Assertive community treatment and intensive case management are two forms of community care for helping people with severe mental illness achieve optimal levels of integration into the community. The two approaches have many characteristics in common: both serve clients who are in great need of intensive assistance, both serve clients in community settings, and both focus on practical issues, such as medications, housing, and finances. However, the approaches have evolved differently.
The program elements of the assertive community treatment model were clearly conceptualized by the model's developers from its inception (
1). Assertive community treatment is recognized as an evidenced-based practice (
2). Twenty-five controlled studies have suggested that it is effective in reducing hospital use, increasing housing stability, controlling psychiatric symptoms, and improving quality of life (
3).
By contrast, intensive case management does not represent a single well-defined program model but rather encompasses various case management practice orientations that are more intense than conventional case management. Some observers, such as Rapp (
4), have emphasized the commonalities between intensive case management and assertive community treatment and have noted that proponents of each model often overstate differences between the two. However, others have concluded that intensive case management and assertive community treatment differ in both conceptualization and client outcomes (
5,
6).
One common means of identifying the critical ingredients of a program model is the use of panels of experts. Surveys of experts have been used for this purpose for both assertive community treatment (
7) and intensive case management (
8). The study reported here was a secondary analysis that capitalized on the shared methods and content of these two surveys. It addressed two questions. First, how similar are assertive community treatment and intensive case management? Second, are there distinctive elements found in one but not in the other?
Methods
During 1992 and 1993, a structured telephone interview of 20 national experts was used to identify critical ingredients of the assertive community treatment model (
7). Respondents rated the importance of a list of 73 potentially critical program elements. For 16 of these items, respondents also indicated ideal model specifications—for example, an ideal caseload ratio.
Schaedle and Epstein (
8) conducted a mail survey of 22 experts in intensive case management. These experts were selected on the basis of contributions to the published literature on intensive case management. Three stakeholder groups were studied: experts, program managers, and case managers. However, in the analysis reported here we examined only the sample of 22 experts. An 80-item survey instrument was developed. The instrument contained 40 items that were identical to items on the assertive community treatment instrument and 40 additional items, derived from a literature review, that were specific to intensive case management. Respondents rated the importance of each item. For 12 of the items, the respondents also indicated ideal model specifications.
Importance ratings for both instruments were based on an identical 7-point Likert scale ranging from 1, very unimportant, to 7, very important. The items were grouped into seven sections: personnel structure; other structural and organizational components; engagement, retention, and discharge; hospitalization and coordination of services; treatment goals and foci; service elements; and client characteristics. Univariate t tests were used to test differences between the two groups of experts. Effect size for the difference between samples also was calculated.
Results
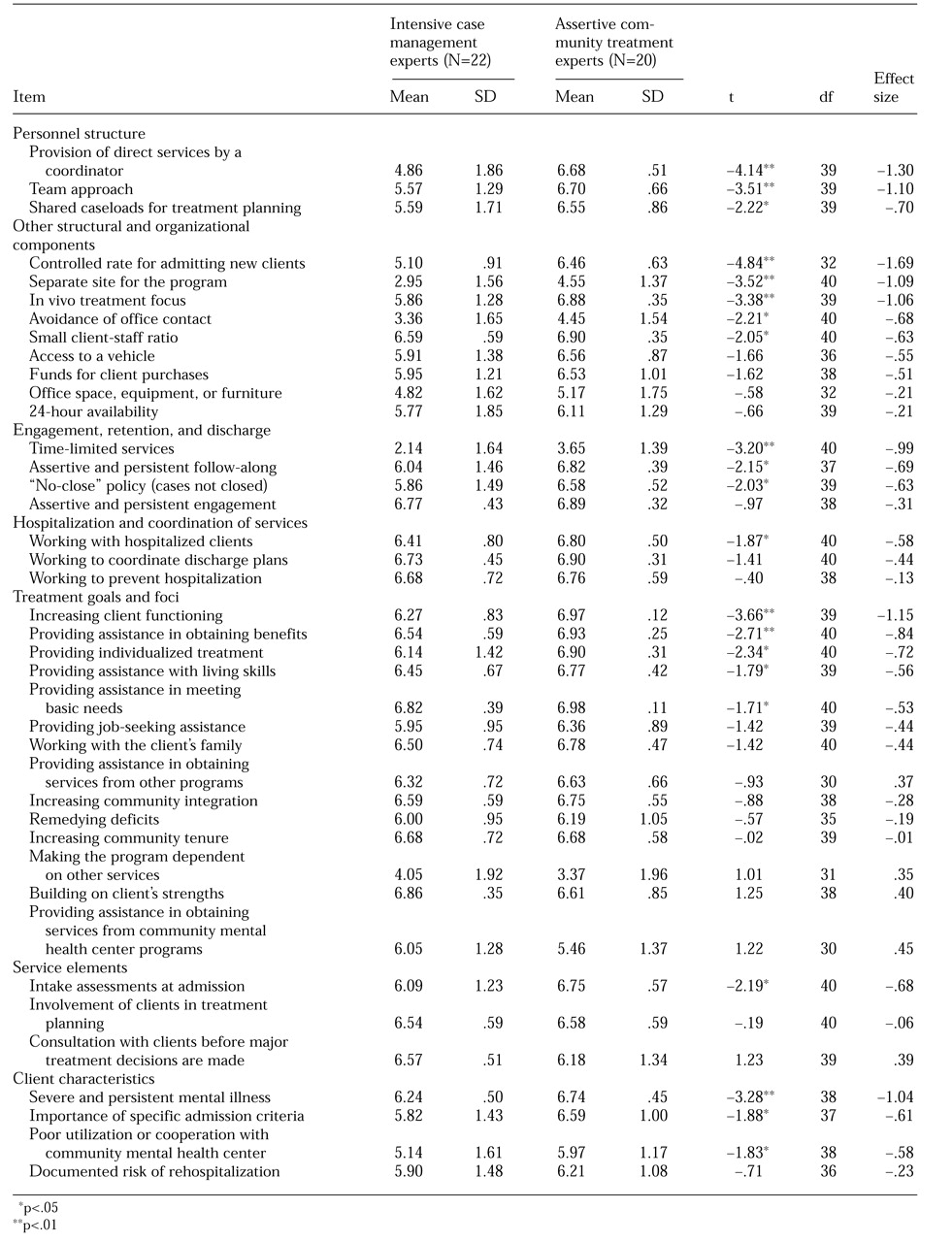
The overall mean rating of importance for the 40 items common to both survey instruments was 6.3 for the assertive community treatment group and 5.8 for the intensive case management group. As shown in
Table 1, the assertive community treatment experts gave higher importance ratings than the intensive case management experts to most items; significant differences were observed for 21 items. All items for which there were significant differences between the two groups received higher ratings from the assertive community treatment experts than from the intensive case management experts.
When specific subgroups of items were examined, significant differences between the two groups in importance ratings were observed for all three items related to personnel structure: provision of direct services by a coordinator, a team approach to treatment delivery, and shared caseloads for service provision. Three of the four items related to engagement and retention received significantly different ratings. Having a "no-close" policy—that is, a policy not to close cases—and assertive, persistent follow-along received higher ratings from the assertive community treatment experts than from the intensive case management experts, although both groups rated these items as important. The experts disagreed on the importance of time-limited services, but only on the degree of unimportance.
Significantly different ratings were assigned to five of nine items related to organization and structure. The assertive community treatment experts placed greater emphasis on admitting new clients at a controlled rate and having an in vivo treatment focus. A small difference was found between groups in ratings of the importance of a small client-staff ratio, but this difference was not considered meaningful, because both groups rated this item as very important.
For eight of 14 items related to treatment goals, no significant differences in ratings were observed between the two groups. Of the items for which significant differences were found, all were rated as important by both groups. One item pertaining to service elements and three of four items pertaining to client characteristics received higher ratings from the assertive community treatment experts than from the intensive case management experts.
The intensive case management experts gave higher ratings to only three of the 40 items that were common to both instruments: providing assistance in obtaining services from community mental health center providers, building on client strengths, and consulting clients before major treatment decisions are made. These differences were not statistically significant.
Differences in ideal model specifications were found for three items. The intensive case management experts endorsed slightly higher ideal caseload ratios than the assertive community treatment experts (12:1 and 10:1, respectively). The assertive community treatment experts suggested twice as many team meetings per week as the intensive case management experts. They also suggested an optimal period for attempting to engage a reluctant client that was more than twice as long as that suggested by the intensive case management experts (15.5 months and 5.5 months, respectively).
Discussion
The purpose of this study was to identify features that differentiate assertive community treatment from intensive case management. We had expected that several features of each approach would be viewed as more important by one group of experts than by the other. Instead, we found that the assertive community treatment experts gave almost all elements a higher rating of importance than the intensive case management experts.
One interpretation of this finding is that assertive community treatment is more clearly articulated than intensive case management, and as a result experts are more confident about its critical ingredients. According to this interpretation, intensive case management shares many critical ingredients with assertive community treatment, but the elements are not as clearly articulated. In other words, intensive case management may not represent a distinct program model but rather mirrors assertive community treatment, although in a less strongly held set of principles.
We discovered several areas in which assertive community treatment differs from intensive case management, primarily elements pertaining to organization and structure. Some observers have suggested that the main features that distinguish assertive community treatment from intensive case management have to do with assertive community treatment's emphasis on a team approach, a difference observed in one study that compared the implementation of the two models (
9). The assertive community treatment experts in our study affirmed the importance of a multidisciplinary team that shares caseloads and meets frequently, whereas the intensive case management experts rated teamwork as much less important, reflecting a critical difference in practice between the two models: intensive case management involves individual caseloads, whereas assertive community treatment does not.
The experts' ratings suggested that assertive outreach plays a greater role in assertive community treatment than in intensive case management. Our findings suggest that there is a greater level of tolerance for closing cases in intensive case management than in assertive community treatment. Although intensive case management experts generally rated a no-close policy as important, they also indicated circumstances under which clients should be discharged, namely, when psychiatrically stable clients refuse services and when clients are readmitted for long-term hospitalization or incarceration.
Our findings also corroborate the view that assertive community treatment mirrors the medical model of care in which psychiatrists and nurses have critical roles (
10). The assertive community treatment experts conceptualized this model as a comprehensive treatment and rehabilitation approach that does not broker services. By contrast, the distinctive features of intensive case management revolve around its roots in case management practices, with an emphasis on client strengths (
4). The primary function of intensive case management is to link and coordinate services. Accordingly, the intensive case management experts strongly endorsed client empowerment items, such as building on client strengths, increasing community integration, and consulting clients before major treatment decisions are made.