Between 2 and 8 percent of all older patients who are discharged from the hospital have diagnosed substance use disorders (
1,
2). Almost nothing is known about the specialized substance abuse and psychiatric treatment these patients obtain. Previously, we examined data from a cohort of more than 21,000 patients aged 55 years or older who had a substance use disorder and who were receiving care from the Department of Veterans Affairs (VA) health care system. After hospital discharge, these patients had a high mortality rate (
3). Over the short term, surviving patients used considerable amounts of specialized substance abuse and psychiatric services (
4), which we refer to in this article as mental health services.
The purpose of this study was to examine the long-term pattern of mental health service use by surviving members of this cohort and to identify baseline patient and treatment characteristics associated with their long-term use of mental health services.
Our previous research showed that over a short-term follow-up period, older surviving VA patients with a substance use disorder used considerable amounts of mental health services (
4). However, on an annual basis, the proportion of patients who obtained outpatient and inpatient mental health care declined. A relatively high rate of short-term remission from alcohol and drug use disorders among older persons may, in part, have accounted for this pattern (
5). Furthermore, because they tended to be in better health, surviving patients may have required less outpatient treatment and rehospitalization than those who died during the follow-up period. However, longer-term relapse rates among older patients with substance use disorders (
6), as well as increased morbidity associated with aging, may mitigate this downward trend (
7).
The older surviving patients with substance use disorders obtained less specialized outpatient mental health treatment—and more outpatient medical care—than their younger counterparts (
1). This may have occurred because physicians prefer medical management over specialized mental health treatment of older patients' substance use disorders (
1). This preference may become more pronounced over time as these patients increasingly experience age-related comorbid medical disorders. Longitudinal data on the use of outpatient health services provide an opportunity to examine whether the proportion of older patients with substance use disorders who use outpatient medical services does in fact increase while the proportion who use outpatient mental health services declines.
During four years after hospital discharge, 57 to 77 percent of older surviving VA patients with substance use disorders received outpatient mental health care (
4). Patients who were initially diagnosed as having alcohol psychosis were the least likely to obtain such care, whereas patients with both a substance use and a psychiatric disorder were the most likely to obtain it. Rates of hospital readmission during the four years also varied by diagnostic subgroup: 57 percent among patients with only a substance use disorder and 71 percent among those with a dual diagnosis (
4). In this study we considered whether patients' initial mental health diagnoses would also have long-term implications for their use of mental health services.
Younger age and being unmarried were associated with a higher rate of four-year mental health readmissions among older patients with substance use disorders (
4). A longer history of substance abuse and co-occurrence of an alcohol use and a psychiatric disorder also predicted greater short-term use of mental health services. Some specific psychiatric conditions predict poorer short-term outcomes for patients with a substance use disorder (
8,
9) and may predict greater use of mental health services by older patients who have substance use disorders. In the study reported here we considered whether demographic characteristics, severity of illness, and individual psychiatric disorders that were known at the time of discharge were associated with a greater likelihood of using mental health services over a ten-year follow-up period.
Better continuity of care may help prevent rehospitalization of older patients with substance use disorders. VA residential care units focus on enhancing social and problem-solving skills and ties to community resources (
10,
11). Thus older patients who are treated in these units may have less of a need for supportive mental health services after discharge. Longer initial hospital stays are also associated with a lower risk of subsequent mental health readmissions (
4), perhaps because they allow more time for thorough evaluation, treatment, and discharge planning.
This study addressed several questions. First, over a ten-year period, would older surviving patients with substance use disorders increase their use of outpatient and inpatient mental health services? Second, during this period, would patients rely more on medical services and less on mental health services? Third, would older patients who were initially diagnosed as having both a substance use disorder and a psychiatric disorder use more services than patients who were diagnosed as having only a substance use disorder? Finally, would variables known at hospital discharge (part of the patient's record), such as demographic characteristics, severity of illness, and continuity of care, predict whether surviving patients would use mental health services over the next ten years?
Methods
Patients
During fiscal year 1987 (October 1, 1986, through September 30, 1987), a total of 21,139 patients aged 55 years or older were discharged alive from VA hospitals with substance use disorders. In this article we refer to this hospitalization as the index episode of care. Diagnostic and treatment data on these patients were obtained from VA inpatient and outpatient files—the Patient Treatment File and the Outpatient Clinic File (
1).
According to the VA Beneficiary Identification and Records Locator Subsystem, 10,461 of these patients (49 percent) died during the next ten years. We previously reported on the patterns and predictors of mortality in this cohort; being older, being unmarried, and having more severe illness at baseline predicted earlier death (
3).
The 10,678 surviving patients were classified into three groups based on
ICD-9-CM (
12) diagnosis in the index episode: 6,012 patients with a diagnosis of alcohol or drug abuse or dependence only (codes 303, 304, and 305), of whom more than 95 percent had a diagnosis of alcohol abuse or dependence; 1,554 patients with a diagnosis of alcohol or drug psychosis (codes 291 and 292), of whom more than 97 percent had an alcohol psychosis; and 3,112 patients with a psychiatric diagnosis (codes 290, 293 to 302, and 306 to 319) in addition to a substance use disorder diagnosis.
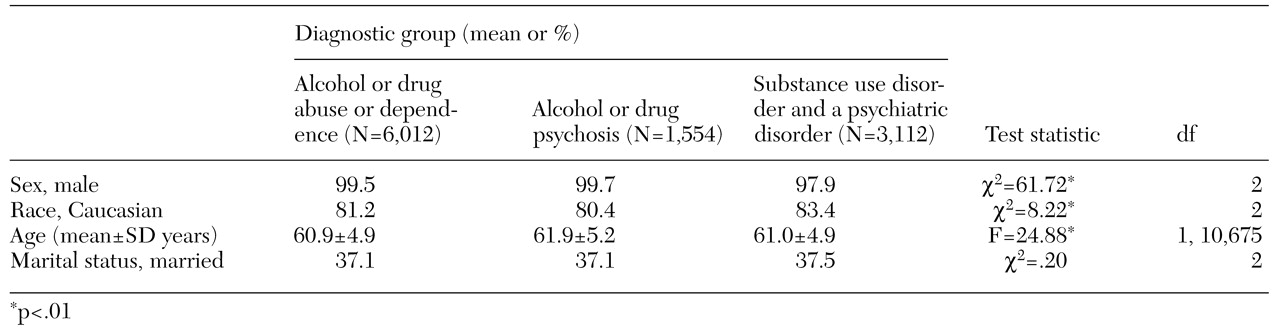
The demographic characteristics of the patients in these three groups are summarized in
Table 1. Almost all the patients were men, and 82 percent were Caucasian. At baseline, the patients had a mean age of 61 years; about 37 percent were married.
Measures
Characteristics at discharge from the index episode. Characteristics at discharge from the index episode included whether the patient had been hospitalized with a substance use disorder (ICD-9-CM codes 291, 292, 303, 304, 305) in the four years preceding the index episode and whether the patient had any psychiatric diagnosis (codes 290, 293 to 302, and 306 to 319) during the index episode. We also examined data from the index episode for the presence of ICD-9-CM codes indicative of specific psychiatric disorders, including depression (codes 296.2, 296.3, 296.82, 298.0, 300.4, 301.12, 311, 309.0, and 309.1), manic or bipolar affective disorder (code 296), schizophrenia (code 295), and personality disorder (code 301); for whether the patient had obtained care in a residential treatment unit; and for whether the index episode of care lasted 15 days or longer. All these variables were dichotomous and were scored as 1 ("yes") or 0 ("no").
Follow-up measures. The pattern of outpatient mental health care was based on the annual percentage of patients who obtained outpatient mental health services in each of four intervals—the first year, years 2 to 4, years 5 to 7, and years 8 to 10—after the index episode. For patients who obtained care, we calculated the mean number of visits per year. We also determined the overall percentage of patients who received outpatient mental health care during the ten-year follow-up period and the average annual number of visits by each patient for the entire ten years. The same method was used to determine the pattern of outpatient medical care.
The pattern of mental health readmissions was based on the annual percentage of patients who were readmitted to the hospital with at least one mental health diagnosis (ICD-9-CM codes 290 to 319) in each of the four time intervals as well as the overall percentage of patients who had at least one mental health readmission during the entire ten-year period. For patients who were readmitted with a psychiatric diagnosis, we calculated the number of readmissions over the ten-year period (one readmission, two to four readmissions, five to seven readmissions, eight to ten readmissions, and 11 or more readmissions).
Analyses
Annualized mental health outpatient treatment and readmission rates are presented in Tables 2 and 3, respectively. These rates were obtained by summing annual percentages within each interval—for example years 2 to 4—and dividing by 3. To determine the statistical significance of group differences in annualized rates, we determined whether a patient had obtained care in a particular three-year interval and then conducted a 3 × 2 (group membership by obtained care) chi square analysis.
Only patients who had made at least one visit to a mental health clinic in a given year were included in the calculation of annualized rates of outpatient mental health visits. These rates were determined by summing patients' visits across the time interval of interest and dividing by 3. Statistical significance of group differences was determined by conducting one-way analyses of variance on patients' average number of visits within each three-year interval. To determine whether there were significant group differences in the distribution of readmissions over the ten-year follow-up (
Table 3), we conducted a 3 × 5 (group membership by readmissions level) chi square analysis.
Predictors of use of mental health services during the ten-year period were identified in a three-step process. First, we examined associations between each individual characteristic that had been assessed during the index episode and the two service use outcomes—outpatient mental health care (yes or no) and mental health readmissions (yes or no) within ten years after discharge. Next, we entered variables that had consistently significant (p<.05) associations with the outcomes into logistic regression models. Significant predictors were retained and are shown in the final logistic regression models.
Results
Service use
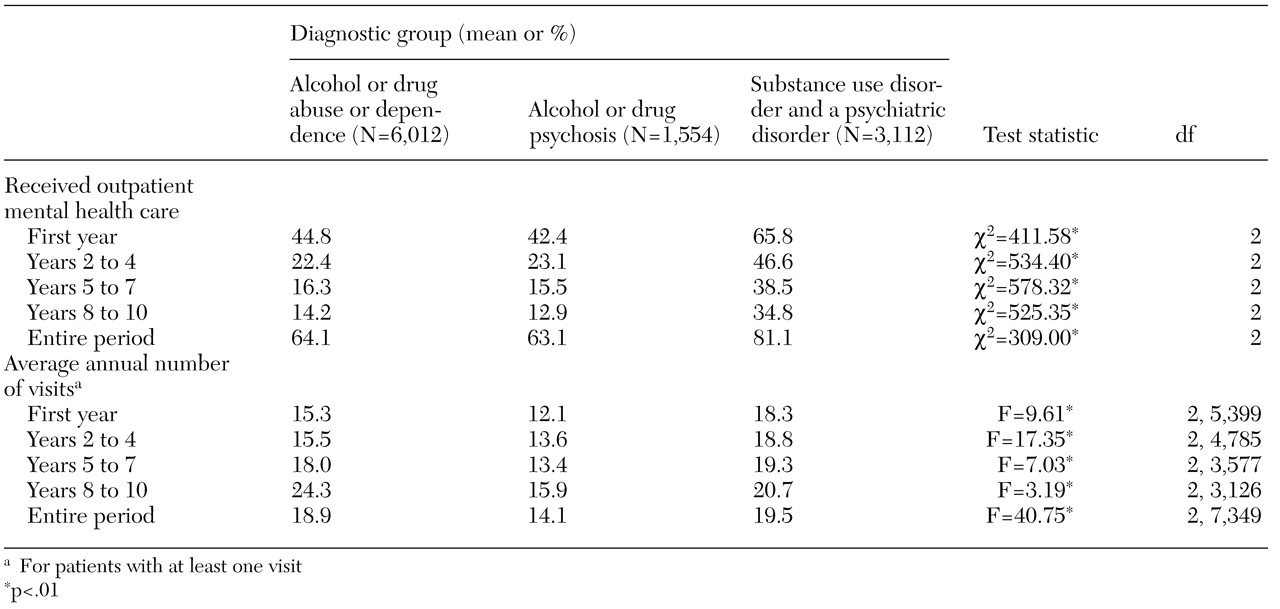
The overall pattern for the ten-year period was a decline in the proportion of patients who used mental health services. However, among patients who obtained outpatient services, the intensity of use increased, as can be seen in
Table 2. A similar pattern was observed for outpatient medical care (data not shown).
Differential patterns of use by diagnosis
Outpatient treatment. Compared with patients with only a substance use diagnosis, those with dual diagnoses were significantly more likely to obtain outpatient mental health care, as shown in
Table 2. In the first year after discharge from the index episode, 66 percent of patients with a substance use disorder and another psychiatric disorder received outpatient mental health treatment, compared with 45 percent of those with only an alcohol or drug use disorder. Over the entire ten-year period, 81 percent of patients with a dual diagnosis received outpatient mental health treatment, compared with only 64 percent of those with only an alcohol or a drug use disorder.
Among patients who obtained outpatient mental health care, the yearly average number of visits increased during the follow-up period. The sharpest increase and highest average number of clinic visits occurred in years 8 to 10 and among patients who were initially diagnosed as having only an alcohol or drug use disorder.
The same overall pattern was seen for outpatient medical treatment. Consistently within each of the four time intervals, patients with dual diagnoses were more likely to obtain outpatient medical care than were patients with only alcohol abuse or dependence or alcohol psychosis. The annual number of visits increased among patients who did obtain care.
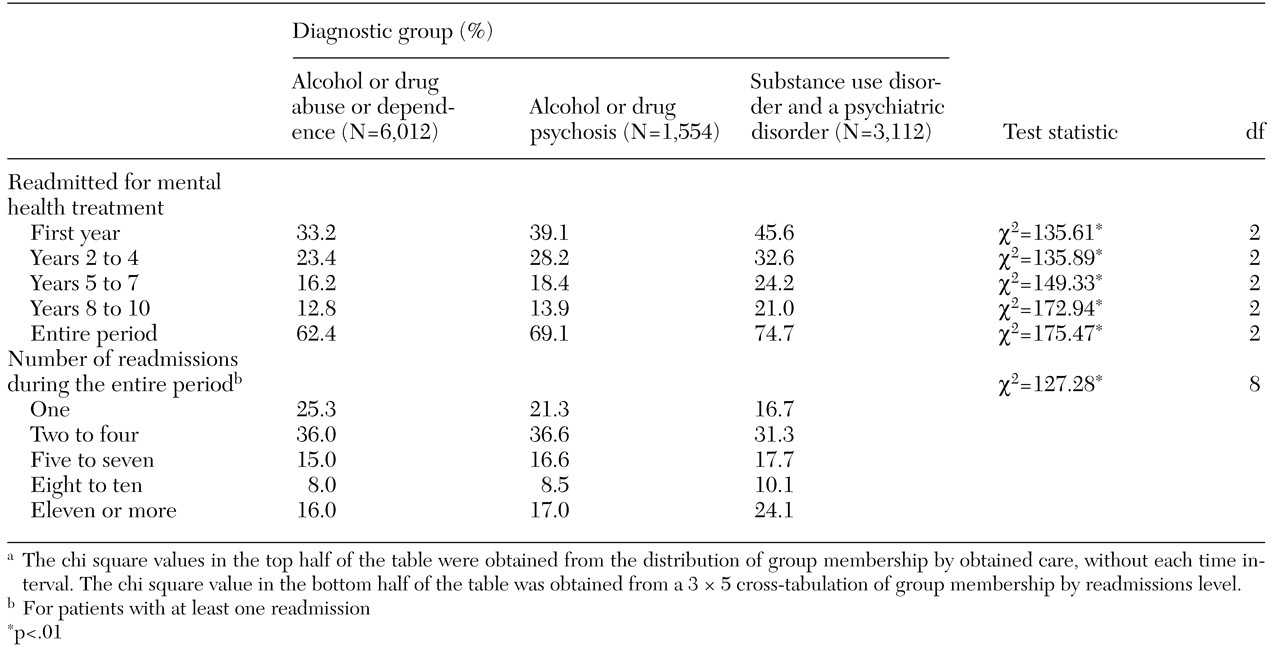
Readmissions. In each of the four postdischarge intervals, patients who had dual diagnoses at baseline were more likely to return for inpatient mental health care than were patients who had only an alcohol or drug use disorder, as illustrated in
Table 3. The overall ten-year mental health readmission rates were substantial: 62 percent among patients with only alcohol or drug abuse or dependence, 69 percent among patients with alcohol or drug psychosis, and 75 percent among patients who had a substance use disorder and another psychiatric disorder. Multiple readmissions were common, especially among patients with dual diagnoses. For example, 24 percent of patients with a substance use disorder and another psychiatric disorder were hospitalized at least 11 times over the ten-year period.
Predictors of use
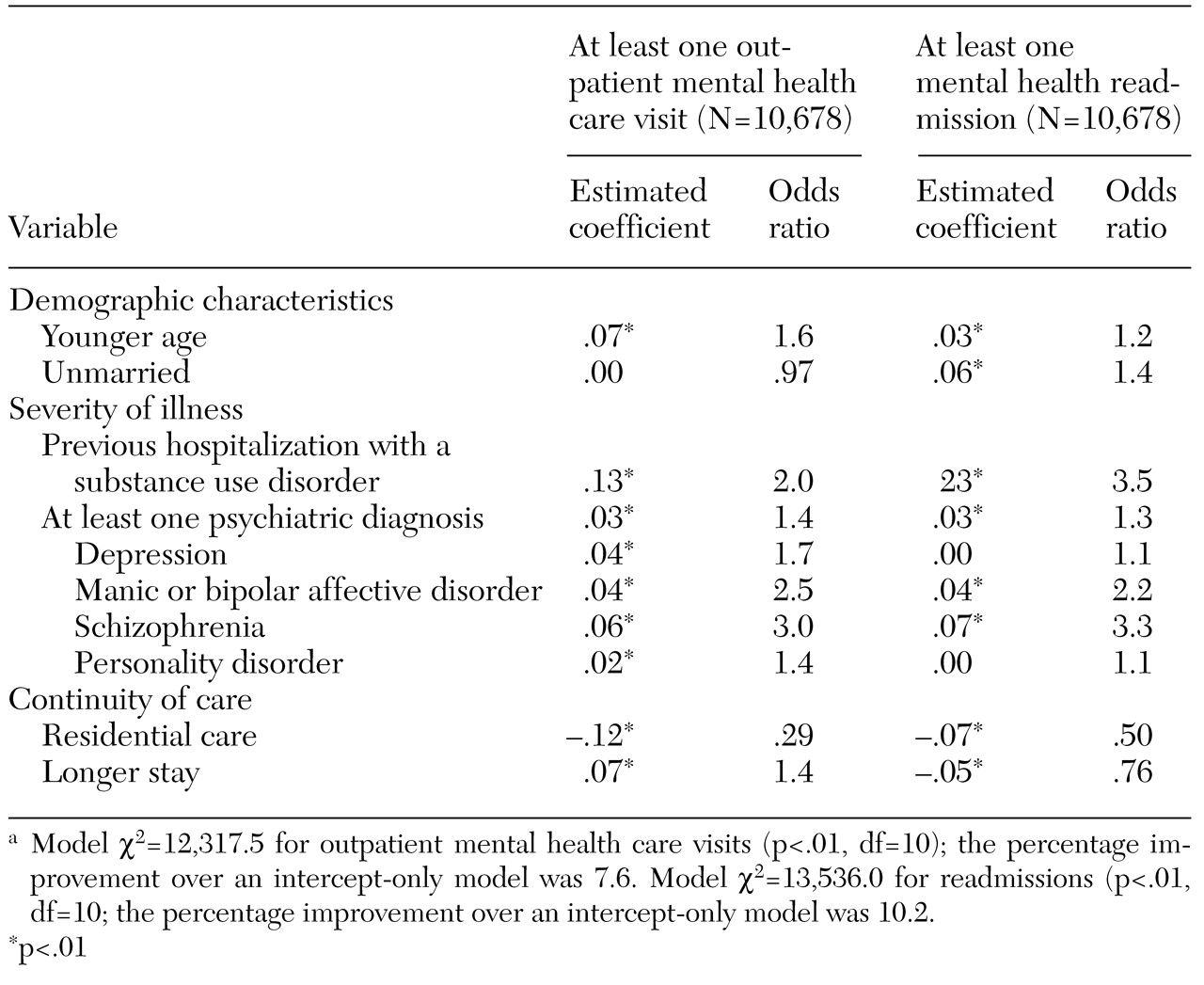
Data on index episode predictors of use of mental health services over the follow-up period are summarized in
Table 4. Being younger and having a more severe disorder were associated with greater use of mental health services over the follow-up period. Depressive, manic or bipolar affective, schizophrenic, and personality disorders were all associated with use of outpatient mental health services. Manic or bipolar affective and schizophrenic disorders were associated with readmission. Initial stay on a residential care unit and longer stay were associated with a lower likelihood of mental health readmissions.
Discussion
Of the large number of older patients who are discharged from the hospital with a diagnosed substance use disorder each year, many survive for long periods. This study focused on the ten-year pattern of use of mental health services among surviving older patients with substance abuse as well as baseline factors that affect the likelihood that these patients will subsequently obtain mental health care.
Patterns of service use
The proportion of older surviving VA patients with substance use disorders who obtained mental health care in the VA system declined significantly over the ten-year period. This decline may in part be a reflection of the considerable rate of improvement in substance abuse and dependence among older adults (
5,
6). It is also possible that the decline reflects greater eligibility for and use of Medicare-reimbursed mental health care by these patients. However, Medicare requires a 50 percent copayment for outpatient mental health care (
13), which probably discourages patients' migration from VA to Medicare-reimbursed outpatient mental health treatment. Furthermore, the rate of diagnosed substance use disorders among Medicare inpatients aged 65 years or older is only 1.9 percent (
2), which suggests that there is no mass exodus by patients from VA-provided to Medicare-reimbursed inpatient mental health treatment. Nonetheless, a complete account of long-term use of mental health services by these patients would encompass the patients' Medicare-reimbursed and privately insured treatment as well as their VA care.
The intensity of service use increased over time among the patients who obtained mental health care. The sharpest increase and the highest average number of outpatient mental health visits occurred in years 8 to 10 among patients who were initially diagnosed as having only an alcohol or drug use disorder. This finding suggests that even late in their drinking or drug-taking careers, some older patients who are initially diagnosed as having only a substance use disorder intensify their efforts to manage their alcohol or drug problems. The finding may also indicate the development or reemergence of comorbid psychiatric disorders that require more intensive mental health treatment.
We considered whether medical care increasingly substituted for mental health care over the ten-year period. This did not appear to be the case, detracting from the idea that physicians steer older patients with substance use problems away from specialized substance abuse and psychiatric services in favor of medical management of substance abuse.
Differences by diagnosis
Patients with substance use disorders had distinct patterns of use of mental health services, depending on their diagnosis. About 14 percent of the patients in our sample were initially diagnosed as having an alcohol psychosis. These patients were more likely to require inpatient mental health care than were patients who were diagnosed as having only substance abuse or dependence, reflecting the ongoing need of these patients for more intensive inpatient support, such as acute detoxification services.
A significant proportion of the patients (29 percent) had a dual diagnosis when they were discharged from the index episode of care. Over the ten-year follow-up period, these patients were consistently more likely to obtain mental health services than were patients who had only a substance use disorder. Clinicians have noted that older patients who have a substance use disorder and a concomitant psychiatric disorder present a treatment challenge (
14,
15). Our findings confirm that as such patients grow older, they have a long-term, sustained need for more intensive inpatient and outpatient mental health care.
Index-episode predictors of subsequent care
Several variables known at discharge predicted which patients would return for additional mental health treatment, including younger age and a greater severity of illness. Being unmarried and having a diagnosis of a manic or bipolar affective or schizophrenic disorder were associated with rehospitalization over the long term. Patients with these characteristics can be identified at discharge, and special preventive efforts can be made to avoid rehospitalization.
Treatment in a VA residential care unit was associated with a lower likelihood of mental health service use. Residential care emphasizes the development of social skills and problem solving and provides help in obtaining community services (
10,
11). Older patients who initially obtain care on these units may be better able to function without subsequent formal health services, even over long periods. A longer stay was associated with a lower risk of readmission over the next ten years. More thorough evaluation, treatment, and discharge planning may also prevent rehospitalization of older patients with substance use disorders.
Limitations
The long-term patterns and predictors of use of mental health services described here may not be generalizable to older surviving female patients with substance use disorders, other cohorts of older patients with such disorders, or other health care systems. It is important to note that our findings apply only to patients who survived the entire ten-year follow-up period. Patients who were older or sicker and who had fewer social resources at baseline were less likely to survive (
3). Thus long-term use of mental health services in the entire cohort was probably higher than suggested by our results. More research is needed to determine whether our findings are generalizable to other older patients with substance use disorders.
The data we analyzed were a good source of descriptive information about long-term use of mental health services, but additional data are needed about specific services received and to explain why the proportion of older surviving patients with substance use disorders who use VA mental health services declines over time. Future research should examine whether this pattern stems from patients' using other sources of health care, remission of substance use problems, improved overall health, or age-related barriers to care, such as transportation problems (
16).
Conclusions
A substantial number of older patients with substance use disorders survive and continue to require mental health care services over the long term. A portion of these patients require increasingly intensive services. The long-term demand for mental health services is strongest among patients with a longer history of substance misuse who have both a substance use diagnosis and another psychiatric diagnosis. Overall, our findings underscore the need for careful evaluation, discharge planning, and long-term monitoring of older patients who are hospitalized with alcohol and drug use disorders. Targeted interventions, such as enhanced continuity of care, might reduce avoidable or excessive use of mental health services by this patient population.
Acknowledgments
This study was supported by grants AA-06699 and AA-12718 from the National Institute on Alcohol Abuse and Alcoholism and by the Department of Veterans Affairs Mental Health Strategic Health Group and the Health Services Research and Development Service of the Office of Research and Development. The authors thank Bernice S. Moos, B.S., and Deborah Hirst, M.A., for assistance with data analysis.