A substantial proportion of the general population has unresolved grief and clinical complications after losing another person through death (
1). "Unresolved grief" refers to extremes in the intensity or duration of symptoms of grief—for example, prolonged anguish, prolonged preoccupation with the lost person, or a complete absence of reaction. Clinical complications include anxiety; depression; social, occupational, and familial dysfunction; health-compromising behaviors; and physical morbidity (
2,
3). In a review of epidemiologic studies, Jacobs (
1) concluded that about 20 percent of acutely bereaved individuals develop clinical complications. Because unresolved grief and clinical complications frequently co-occur, they are sometimes collectively referred to as complicated grief.
It is also estimated that the proportion of patients at general psychiatric outpatient clinics who have complicated grief is high. Accurate estimates are difficult to obtain, because patients usually do not cite loss as a reason for seeking treatment—losses and related problems emerge later in treatment (
4). Few studies have investigated the prevalence of loss and complicated grief among the wide range of patients who come to general psychiatric outpatient clinics. Most investigators have focused on specific samples, such as elderly bereaved spouses (
5,
6). Although such studies are important, they may inadvertently contribute to underestimation of the prevalence of loss and complicated grief among younger patients.
Two studies have focused on loss in a general psychiatric outpatient population. Zisook and colleagues conducted a 53-item questionnaire survey of 220 patients at intake (
7) and followed this up with a longer questionnaire survey of 1,000 patients (
8). In both studies, more than 40 percent of the patients reported experiencing the death of a first-degree relative or spouse and about 20 percent reported experiencing unresolved grief. The two studies were limited because they used only a single self-report item to generate a dichotomous classification of complicated grief—unresolved or resolved—and used nonstandard measures of depression.
Currently no standard definition or diagnostic criteria exist for pathological reactions to loss through death (
9). After reviewing the literature, we concluded that there was a need to study the prevalence of loss and complicated grief among patients at general psychiatric outpatient clinics, to include standard measures, and to consider the possibility of different levels of complicated grief.
We investigated the prevalence of loss through the death of another person and of complicated grief among patients at intake over the course of a year at two psychiatric outpatient clinics in the Vancouver area. A set of grief-specific measures as well as measures that were not specific to grief were used. Most of these measures were well-known standard dimensional measures of disturbance. On the basis of previous reports and our own experience, we expected that the prevalence of loss and complicated grief would be substantial and that we would be able to differentiate various levels of complicated grief.
Methods
Setting and patients
The study was conducted at two sites between June 1998 and February 2000. Site 1 was the psychiatric outpatient service of the psychiatry department of Lions Gate Hospital, a 300-bed community hospital in North Vancouver. Between 500 and 600 initial intake assessments are conducted each year by staff from the disciplines of psychiatry, social work, occupational therapy, and nursing. Patients are usually referred by health professionals—mostly general practitioners—in the community. Data were collected at this site between June 1, 1998, and May 31, 1999.
Site 2 was the outpatient psychiatry program at Vancouver General Hospital, a 900-bed university hospital. Between 300 and 400 initial intake assessments are conducted each year by staff from the disciplines of psychiatry, psychology, social work, and nursing. Patients are self-referred and are also referred by health professionals in the community. Data were collected at this site during the period of February 1, 1999, to January 31, 2000.
A total of 938 patients—548 at site 1 and 390 at site 2—registered for an intake interview. As part of routine procedures, the patients were asked to complete preintake questionnaires. A total of 862 patients (91.9 percent) complied with this request and were interviewed. A total of 729 patients (84.6 percent) were asked about losses through the death of another person as part of their regular intake interview. The other 133 patients were inadvertently not asked about loss. Emphasis was placed on the one or two most significant losses in each patient's life. The death of a parent, a partner, a child, a sibling, or a close friend was considered to be significant.
Of the 729 patients who were asked about loss, 403 (55.3 percent) reported experiencing one or more significant losses through death during their lives. Most of the 403 patients were informed about the study and were asked whether they would complete a set of postintake questionnaires that focused on their losses and their reactions. Patients whose mental state was too disturbed or who were unable to understand written English were not asked to participate. After a complete description of the study was provided, written informed consent was obtained from 235 patients (58.3 percent).
Representativeness of subsamples
The 729 patients who were asked about losses were compared with the 133 patients who were not asked on five demographic variables—age, sex, educational status, employment status, and marital status—and three disturbance variables—depression, anxiety, and general symptomatic distress. None of the results (chi square or t test) was significant. Similar comparisons were made between the 235 patients who completed the postintake questionnaires and the 168 patients who did not. Again, none of the test results was significant. Thus the patients who provided data were comparable with those who did not in terms of these demographic and disturbance variables.
Variables and measures
The preintake questionnaires measured indicators of disturbance that were not specific to loss. These questionnaires covered psychiatric symptoms and social (role) dysfunction. Depression was assessed with the 21-item Beck Depression Inventory (
10). Possible scores range from 0 to 63, with higher scores indicating higher levels of depression. Anxiety was assessed with the 20-item Trait Anxiety Scale (
11). Possible scores range from 20 to 80, with higher scores indicating higher levels of anxiety. General symptomatic distress was assessed with the global severity index of the 53-item Brief Symptom Inventory (
12). Possible scores range from 0 to 4.00, with higher scores indicating higher levels of distress. Social (role) dysfunction in six areas—work, social, extended family, partner, parent, and family unit—was measured with the 54-item Social Adjustment Scale- Self Report (
13). Possible scores range from 1 to 5, with higher scores indicating higher levels of dysfunction.
The postintake questionnaires measured loss-specific disturbance variables for each patient's one or two most significant losses. Intrusion was assessed with the seven-item subscale of the Impact of Event Scale (
14). Possible scores range from 0 to 35, with higher scores indicating higher levels of intrusion. Avoidance was assessed with the eight-item subscale of the Impact of Event Scale. Possible scores range from 0 to 40, with higher scores indicating higher levels of avoidance. Pathological grief was assessed by seven items developed by Prigerson and colleagues (
15). Possible scores range from 0 to 21, with higher scores indicating higher levels of pathological grief. Grief was assessed by the 13-item present feelings subscale of the Texas Revised Inventory of Grief (
16). Possible scores range from 13 to 65, with higher scores indicating higher levels of grief.
We used two variables—intrusion or avoidance, and social dysfunction—to differentiate between two levels of complicated grief—moderate and severe. In addition, a minimum period since the loss—three months—was required for a patient to meet the criteria for complicated grief. Use of these three variables ensured that any disturbance we observed included both loss-specific symptoms and social dysfunction and was not an immediate grief reaction. The focus was on the most troublesome loss.
To be categorized as having moderate complicated grief, a patient had to attain a score of 10 or above on the intrusion or avoidance subscale and a score of 2 or above on one of the six areas of the Social Adjustment Scale-Self-Report, in addition to meeting the criterion of at least three months since the loss. These criteria were selected, after a review of the studies that used these measures, to include patients with symptoms of at least moderate grief, social (role) dysfunction, and sufficient time since the loss. To be categorized as having severe complicated grief, a patient had to attain a score of 20 or above on the intrusion or avoidance subscale and a score of 3 or above for one of the six areas of the Social Adjustment Scale-Self-Report, again in addition to meeting the criterion of at least three months since the loss. The remaining patients were categorized as having minimal disturbance.
Results
The 235 patients who completed the postintake questionnaires received DSM-IV diagnoses that were determined jointly by an intake interviewer and a psychiatrist. Almost all the patients—230, or 98 percent—received an axis I diagnosis. The most frequent primary diagnoses were major depression (117 patients, or 50 percent), dysthymia (42 patients, or 18 percent), substance abuse (35 patients, or 15 percent), and bipolar disorder (26 patients, or 11 percent). A total of 115 patients (49 percent) received one or more axis II diagnoses. The most frequent of these diagnoses were obsessive-compulsive personality disorder (47 patients, or 20 percent), dependent personality disorder (35 patients, or 15 percent), and borderline personality disorder (14 patients, or 6 percent).
The mean±SD age of the patients was 42.2±11.9 years (range, 18 to 82 years), and 134 patients (57 percent) were women. Racial data are not available, because the outpatient clinics studied do not record this information. A total of 202 patients (86 percent) had at least a high school education, and 125 (53 percent) were employed. Eighty patients (34 percent) lived with a partner, 71 (30 percent) were separated or divorced, 12 (5 percent) were widowed, and 73 (31 percent) had never been married.
Prevalence of significant loss
The 235 patients who completed postintake questionnaires had experienced an average of 2.9 significant losses during their lives. The types and proportions of the most troublesome losses were the death of a parent (110 patients, or 47 percent), a friend (33 patients, or 14 percent), a grandparent (23 patients, or 10 percent), a sibling (14 patients, or 6 percent), a partner (nine patients, or 4 percent), a child (seven patients, or 3 percent), or other (38 patients, or 16 percent). The mean±SD time since the loss was 10.4±9.7 years.
Moderate complicated grief
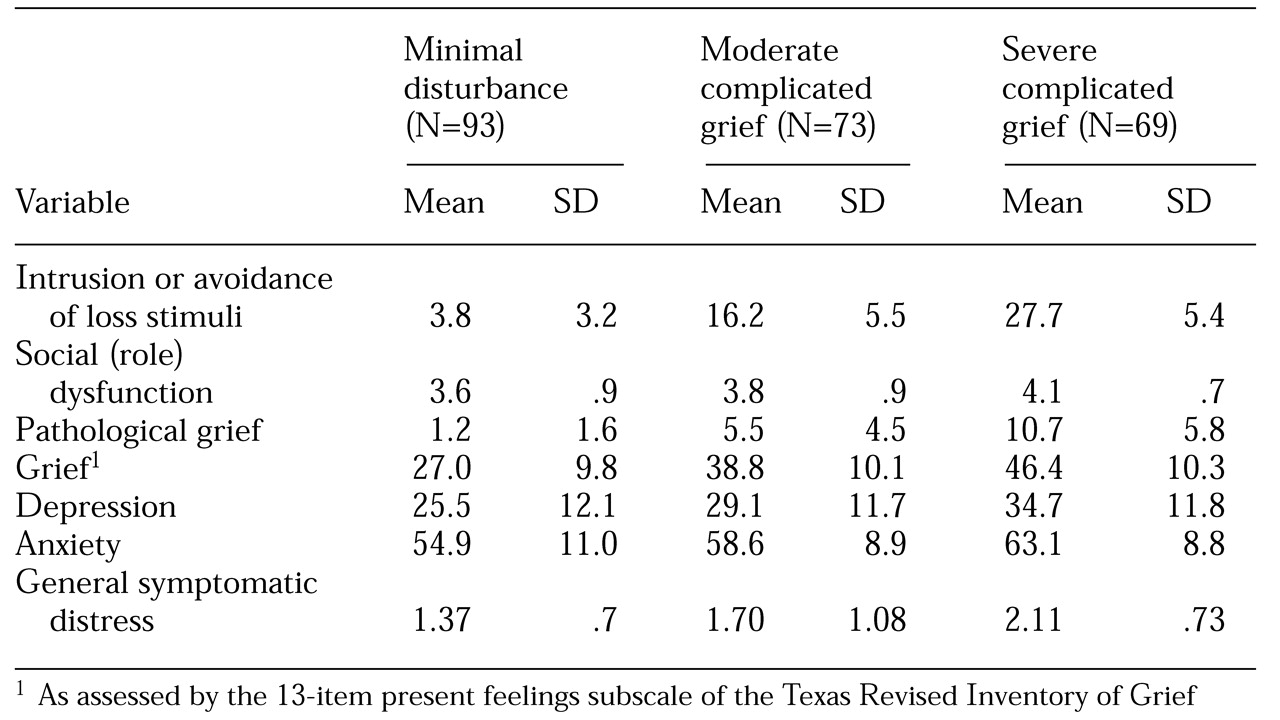
Of the 235 patients who completed the postintake questionnaires, 73 (31 percent) met the criteria for moderate complicated grief. These patients had experienced a mean±SD number of significant losses through the death of another person of 2.7±1.7. As indicated in
Table 1, their average scores were well above the minimum for moderate complicated grief. These patients' scores on the disturbance variables that were not specific to loss were also considerably elevated. The mean±SD time since the most troublesome loss was 10.6±10.1 years.
Severe complicated grief
A total of 69 patients (29 percent) met the criteria for severe complicated grief. These patients had experienced a mean±SD number of significant losses through death of 2.9±1.6. Their average scores were well above the minimum for severe complicated grief. According to reported norms (
10,
11,
12), these patients' scores on variables that were not specific to loss were high compared with those of other outpatients. The mean±SD time since the most troublesome loss was 8.4±9.1 years.
Disturbance variables
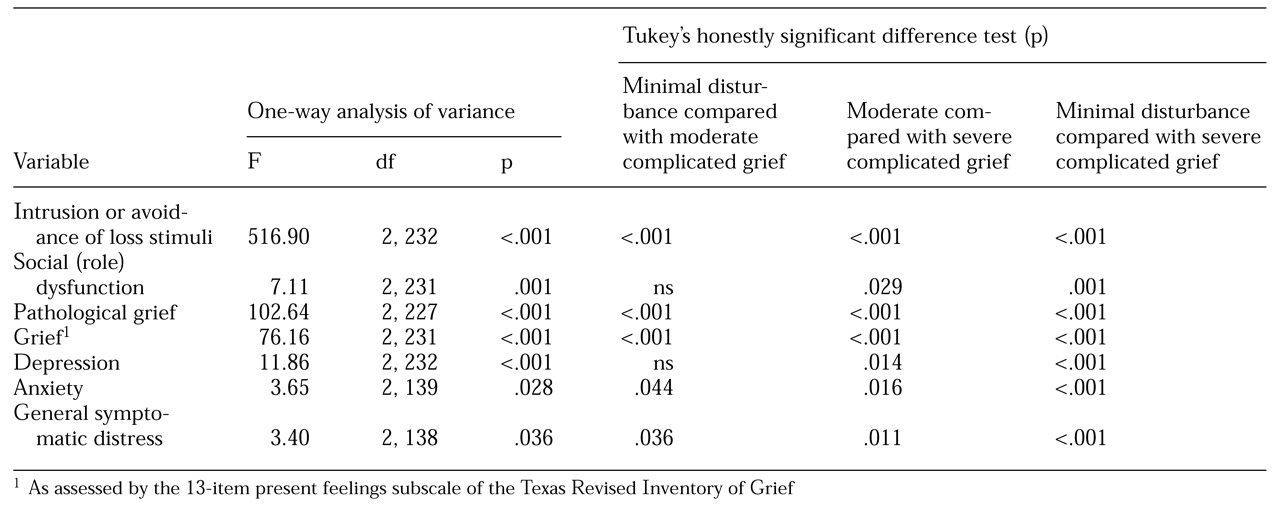
For the three groups, the seven disturbance variables listed in
Table 1 were compared. The result of a one-way multivariate analysis of variance for the set of seven variables was significant (Pillai's trace=.853, F=23.16, df=14, 436, p<.001). As indicated in
Table 2, the results of all seven corresponding univariate analyses of variance were significant. A multiple comparison test—Tukey's honestly significant difference test—was conducted for each pair of groups within each analysis of variance. For five variables—highest intrusion or avoidance, pathological grief, grief, anxiety, and general symptomatic distress—each group had significantly different scores from the other two: patients who had minimal disturbance had lower scores than those who had moderate complicated grief, who in turn had lower scores than those who had severe complicated grief. In addition, for two variables—social dysfunction and depression—the scores of the patients who had severe complicated grief were significantly higher than those of the patients who had moderate complicated grief or minimal disturbance. Because the highest levels of intrusion or avoidance and social dysfunction were used to define the three groups, it is not surprising that the groups differed significantly on these variables.
Variables not specific to loss
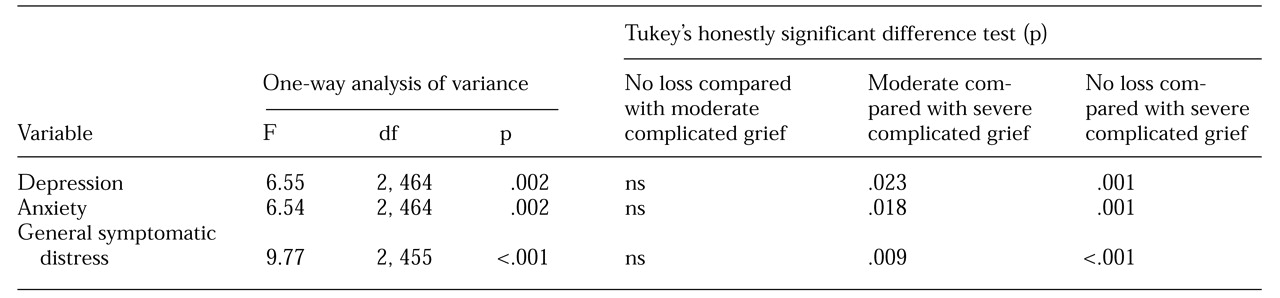
Three disturbance variables that were not specific to loss—depression, anxiety, and general symptomatic distress—were compared for patients who had moderate complicated grief, patients who had severe complicated grief, and the 326 patients who had not experienced a significant loss through the death of another person. For patients who had experienced no significant losses through death, the means±SDs for the three variables were 28.7±13.1, 58.4±10.3, and 1.62± .78, respectively. (Data for the groups with moderate or severe complicated grief are shown in
Table 1.) The result of a one-way multivariate analysis of variance for the set of three variables was significant (Pillai's trace=.045, F=3.46, df=6, 904, p<.002). As shown in
Table 3, the results of the corresponding three univariate analyses of variance were also significant. Tukey's test was again conducted for each pair. For each variable, the scores of the group with severe complicated grief were significantly higher than those of the other two groups.
Complicated grief in the entire sample
By multiplying the prevalence of significant loss through death (55.3 percent) by the prevalence of a specific level of complicated grief—for example, 31 percent for moderate complicated grief—it is possible to obtain an estimate of the proportion of patients who manifest that level of complicated grief in the entire outpatient sample. Using this method, we estimated that of all the patients who sought services at the two outpatient sites, 160 patients (17.1 percent) met the criteria for moderate complicated grief and 152 patients (16.2 percent) met the criteria for severe complicated grief. Thus 312 patients (33.3 percent) met or exceeded the criteria for moderate complicated grief.
Discussion
This exploratory study investigated the prevalence of loss and complicated grief among a large number of patients who sought services in two outpatient psychiatry departments—one in a suburban community hospital and the other in an urban university hospital. In contrast with many studies of loss through the death of another person, our sample was not elderly: the patients' average age was 42. The most frequent losses involved parents, grandparents, and friends rather than partners or children. More than 55 percent of the sample had experienced one or more losses through death; the average was nearly three losses.
Two levels of complicated grief—moderate and severe—were defined on the basis of loss-specific symptoms, social dysfunction, and time since the loss. Patients who did not meet the criteria for complicated grief were categorized as having minimal disturbance. In general, the three groups were well differentiated in terms of loss-specific variables, social dysfunction, and variables not specific to loss. The level of disturbance among those with severe complicated grief was high.
Furthermore, when patients who had severe complicated grief were compared with patients who had not experienced the loss of another person, they were found to have significantly higher levels of depression, anxiety, and general symptomatic distress. Simply experiencing a loss through death was not in itself associated with higher levels of these conditions. Only patients who had a severe level of complicated grief had significantly more severe symptoms. This finding supports the need to distinguish among levels of complicated grief. The data suggest that a sizable proportion of the entire outpatient sample met or exceeded the criteria for moderate complicated grief. Also notable was the considerable amount of time that had elapsed since the losses, which indicates that these patients had long-term complicated grief.
Our findings agree with those of the two earlier surveys of Zisook and colleagues (
7,
8). First, the age of the patients—adult but not elderly—and the most prevalent types of losses—those involving parents and grandparents—were similar. Second, the prevalence of loss was substantial in both of those studies, and it was even higher in our study. Third, loss by itself was not necessarily related to higher levels of disturbance that is not specific to loss, such as depression. Finally, the average length of time since the loss—about ten years—was considerable in both studies. Our study extended the results of these earlier surveys by using more comprehensive and standard measures of disturbance, assessing patients at two different sites, and distinguishing among various levels of complicated grief.
Given the lack of a standard definition or diagnostic criteria for complicated grief, it is difficult for clinicians and researchers to know whether they are dealing with healthy or pathological reactions to loss. If their criteria are too lenient, they run the risk of overemphasizing psychopathology; if their criteria are too strict, they run the risk of depriving patients of useful treatment. Distinguishing among different levels of disturbance might be more helpful than using a strict cutoff for complicated grief. Clinicians can consider different levels in making treatment plans, and researchers can use different levels of complicated grief in investigating the causes and treatment for it.
The two levels of complicated grief used in this study were based on three criteria—intrusion or avoidance of loss stimuli, social dysfunction, and time since loss. Future work may show that other levels or criteria lead to better differentiation and prediction of important clinical events, such as prognosis and response to treatment.
The strengths of our study include the fact that a large number of outpatients from two different sites were studied over one year, that a large proportion of eligible patients were asked about losses as part of routine procedures, and that a set of standard measures of disturbance—variables specific to loss and variables not specific to loss—was used.
The limitations of the study include the fact that not all patients who registered for intake were asked about losses and that not all patients who had experienced significant losses completed the postintake questionnaires. Nevertheless, comparisons between patients who provided data and those who did not revealed that the patients were comparable in terms of demographic and disturbance characteristics. In addition, the sample was limited to patients who functioned well enough to seek outpatient services; the prevalence of loss and complicated grief may be even higher among patients who are unable to seek such services.
The patients, all from the Vancouver area, were mostly white, although the population in this area is ethnically diverse. The findings may not be generalizable to cities with different racial compositions. Finally, the study did not include a control group consisting of people in the general population who did not seek psychiatric services. Comparisons that include such a control group would be informative.
Conclusion
Clinicians should systematically assess patients for loss and complicated grief on a routine basis, because most patients do not initially complain about loss. Although the loss of a child or a spouse is often regarded as the most stressful type of loss, our study showed that the loss of another person, such as a parent, a grandparent, or a friend, can be troublesome for long periods.
These losses should be considered as possible etiologic factors in the management of all psychiatric outpatients. Furthermore, losses need to be addressed in treatment—through therapies that are specifically designed for patients who have experienced a loss (
17) and through the many therapies that are not so designed. In the case of these nonspecific therapies, knowledge about high prevalences can sensitize therapists so that they can respond to indirect references to losses and inquire about losses in the absence of such references. In addition, nosologists who revise standard classification systems for mental disorders, such as the
DSM, should formulate a clear status for complicated grief that differs from the current ambiguous one (
18).
Several areas would benefit from future research. Examining the importance of specific symptoms of grief and comparing them with specific symptoms of disorders such as depression would be informative. Further study of the association between various psychiatric disorders and complicated grief may reveal causal sequences and suggest differential treatments.
Finally, the large number of patients who met the criteria for complicated grief in our study suggests the need for cost-effective interventions. Given that time-limited, short-term group therapies are among the most cost-effective forms of therapy (
19,
20), investigation of their usefulness in addressing complicated grief is warranted. Our own work with time-limited, short-term group therapy for patients with complicated grief has produced promising results (
21,
22). The results of this study suggest that such groups could be offered to an even larger number of patients.
Acknowledgment
The research project was supported by grant MT-13481 from the Medical Research Council of Canada in Ottawa.