Clients' participation in addressing their health and mental health care needs is a key element of health care practice (
1). Services provided by client-run self-help agencies have become essential components of mental health care (
2,
3,
4), and self-help agencies are increasingly accountable for client outcomes (
5,
6,
7,
8). Given that little attention has been paid to determinants of outcomes for clients of self-help agencies, we looked at the relationship between such outcomes and attendance at the agency, client satisfaction with the agency, organizationally mediated empowerment—that is, involvement in decisions about one's own services and the way the organization delivers services—and psychological disability. The outcomes assessed were independent social functioning, assisted social functioning, and personal empowerment.
Although self-help agencies vary considerably in character, the agencies we studied reflect the goals and aspirations of the early leaders of the self-help movement who founded them. These self-help agencies have been funded by the Substance Abuse and Mental Health Services Administration and various foundations partly because they are organized around the original principles of this movement. First, the people who use the services also run them and make all decisions—the service providers and recipients are one and the same. Second, these groups strive to share power, responsibility, and skills and endorse a nonhierarchical structure in which people reach across to each other rather than up and down a hierarchy. Third, client-run programs are based on choice: they are totally voluntary. Finally, the programs are based on a nonmedical approach to treating disturbing behavior, and they address the economic, social, and cultural needs of clients (
9).
The principles of empowerment through shared governance and the focus on ability rather than disability are central. Self-help agencies offer mutual support groups, drop-in space, survival resources, and direct services, including food, assistance with temporary shelter and permanent housing, financial benefits, counseling and advocacy, job counseling, substance abuse counseling, money management counseling and payeeship services, case management, peer counseling, information, and referral. Most paid staff members who are not former clients of the program have had life experiences of poverty, homelessness, and institutionalization that are similar to those of clients. Volunteer jobs provide clients with opportunities to help others in material ways, such as serving food and distributing clothing; to obtain a work history; and to participate in organizational decision making.
The ideology and service package of self-help agencies distinguish the types of outcomes we examined in this study and were the basis for specifying factors that could determine such outcomes. Self-help agencies offer a strengths-based approach that focuses on promoting personal empowerment or greater control over one's life situation, independent social functioning, and assisted social functioning. Whereas mental health professionals emphasize independent and assisted social functioning, clients of self-help agencies emphasize the ability to participate in the community as a result of having greater control over their own situation and a better ability to command the help of others. The outcome goals are the same (
7,
8,
9,
10,
11).
Self-help agencies try to achieve these outcomes by creating a more hospitable and respectful and less stigmatizing—and thus more accommodating—environment. Whether clients use a disability model or a recovery model, there is a common emphasis on providing a community that accepts and values the person (
12). Through the self-help agency, clients gain resources, skills, and contacts. They also learn to redefine their disability as something that is not necessarily an impediment. Thus attendance at the agency becomes a mechanism for increasing personal empowerment and improving one's ability to function outside the agency, either individually or through better use of personal and professional relationships.
Increasing clients' involvement in organizational decisions about how services are delivered—known as organizationally mediated empowerment and long hypothesized to be a key factor in client outcomes (
13,
14)—has been a motivating force in the development of self-help agencies (
7). Clients are given an active role in running the agencies. At community meetings, the entire membership is given authority over important policy decisions, including decisions about staffing, services offered, and agency rules. Governing boards are elected by clients, and a majority of board members are clients. When clients break rules, decisions about what actions should be taken are made either by elected committees or by the agency's entire membership. These procedures empower clients and minimize hierarchy within the agency, despite the exigencies of maintaining organizational structures (
7). The exercise of this decision-making power is thought to translate to other areas of clients' lives, resulting in greater control over their life situation and better social functioning (
15,
16).
Client satisfaction is the most widely assessed outcome among users of mental health services. Moreover, dissatisfaction with traditional mental health services is one of the major reasons for the development of self-help agencies. Self-help agencies seek to improve satisfaction by involving clients in the helping process. The assumption—although not consistently supported in the literature (
17)—is that satisfaction with the self-help agency, or at least reduced dissatisfaction, will foster more personal commitment to the helping process and thus will be associated with better outcomes.
Self-help agencies often differ in the degree to which they accept the disease concept of mental illness. However, most agencies agree that an individual's psychological disabilities or problems may impede the person's ability to function and may be disempowering. Self-help agencies assume that their efforts will help control the negative effects of mental disabilities through environmental accommodations and thus improve social functioning.
This study is the first to empirically evaluate the relationship of the hypothesized determinants of client outcomes in self-help agencies to the actual experiences of agency clients. We evaluated these relationships over six months, taking into account the clients' baseline status and other possible confounding influences. The study was part of a larger investigation of users of mental health self-help agencies and organizations (
18,
19,
20,
21,
22).
Methods
Subjects
The participants were long-term users of four self-help agencies in the San Francisco Bay Area. We surveyed the entire staff—who were themselves clients, all volunteers—and a sample of nonstaff clients. We selected clients randomly from those who had attended the self-help agency at least 12 times during the previous three months and who were present in the drop-in center when an interviewer was available. This approach ensured that study participants had had a minimum level of exposure to the agency and were not casual visitors. The interviewers were former mental health clients as well as mental health professionals. They went to the self-help agencies at different times on different days, with no consistent schedule. Data were gathered in 1992 and 1993. Human subjects protection procedures were approved by the University of California, Berkeley, campus committee for the protection of human subjects and a similar committee of the Public Health Institute.
Of the 321 baseline interviews attempted, 310 (97 percent) were completed. All statistics are based on a sample of 255 participants (82 percent) who were interviewed both at baseline and at six months. None of the participants who could be located at six months refused a follow-up interview. On the basis of the records that were available at two of the four self-help agencies, no significant differences in age, sex, or diagnosis were observed between our sample and the total clientele of the agencies.
Measures
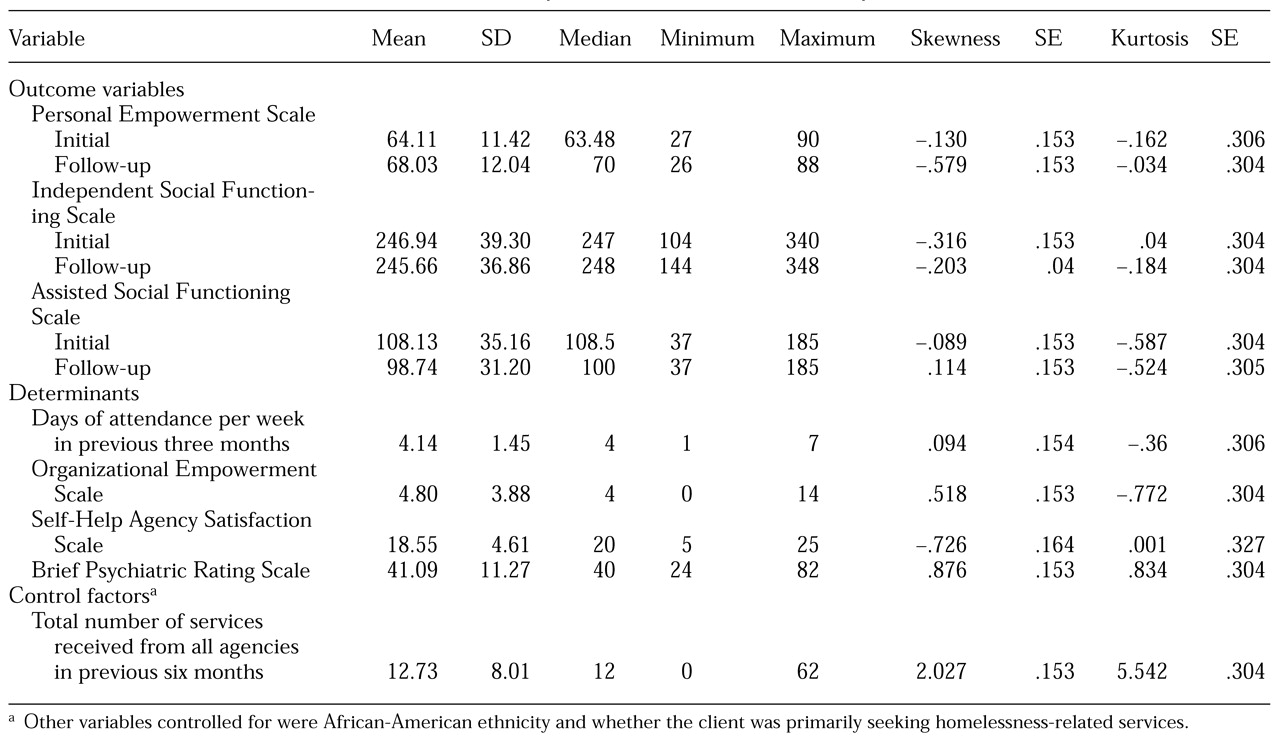
Scales and items were selected on the basis of discussions between consumer leaders—both members and nonmembers of the agencies studied—and researchers as well as observations made at the self-help agencies during the course of a year. A panel of researchers and consumers refined the items that were used to measure organizational and personal empowerment and satisfaction with the self-help agencies. Summary statistics for all the measures are listed in
Table 1 along with statistics indicating the measures' conformity with measurement requirements of the proposed structural modeling.
Outcomes
The Personal Empowerment Scale (PES) (
19) contains 20 items that measure control over common life domains, including shelter, income, service provision, and an individual's ability to minimize unwanted occurrences, such as personal danger and homelessness. Possible scores range from 20 to 100, with higher scores indicating greater empowerment. This scale had an internal consistency (alpha) of .84 at baseline and .85 at follow-up and a stability coefficient (r) of .49.
The Independent Social Functioning Scale (ISFS) (
23,
24) contains 59 items that measure "the extent to which an individual participated in and made use of the community in a self-initiated manner and without the help of others." The ISFS measures the amount of time spent in community-related activities; the ease with which a person engages in social contacts, uses community services, and obtains basic resources; the amount of contact with family, friends, and acquaintances; involvement in income-producing activities or educational activities that might lead to employment; and the amount of time spent in purchasing activities, such as shopping. Possible scores range from 74 to 370, with higher scores indicating better functioning. The ISFS's internal consistency was .94 at baseline and .95 at follow-up; its stability coefficient was .58.
The Assisted Social Functioning Scale (ASFS) (
23,
24) contains 37 items that measure the types of community involvement covered in the ISFS. The scale assesses whether each behavior is in some way assisted by a friend or helper. Possible scores range from 37 to 185, with higher scores indicating better functioning. The scale's internal consistency was .97 at baseline and .97 at follow-up; its stability coefficient was .49.
Determinants
Attendance was measured as the client's average number of contact days at the self-help agency per week during the three months before the interview. This variable was normally distributed, with a range of one to seven days.
The Organizational Empowerment Scale (OES) (
19) is distinct from the PES in that it considers members' experiences as being structured by the organization of the agency. Conceptually, the scale draws from the Levi Strauss Company's definition of organizational power as an effort that increases the authority and responsibility of those in the organization. It measures the discretion exercised by an individual in carrying out tasks within the organization and the power of the individual to mobilize scarce resources within the organization. This 17-item scale assesses the actual exercise of responsibilities within the organization that can empower the individual with the skills necessary to make responsible decisions in his or her own life.
Items from the scale address formal participation, such as voting for officers or serving as an officer or a board member; use of discretion, as in helping organize a meeting or planning a meal; the commitment of resources, as in participating in an employee or volunteer recruitment process or selecting activities for members of the self-help agency; and defining situations, as in establishing agency rules. Possible scores range from 0 to 17, with higher scores indicating greater participation. The internal consistency of the scale was .87 at baseline and .90 at follow-up; its stability coefficient was .62 (
13).
The five-item involvement subscale of the Self-Help Agency Satisfaction Scale (SHASS) measures member satisfaction with decisions about services, activities, rules, the process of making suggestions, and access to jobs at the self-help agency. Possible scores range from 5 to 25, with higher scores indicating greater satisfaction. The internal consistency of the scale was .87 at baseline and .91 at follow-up; its stability coefficient was .44. Discriminant validity was established through factor and cluster analyses with quality-of-life satisfaction scales and supported the hypothesis that the SHASS subscale we used represents a distinct construct, different from indicators of general life satisfaction (
25).
The Brief Psychiatric Rating Scale (BPRS), which measures current psychological disability, is a frequently used symptom-based index (
24,
25,
26,
27). We used training films and dictionaries to standardize assessments of symptom ratings. Interviewers were trained to complete an expanded 24-item version of the BPRS. Possible scores ranged from 7 to 168, with higher scores indicating greater severity of symptoms. Interrater reliabilities were around .9 during the training; internal consistency was .79 at baseline and .74 at follow-up; the stability coefficient was .49.
Control factors
African-American ethnicity versus other ethnicity—coded as 1 and 0, respectively—was selected as a control for the purpose of generalizability, given the high proportion of African-American clients served by the agencies. To address the unique contribution of self-help agencies to client outcomes beyond the concrete services that might be offered in any context or by trained professionals, we included a control for clients' total service use in the six months before the baseline period. The total service use score records the receipt of 25 different services—for example, support, advocacy, vocational services, housing assistance, help with living skills, and social activities—from four sources: a social service agency, a mental health center, a self-help agency, or any other agency. Possible scores range from 0, indicating that no services had been received from any source, to 100, indicating that all services had been received at all settings.
Finally, we controlled for clients who were primarily seeking homelessness-related services at the self-help agency, which is an indicator of limited program involvement—for example, such persons might show up once a week to take a shower. Cases were coded 1 if clients were primarily seeking homelessness-related services and 0 if they were seeking other services.
Statistical methods
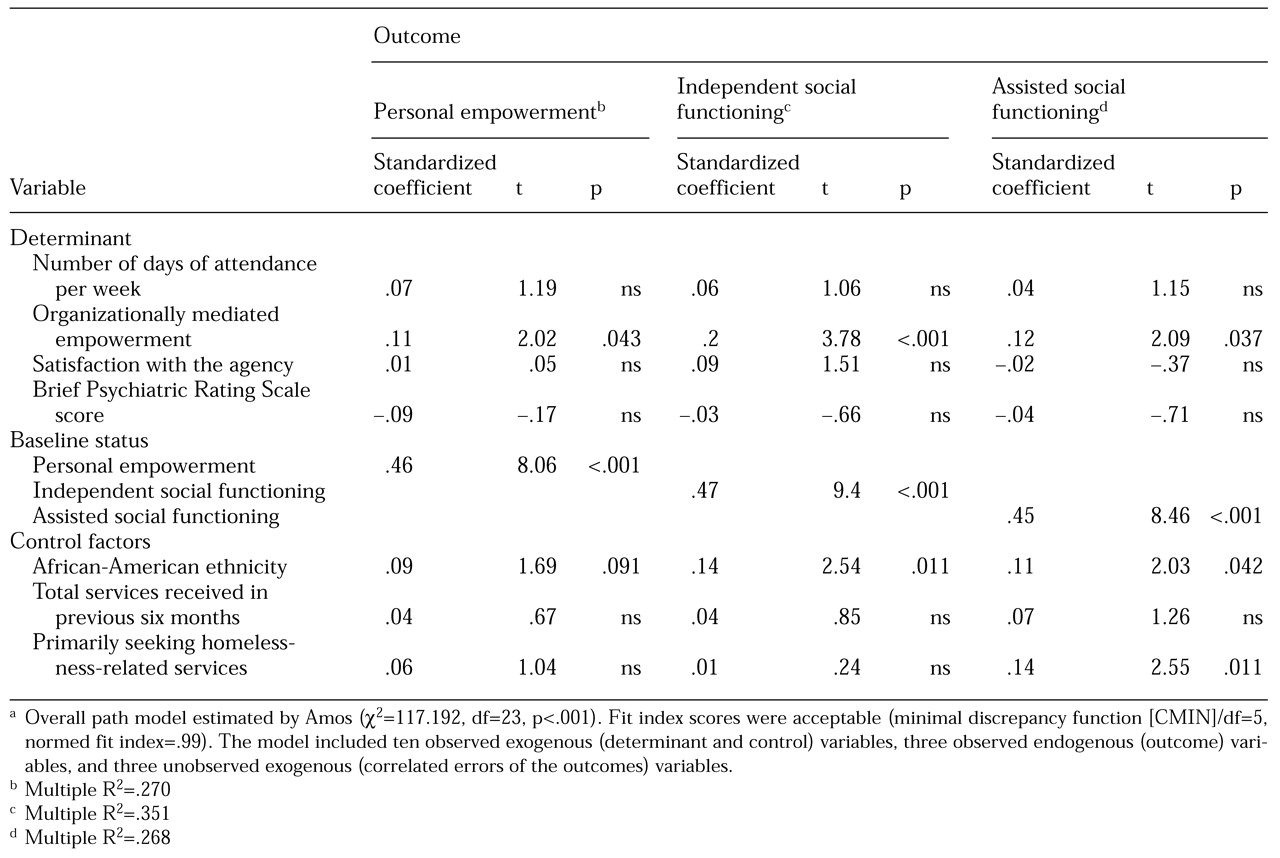
We conducted univariate descriptive analyses and paired-sample t tests that described changes in outcomes. The relationship between each of the four determinants and the three outcomes—after controlling for baseline status on the given outcome variable, race, whether the client was primarily seeking homelessness-related services, and total service use score—was assessed with structural modeling using Amos software (
28).
Results
The mean±SD age of the follow-up sample of 255 participants was 38.8± 8.31 years. A total of 186 participants (73 percent) were men. A large proportion were African Americans (179 participants, or 69 percent). A total of 224 (88 percent) had confirmed DSM-III-R diagnoses.
At baseline, 117 participants (46 percent) lived on the streets, in a car, in a shelter, or in transitional housing. The remaining 138 (54 percent) were often precariously housed; 19 percent of them had had to vacate their residence within two months of the baseline interview and almost half within two weeks. In addition, 199 respondents (78 percent) had been homeless at least once in the previous five years, many for a considerable period; the median duration of homelessness was two years, and 20 participants (10 percent) had been homeless for the entire five years. Thirty-seven participants (15 percent) were primarily seeking homelessness-related services at the self-help agency.
During the three months before the initial interview, participants visited the self-help agency an average of 4.14 times per week. During the six-month follow-up period, they visited the agency an average of 3.24 times per week.
On average, the study participants showed significant improvement in personal empowerment over the six-month study period, from a baseline mean score on the PES of 64 to a mean score of 68 at follow-up (t=5.39, df=254, p<.001). The mean score on the ISFS did not change significantly during the study period. The mean score on the ASFS decreased significantly, from 108 at baseline to 99 at six months (t=4.33, df=252, p<.001).
The overall structural model as estimated by Amos was significant (
Table 2). The model indicated that organizationally mediated empowerment was positively associated with all three outcomes. The standardized regression weights for the three outcome variables are listed in
Table 2. Other than baseline status, the variable that was most strongly associated with each of the outcomes was organizationally mediated empowerment.
Psychological disability was not associated with any of the three outcomes, nor was attendance at and satisfaction with the self-help agencies. Finally, among the control variables, being an African American was positively associated with all three outcomes, and seeking primarily homelessness-related services was positively associated with enhanced assisted social functioning.
Discussion
Given that enhancing personal empowerment is the primary objective of self-help agencies, the positive change in this outcome among the members of the self-help agencies in this study is gratifying. Although the presence of a control group would have allowed us to more readily attribute this finding to attendance at the agency, the association we observed is theoretically consistent with self-help agencies' claim that they empower people through agency participation.
It is a concern that we found no change in independent social functioning and that assisted social functioning decreased significantly over the study period. The decline in assisted social functioning is disturbing given that self-help agencies are thought to offer clients the type of support that enhances this mode of functioning. Some might argue that the emphasis of self-help agencies on self-reliance means that people become better able to conduct activities without the help of others and thus that clients' assisted social functioning would be expected to decrease during the course of the study. Although the improvement in the participants' personal empowerment supports this argument, the argument's validity may be questioned because we did not find a significant and compensating increase in independent social functioning. Perhaps the fact that the study participants were long-term users of self-help agencies means that they were enrolled in the study when they were at the top of their assisted functioning curve and that regression to the mean occurred.
The results of the multivariate analysis, although derived from a quasi-experimental design that limits inferences about causation, seem to demonstrate that an outcome-driven self-help agency should establish a structure that promotes the active involvement of clients in the agency's operation. It is through organizational empowerment efforts that self-help agencies seem able to achieve positive outcomes for their members. These outcomes are obtainable even for clients who have significant psychological disability, which is consistent with the ideology of self-help agencies. In fact, although we could not accept the null hypothesis, the usually apparent negative effects of such disability on outcomes appear to have been mitigated.
We did not find a positive association between outcomes and attendance at and satisfaction with the self-help agencies. Thus the provision of a user-friendly environment of peer-controlled and -operated services that ameliorate clients' dissatisfaction with mental health services may be desirable but not sufficient for achieving positive results.
Professionally led services have attempted to provide a supportive environment for many years. Proponents of self-help agencies may argue that such services are not supportive enough, but it seems that the crucial element lacking is the opportunity for empowered decision making. Mainstream community mental health agencies can take an important lesson from these results. Their efforts to involve people in meaningful decision making about their own care and the care of others may be just as influential in the context of their own experience as they appear to be in the client-run self-help agency.
It must again be emphasized that our results apply to the model self-help agencies studied and that there is increasing variance in the philosophy and operations of self-help agencies nationwide. Our results may not be generalizable beyond long-term clients who have made the effort to visit the agency at least once a week on average for at least three months. Furthermore, we had no control group to enable further validation of the importance of organizational empowerment to outcomes of clients in self-help agencies. Nevertheless, these empirical findings seem to offer initial confirmation of and insight into the active ingredient of intervention efforts of self-help agencies. Future research should attempt to replicate our model in a randomized clinical trial.
Conclusions
Our results support the hypothesis that the significant ingredient for promoting positive outcomes among clients in self-help agencies is an organizational structure that allows clients to meaningfully participate in decisions about their care and the care of others. Peer-controlled and peer-operated service that is attitudinally supportive may be desirable but not necessarily sufficient for achieving such positive outcomes.
Acknowledgment
This study was supported by grant R01-MH-37310 from the National Institute of Mental Health.