Sample
We conducted a cross-sectional survey of 2,000 randomly selected students who were enrolled at the University of Geneva in October 1997. A questionnaire was mailed to the students in November of that year, and up to two follow-up reminders were sent to nonrespondents over the next three months. Of the 1,954 students remaining after the deletion of incorrect or foreign addresses (98 percent), 1,257 (64 percent) responded to the questionnaire.
Variables and instruments
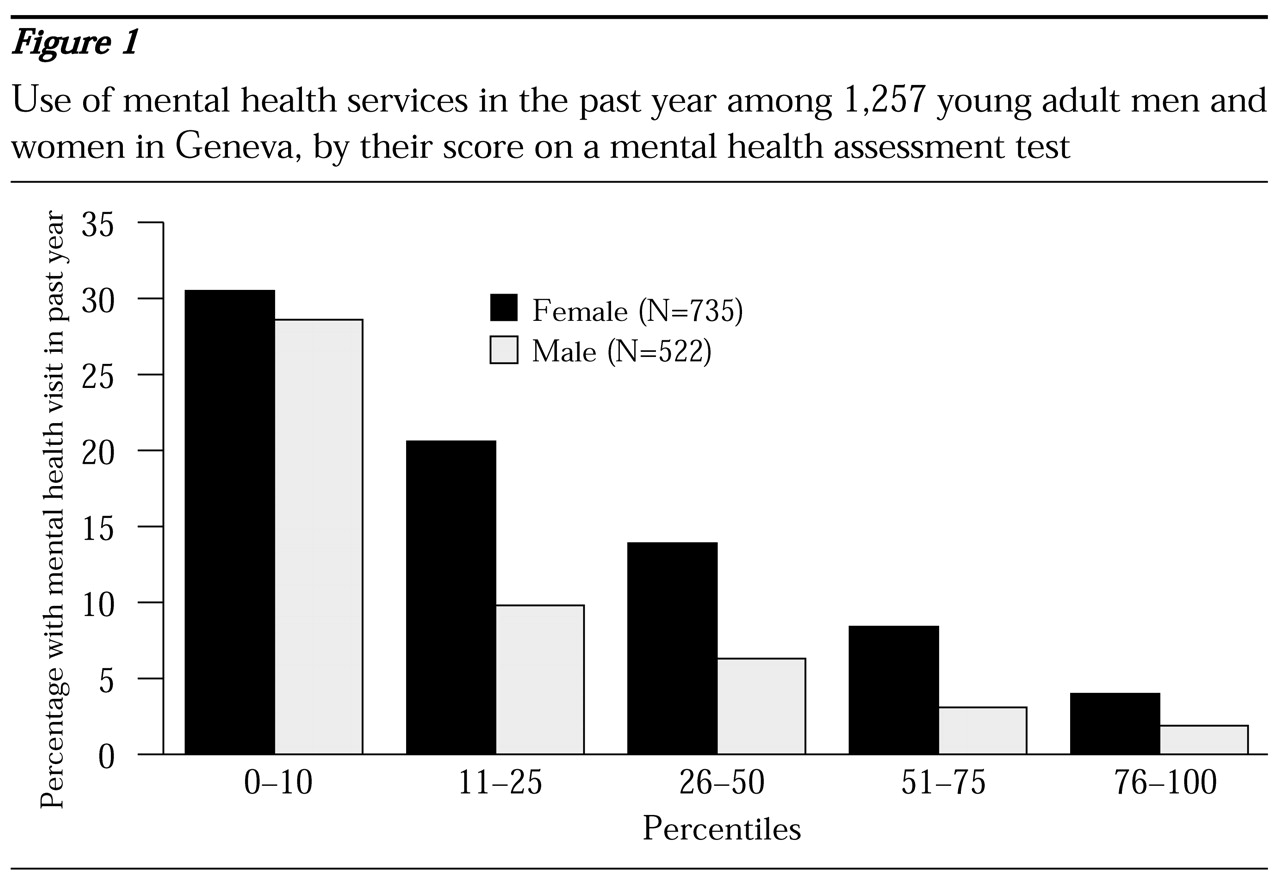
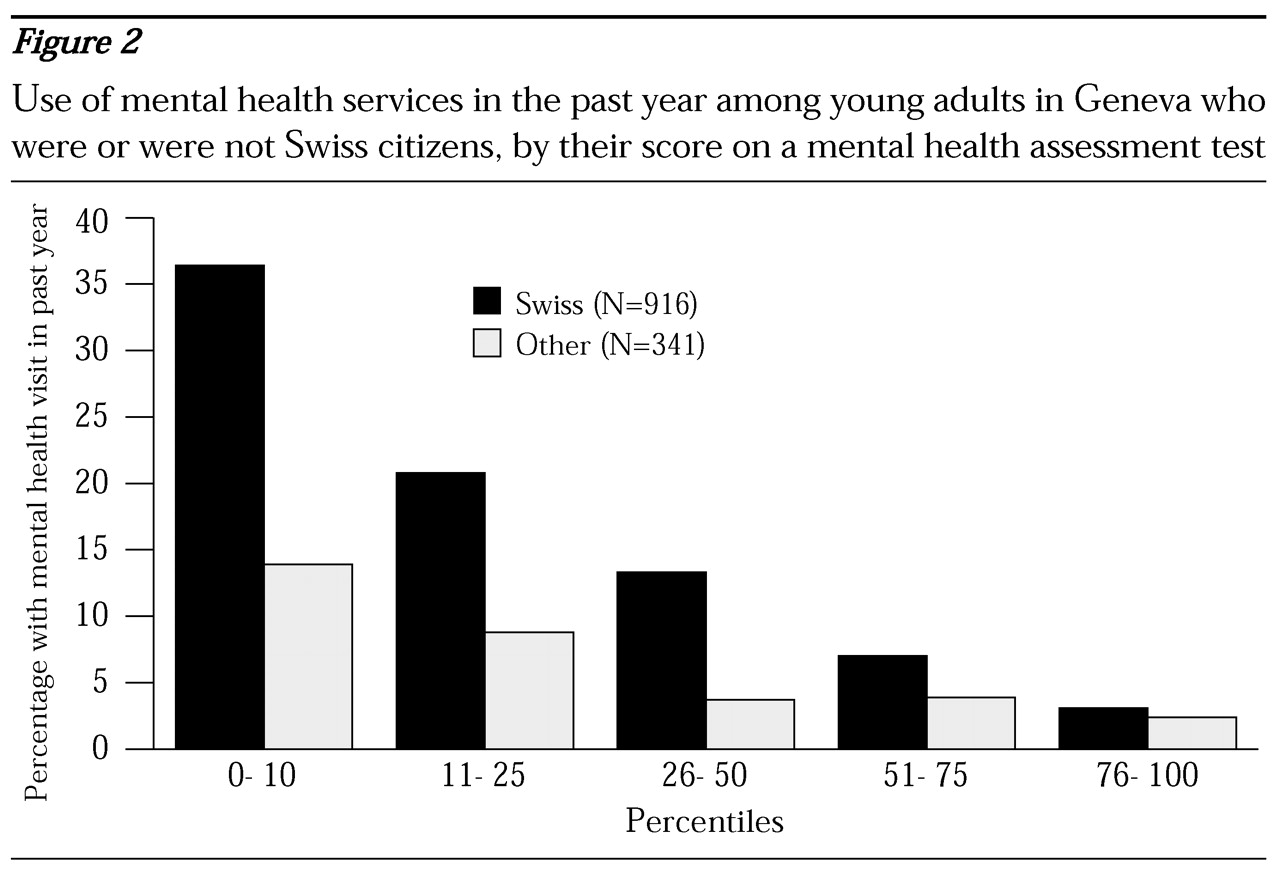
The dependent variable in the study was the students' use of ambulatory mental health services in the previous 12 months. Respondents were asked how many times during that period they had visited a psychiatrist or a psychologist and how many times they had visited other health care providers, such as a family doctor or a medical specialist. Respondents who reported at least one visit to a psychiatrist or a psychologist were classified as users. We did not ascertain whether visits to health professionals other than psychiatrists were motivated by a mental health problem.
We measured the respondents' mental health status with the 12-item Short-Form Health Survey (SF-12), version 2 (
10). Earlier versions of this instrument have been shown to accurately identify individuals who have a psychiatric disorder (
11). Because algorithms to compute the physical health and mental health scores for version 2 were not available at the time of analysis, we performed a factor analysis of the 12 items, followed by varimax rotation. This analysis yielded a two-factor solution that can be used to represent physical and mental health constructs.
We used the resulting loadings to compute two orthogonal summary scores of mental and physical health, each being a distinct linear combination of the 12 items. Consistent with predictions, the general health item loaded moderately on both dimensions, and the other items loaded predominantly on the dimension they were designed to measure. Summary scores of physical and mental health were standardized to have a mean of 50 and a standard deviation of 10.
Perceived stress was measured with the Brief Encounter Psychosocial Instrument (BEPI) (
12,
13), a five-item scale that measures the balance between perceived daily life demands and capability to cope with these demands (for example, "In the past month, have you ever felt as if there are more demands in your life, emotionally and physically, than you can handle comfortably?"). Responses were scored on a scale of 0 to 10, with higher scores indicating worse functioning. The BEPI was internally consistent (Cronbach's alpha=.84), and a factor analysis confirmed that its items represented a single dimension.
Internal resources—sense of mastery and self-esteem—were measured with an eight-item instrument adapted from the work of Pearlin (
14). The score for each subscale was computed by averaging the values of the corresponding items. Both subscales had good internal consistency (Cronbach's alpha=.81 for self-esteem and .72 for mastery), and the bidimensional structure of the instrument was confirmed by factor analysis.
We used a six-item instrument adapted from the Duke-UNC Functional Social Support Questionnaire (
15) to measure confidant and affective social support. The score for each subscale was computed by summing relevant items. Internal consistency was satisfactory for both subscales (Cronbach's alpha=.70 for affective support and .79 for confidant support), and factor analysis confirmed the underlying constructs.
We used the official French translation of the SF-12. For the other scales, we produced French translations in a standardized procedure: three independent translations, selection of a consensus translation by an expert panel, and pretests. A description of the items and detailed validation of the instruments are available from the authors.
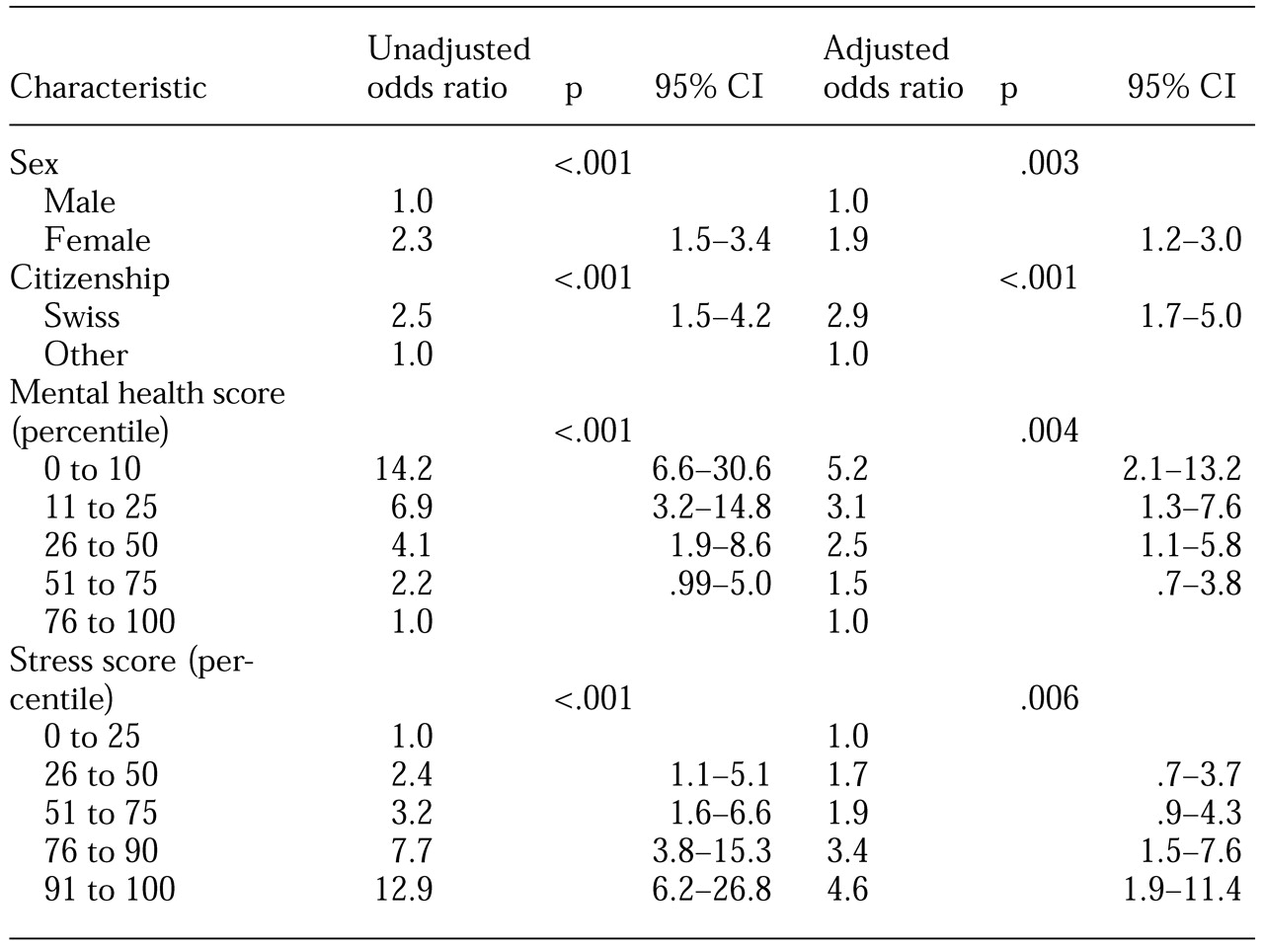
Data analysis
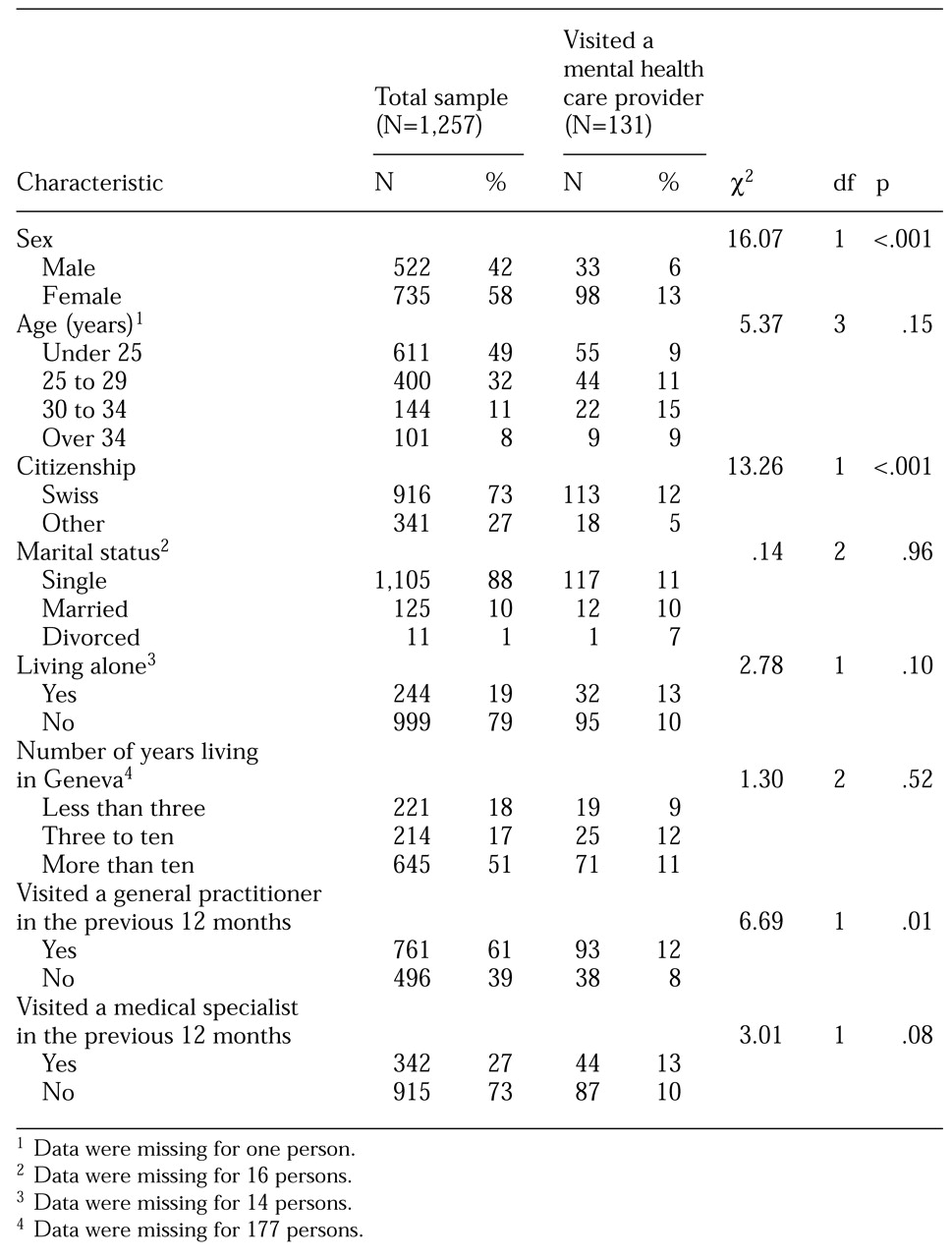
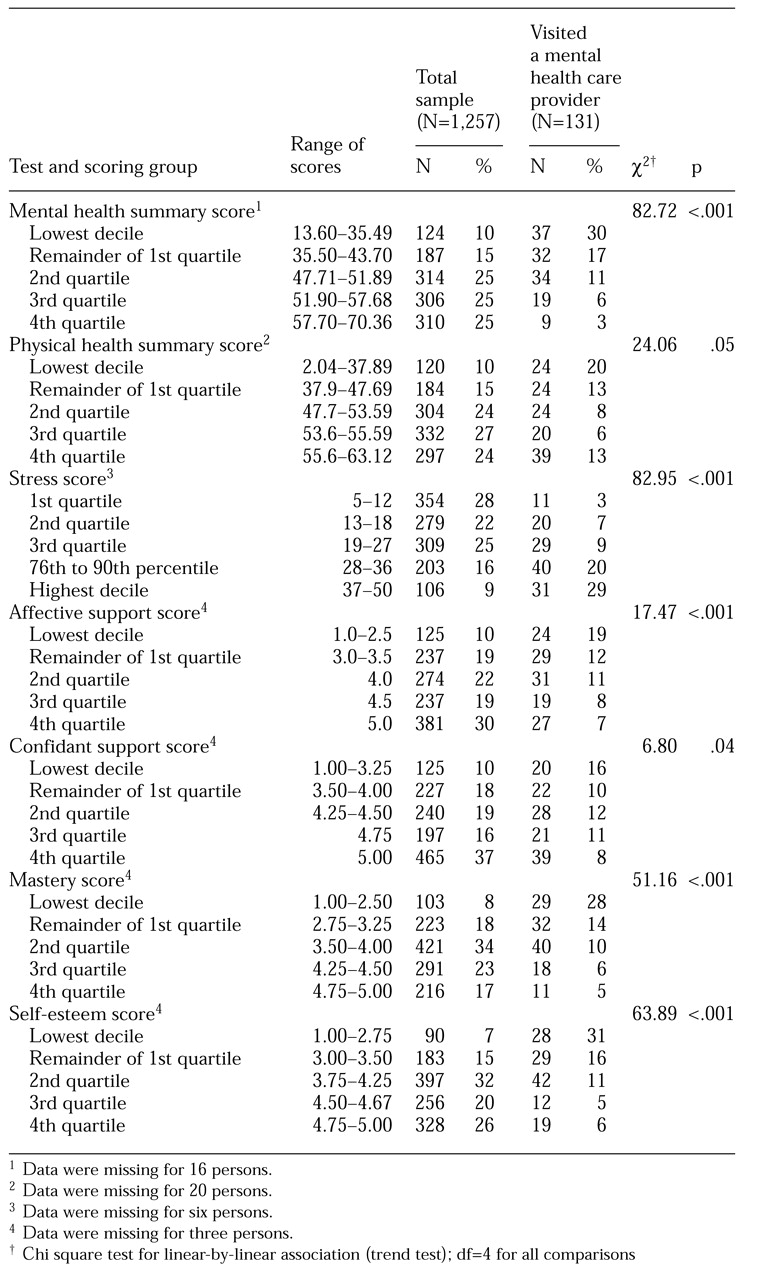
The mental and physical health and other psychological and sociodemographic characteristics of users of ambulatory mental health services were compared with those of nonusers. To examine the linearity of relationships, psychometric scores were split into five discrete levels: the lowest decile, the remainder of the first quartile (percentiles 11 to 25), and the second, third, and fourth quartiles. For stress, we isolated the highest decile, because high scores denote worse levels of functioning. Cross-tabulations and chi square tests were used for univariate analyses, and logistic regression was used to build multivariate models of mental health service use. A backward stepwise approach was used to identify the variables included in the final model. All statistical tests were two-tailed, with a significance level of .05.