COVID-19 Relief Supplement funds, which can be used to develop and support evidence-based crisis services for adults and youths with mental illnesses (
22–
24). In 2020 and 2021, states received additional federal funds for their CSC programming: $82.5 million through the MHBG COVID-19 Supplement and $150 million through the American Rescue Plan (ARP). States have until March 2023 to expend the COVID-19 Supplement and until September 2025 to expend the ARP funds. How states choose to direct federal funding for CSC will continue to shape its implementation. The results of this study suggest that research-based federal guidance can play a vital role in shaping how these funds are used.
Future studies may investigate how the CSC programs funded by the MHBG set-aside funds compare with those that do not receive these funds. It would be useful to assess whether the amount of MHBG set-aside funding, or the percentage of overall CSC program costs covered by MHBG set-aside funding, influences the services offered or other program characteristics. Furthermore, it would be valuable to investigate how decision making at the state level occurs, regarding which clinics are funded and which CSC models are selected for implementation. These levers of decision making may be important in how CSC programs function. Finally, this study did not investigate the quality of these programs or whether CSC was being offered with fidelity to a certain model. This gap represents an important avenue of further research.
Conclusions
The current study of CSC programs funded through the MHBG set-aside in 2018 highlights that federal funding and guidance may help shape national implementation efforts. This approach to the administration of federal funds by the states for CSC may inform the rollout of other behavioral health interventions, although more research is needed to determine the factors that may shape national dissemination efforts and program characteristics. Additional studies could focus on the influence of various factors, including state leadership, age of the program, the relative amount of MHBG set-aside funds, how the funds are used, and how the core components of CSC are offered.