There is a growing trend in the Department of Veterans Affairs (VA) system for veterans to seek such payments. Recent data show that Gulf War veterans draw disability compensation at a much higher rate than veterans of any previous conflict and at almost twice the current rate of World War II veterans (16 percent compared with 8.6 percent) (
5). Furthermore, 69 to 94 percent of veterans who seek treatment for PTSD in the VA system apply for psychiatric disability (
6,
7,
8). Evidence suggests that evaluation of PTSD symptoms in this population may be influenced by the substantial financial incentive for veterans to present as socially and occupationally impaired. Given that lifetime prevalence of PTSD among combat veterans is between 9 percent and 31 percent (
9,
10), this issue is highly relevant to the VA system in terms of both clinical care and disability policy.
Background
In 1996, total compensation and pension expenditures for the VA were estimated to be just over $18 billion, with 2.2 million of the surviving 25.4 million veterans (8.9 percent) receiving some level of service-connected disability benefits (
11). If disability status is granted, a rating of severity of disability is made on a scale of zero to 100 percent. The relationship between disability payments and disability ratings is curvilinear, and many benefits—for example, some medical and dental coverage—do not begin until the veteran receives a rating of 100 percent. Even veterans who are rated as 90 percent disabled stand to benefit significantly when their rating increases to 100 percent.
When disability claims are denied or are only partially granted, veterans may appeal the decision an indefinite number of times. These repeat claims outnumber original claims almost three to one and dominate the VA adjudication and appeals system. Veterans who are granted disability compensation must undergo continuing disability review, usually every other year, to determine whether they continue to be eligible for disability payments.
For many veterans who have chronic illnesses, the process of obtaining and maintaining disability payments is a protracted struggle. However, the financial incentives are significant. For example, in South Carolina, where per capita income is about $17,000 before taxes, a single veteran without dependents who was 100 percent service connected in 1999 received an annual tax-free income of $23,868, in addition to other benefits (
11).
Studies consistently demonstrate that combat veterans who are evaluated for PTSD in the VA system exhibit extreme and diffuse levels of psychopathology across instruments that measure different domains of mental illness and extreme elevations on the validity scales of the Minnesota Multiphasic Personality Inventory (MMPI) in the direction of overreporting (
12,
13). These validity scales—for example, the F-K index—take into account the stereotypes held by many lay people who assume that serious mental illnesses involve a large number of bizarre symptoms, such that high scores indicate endorsement of items that are rarely endorsed even by persons with the most severe mental illness. An in-depth discussion of how these validity scales were developed, what they mean, and how they should be applied to veterans has been published elsewhere (
14).
Combat veterans also are prone to inflating their reports of combat exposure over time (
15). This general reporting pattern significantly complicates the assessment of symptoms for the purposes of both diagnostic decision making and evaluation of treatment outcome and frequently casts doubt on the credibility of symptom reports (
13). We have previously discussed possible explanations for this pattern (
13), including co-occurrence of symptoms, a "cry for help," a sociological phenomenon known as Vietnam syndrome, and the influence of systemic variables within the VA.
Some researchers have speculated that the phenomenon of apparent symptom overreporting may reflect the motivation of veterans to present as severely disabled in order to obtain disability compensation (
16,
17). Several studies have examined the influence of compensation-seeking status on symptom reporting patterns by using self-report measures of psychopathology. Although two early studies had mixed results (
18,
19), their conclusions were limited by the manner in which compensation seeking was defined and in how the study participants were grouped for analysis.
Accurately understanding the role of compensation-seeking status requires a definition of "compensation seeking" that maximally differentiates persons who have financial incentives from those who do not. Two studies examined this issue by differentiating veterans on the basis of financial incentive (
7,
8). Veterans were classified into two groups at the time of evaluation. Compensation-seeking veterans were those who were currently seeking or planning to seek VA disability compensation or increases in existing disability payments for PTSD. Non-compensation-seeking veterans were those who were not intending to seek VA disability compensation for their PTSD symptoms.
The proportion of veterans who were classified as compensation seeking in each of these two studies was identical at 69 percent. Compensation-seeking veterans received significantly higher pathological scores on clinical measures and obtained much higher elevations on MMPI validity scales associated with symptom exaggeration and malingering than did non-compensation-seeking veterans. These results were obtained despite the fact that the two groups did not differ in the frequency of PTSD diagnoses. Furthermore, differences on most indexes exceeded effect sizes of 1.0, even when the effects of income, Global Assessment of Functioning (GAF) scores, and clinician-rated severity of PTSD were controlled for.
Evidence also suggests that the MMPI validity scales can be used to identify veterans who may be exaggerating their psychopathology in order to gain disability compensation. Specifically, veterans with F-K indexes of more than 13 were not significantly more likely to be seeking compensation (
20), whereas those with F-K indexes of more than 22 were, and they scored much higher on self-report measures of psychopathology despite having lower rates of PTSD diagnoses and similar rates of other psychiatric diagnoses (
21). (Possible scores on the F-K index range from −30 to 60, with higher scores indicating greater symptom exaggeration or malingering.) These data suggest that the availability of disability benefits influences the way in which veterans present their difficulties. This conclusion is consistent with evidence that persons from other compensation-seeking populations—for example, injury and pain litigants—also tend to overreport symptoms (
22).
The study reported here used archival data to further examine the relationship between compensation-seeking status and symptom reporting among combat veterans who were evaluated for PTSD. Specifically, we were interested in comparing the symptom reports of combat veterans who were seeking compensation for any type of disability with the reports of those who were not seeking such compensation. We hypothesized that differences consistent with the results of previous research would be demonstrated between these two groups.
Methods
Participants
Archival data were drawn for 320 male combat veterans aged 18 years or older who were consecutively evaluated at a VA PTSD outpatient clinic from 1995 to 1999. The study was conducted after approval had been obtained from an institutional review board, including a waiver of the requirement for obtaining informed consent. Compensation-seeking status was obtained through interviews, chart reviews, and self-report items included in a psychosocial history questionnaire. Study participants were classified as compensation seekers if they had already applied or were planning to apply for any type of VA disability compensation. Participants were classified as non-compensation seekers if they were not intending to apply for any type of VA disability compensation.
Data on compensation-seeking status were available for 193 veterans (60 percent), including 143 compensation seekers (74 percent) and 50 non-compensation seekers (26 percent). Our experience with the PTSD clinic suggests that the lack of data for 40 percent of the total sample was due to changes and fluctuations in procedures for conducting evaluations over time rather than the result of any systematic source of bias or error. However, we conducted statistical analyses to compare veterans for whom compensation-seeking status was available with veterans for whom it was not. The rate of disability seeking was 5 percent higher than in previous studies, which have focused specifically on compensation seeking for PTSD (
7,
8).
Procedure and instruments
Psychiatric diagnoses were based on
DSM-IV (
23). All PTSD diagnoses were determined on the basis of team consensus (a psychiatrist, a clinical psychologist, and a social worker) after a thorough evaluation, including a chart review, psychosocial and military history interviews, and the Clinician-Administered PTSD Scale (CAPS-1), a structured clinical PTSD interview (
24).
Additional clinical information was obtained by using a battery of self-report measures, including the Minnesota Multiphasic Personality Inventory-2 (MMPI-2), a widely used 567-item true-false questionnaire that assesses a wide range of domains related to psychopathology and test-taking attitude, including scales designed to detect feigned or exaggerated psychopathology (
25); the Beck Depression Inventory (BDI), a widely used, well-validated, 21-item self-report measure of depressive symptoms (
26); the Dissociative Experiences Scale (DES), a 28-item self-report measure of dissociative symptoms (
27), with a behaviorally anchored, fixed response format (DES-FRF) found to have good alternate form reliability (r=.71) with the original DES, strong internal consistency (alpha=.95), and a significantly lower inverse relationship with intelligence (r=−.18) compared with the original DES (r=−.42) (
28); and the Mississippi Combat PTSD Scale (M-PTSD), a 35-item Likert-scale measure of combat-related PTSD symptoms that has been widely used and has strong psychometric properties (
29).
Statistical analyses
Because compensation-seeking status was available for only 60 percent of the veterans in our archival data set, we first conducted multivariate analyses of variance and chi square tests to compare clinical and demographic characteristics of veterans for whom compensation-seeking status was available and those for whom it was not. These analyses were conducted to ensure that there were no obvious sources of systematic bias in the way in which this variable was assessed or reported.
Analyses were then conducted to determine whether there were any demographic differences between the two groups. For continuous-scaled variables, t tests for independent samples were used; robust t tests were used when group variances were not equal—that is, when Levene's test of equal variances was significant at p<.05. Test-taking attitude was used to screen out data from veterans who completed the MMPI-2 in a grossly invalid manner, such as engaging in mostly true or mostly false responding (true response inconsistency [TRIN]>100), random responding (variable response inconsistency [VRIN]>80), or missing responses (more than 15 items left blank). These criteria resulted in the exclusion of 17 compensation-seeking and five non-compensation-seeking veterans. Thus 171 veterans (126 compensation seekers and 45 non-compensation seekers) were included in the study.
Three separate one-way multivariate analyses of covariance (MANCOVAs) were conducted to compare the two groups on MMPI-2 scales, of which all adjusted for the covariate of income, which was the single demographic variable found to be different between the two groups. The groups were first compared on the ten MMPI-2 K-corrected clinical scale raw scores, then on the 15 MMPI-2 content scale raw scores, and finally on three MMPI-2 raw-scored validity (overreporting, or "fake-bad") scales designed to detect feigned psychopathology (the F, the Fp, and the F-K index).
Individual MANCOVA alpha levels of .05 were implemented for testing effects, using Wilks' lambda statistic. Significant multivariate effects were followed by univariate tests to assess which particular scales differentiated groups (alpha=.01, to control for multiple comparisons). As an additional method of exploring the relationship between compensation-seeking status and validity scale scores, a 2 × 2 chi square analysis was conducted to test the hypothesis that extreme exaggeration (an Fp score greater than 7) would be more likely than nonexaggeration (an Fp score less than 2) for the purposes of seeking VA disability compensation (
25,
30).
Next, three separate analyses of covariance (ANCOVAs) were conducted to compare compensation-seeking veterans and non-compensation-seeking veterans on other self-report measures, adjusting for income. Separate ANCOVAs used scores on the BDI, the M-PTSD, and the DES-FRF as dependent variables. An alpha level of .01 was set for these analyses to control for multiple comparisons.
Last, a sequential logistic regression analysis was implemented to examine whether there was a relationship between compensation-seeking status and the presence of a PTSD diagnosis, with income controlled for. First, income was tested for its possible effect on disability status. PTSD diagnosis was subsequently entered to determine whether it had an effect on disability status beyond that accounted for by income. In a separate logistic regression analysis, PTSD diagnosis was entered first, followed by income to assess whether income had a significant effect on disability status beyond that achieved by PTSD diagnosis.
Results
The statistical analyses that compared veterans for whom compensation-seeking status was available with veterans for whom it was not showed no significant between-group differences on any clinical self-report measures, diagnostic rates, or demographic variables. This finding was consistent with our expectation that there would be no obvious sources of systematic bias in the way in which the variable compensation-seeking status was assessed or reported in our archival data set.
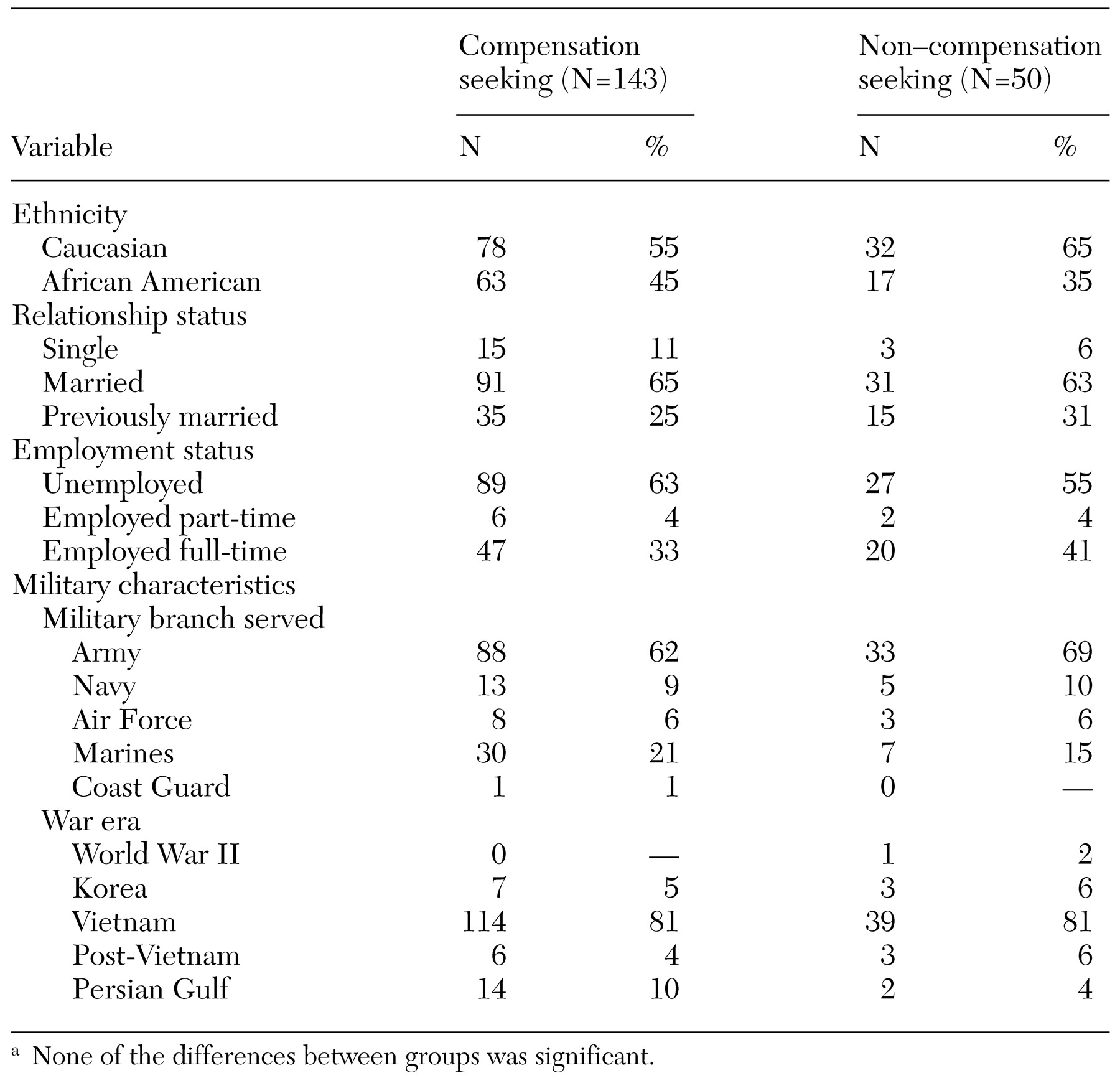
The mean±SD age of the compensation-seeking veterans was 49.01± 5.80 years, and the mean age of the non-compensation-seeking veterans was 50.22±8.18 years; no significant difference was observed between the two groups. Veterans in the compensation-seeking group had an average of 12.39±2.25 years of education, compared with 12.27±2.53 in the non-compensation-seeking group, and there was no significant difference between the two groups. The average annual income of the compensation-seeking group was $17,649.83± 17,217.36, compared with $25,011.32± 17,747.11 in the non-compensation-seeking group; the difference between the two groups was significant (t=−.25, df=161, p<.05). Groups were also compared by using chi square analyses on nominal-scaled demographic variables, including ethnicity, relationship and employment status, branch of military service, and era of war served, of which none yielded significant between-group differences (
Table 1).
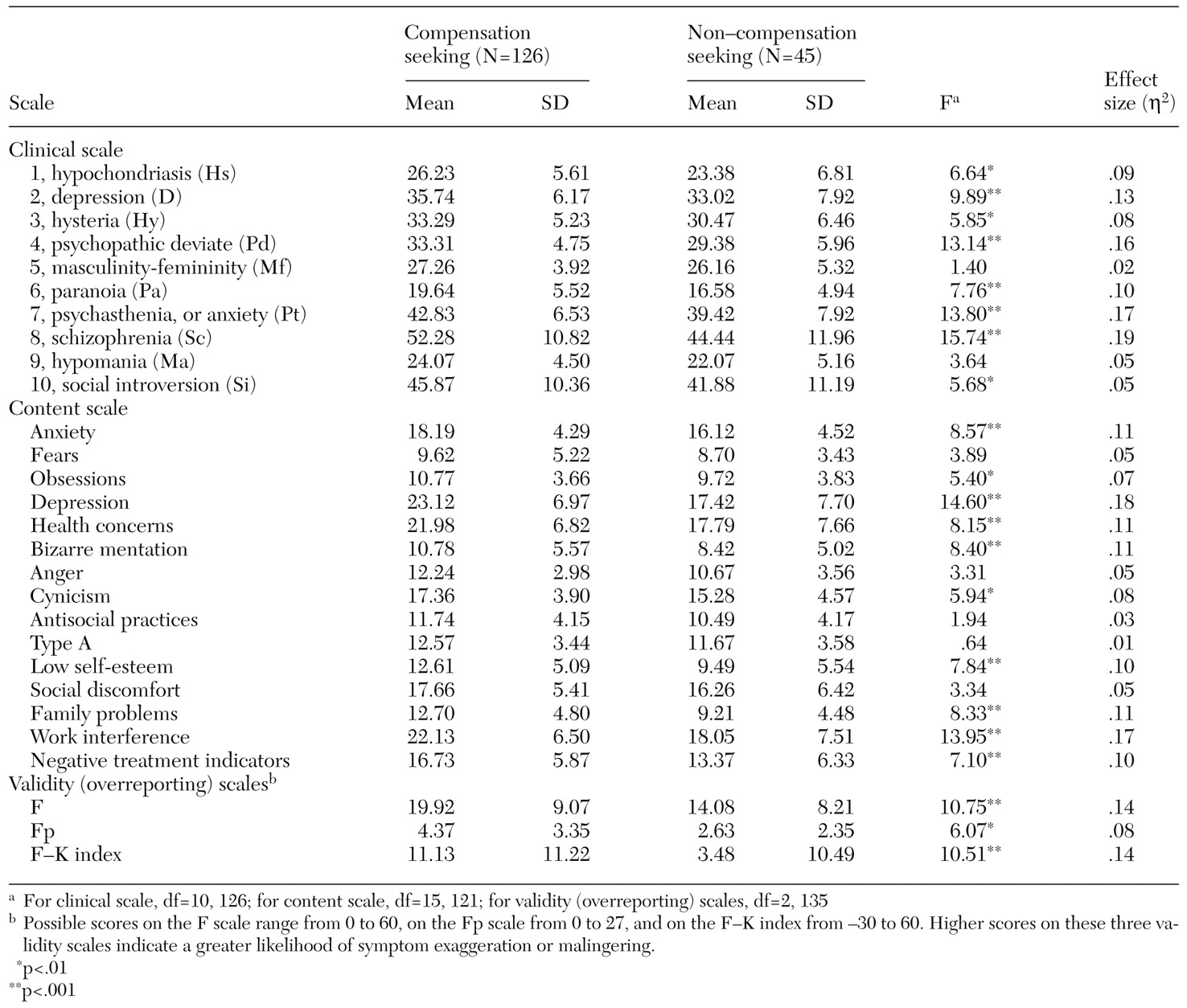
The results of the MANCOVAs that compared compensation-seeking and non-compensation-seeking veterans on the MMPI-2 clinical scales, adjusted for income, are summarized in
Table 2. Overall, the difference between the two groups was significant (F=2.09, df=10, 126, p<.05). Compensation-seeking veterans scored significantly higher on scales that measured health concerns, depression, somatization, anger and hostility, paranoid ideation, anxiety and obsessive rumination, difficulties thinking and concentrating, and social introversion.
The results of the MANCOVAs that examined the MMPI-2 content scales are also shown in
Table 2. Overall, the difference between the two groups was significant (F=2.67, df=15, 121, p<.05). Compensation-seeking veterans scored significantly higher on scales that measured anxiety, obsessive rumination, depression, health concerns, bizarre thought processes, cynicism, low self-esteem, family discord, work interference, and negative treatment indicators.
A significant difference between the groups was also noted in the MANCOVAs that examined differences on the MMPI-2 validity (overreporting) scales (overall F=3.54, df=3, 133, p<.05). The compensation-seeking group obtained higher scores on all three scales (
Table 2). The 2 × 2 chi square analysis exploring the relationship between compensation-seeking status and Fp classification of extreme exaggeration versus nonexaggeration was significant (χ
2=5.25, df=1, N=162, p<.05), with significantly more compensation-seeking veterans classified as extreme exaggerators.
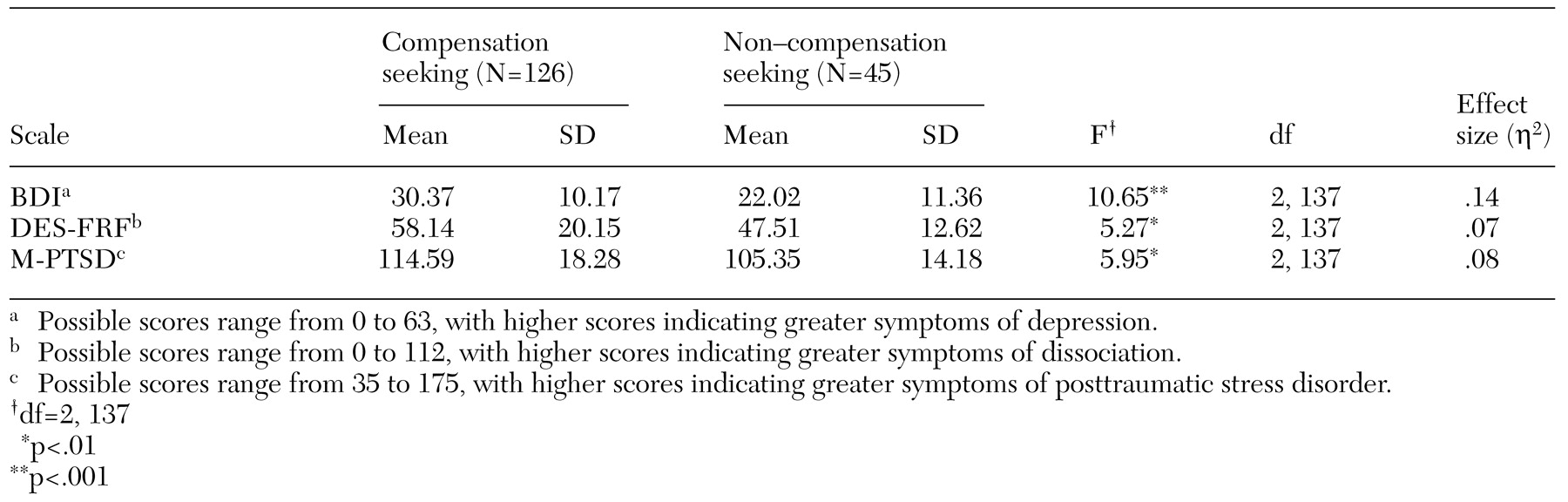
The ANCOVA results shown in
Table 3 demonstrate that, with adjustment for income, compensation-seeking veterans obtained significantly higher scores on the BDI, the DES-FRF, and the M-PTSD.
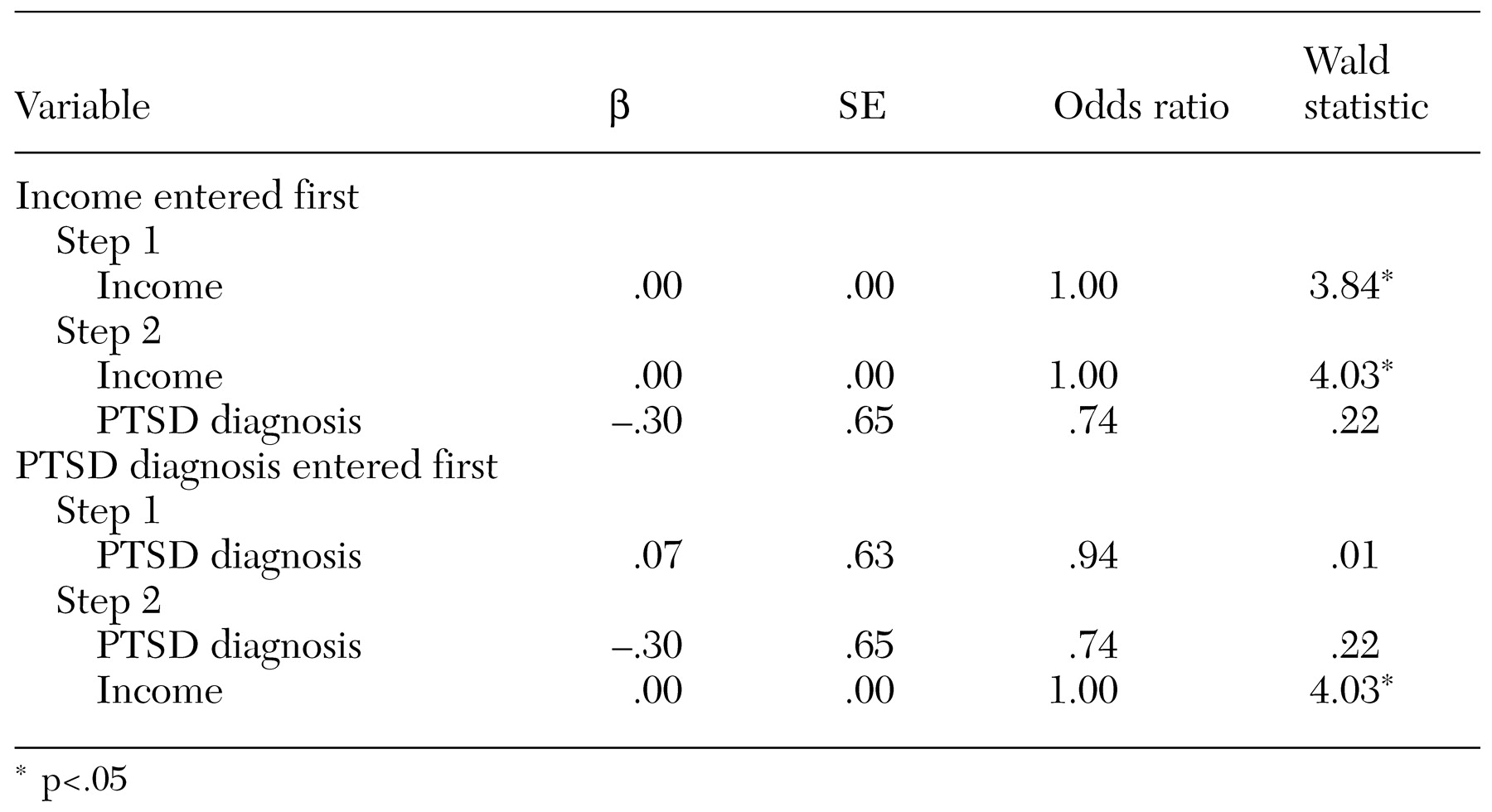
The results of the logistic regression analysis are shown in
Table 4. With income controlled for, no significant relationship was apparent between compensation-seeking status and the presence of a PTSD diagnosis. When income was entered into the regression model first, PTSD diagnosis did not predict compensation-seeking status beyond that predicted by income alone. When PTSD diagnosis was entered first, income was a significant predictor of disability status beyond the contribution of PTSD diagnosis alone.
Discussion
This study examined symptom reporting patterns among two groups of combat veterans who were evaluated for PTSD: those who were seeking compensation for any type of VA disability and those who were not. Overall, veterans who were seeking compensation obtained significantly higher pathological scores on a variety of self-report measures of psychopathology, including most clinical and content scales of the MMPI-2 and other measures of depression, dissociation, and PTSD symptom severity. This was true even when the effects of income—the sole demographic variable that proved to be significantly different between the two groups—was controlled for.
However, compensation-seeking veterans also evidenced greater elevations than non-compensation-seeking veterans on primary validity scales of the MMPI-2 (
31) and were significantly more likely to be classified as extreme exaggerators. Thus it appears that veterans who were seeking compensation were much more likely to overreport or exaggerate their symptoms than those who were not seeking compensation. This pattern of differences closely resembles those found in previous studies that compared veterans who were specifically seeking compensation for PTSD-related disability with non-compensation-seeking veterans (
7,
8), although the effects we found in our study were somewhat smaller.
Implications
Clinical care. The specter of disability payments may affect clinical care in several ways. Exaggeration of symptoms complicates differential diagnosis and the development of appropriate treatment plans. Furthermore, the effectiveness of treatment may be undermined in that the contingencies of the system reward illness behaviors and the maintenance of symptoms. Experience suggests that many patients acknowledge using treatment sessions as a means of documenting, through clinicians' progress reports, their psychiatric difficulties. The provision of permanent disability payments may also foster the harmful notion that recovery from PTSD or successful management of symptoms is not possible.
Clinicians in VA practice settings should expect that many veterans will present with unrealistic pictures of their symptoms, but such behavior should not necessarily be taken as evidence of malingering. If the MMPI-2 is used, traditional cutoff points on the validity scales (F-K scores greater than 13) may not be appropriate. Instead, population-specific cutoff points (F-K scores greater than 22) should be considered (
20). On the other hand, careful follow-up evaluation of veterans who overreport their symptoms is warranted, including careful assessment of military documentation, structured interviews, and perhaps even psychophysiological assessment.
Treatment outcome research. The evaluation of treatment outcome results in clinical trials is a related area of concern. Treatment efficacy data for combat-related PTSD are currently lacking. Furthermore, in many studies PTSD treatment effect sizes were larger in nonveteran samples than among veterans (
32). This observation may be at least partially attributed to the overreporting response pattern and the reluctance of many veterans to acknowledge therapeutic gains because they have financial incentives not to do so.
Although there have been few direct empirical studies of this hypothesized association between compensation seeking and treatment, several studies have had results that deserve mention. One study found that veterans who were classified on the MMPI as "symptom overreporters" were less likely to manifest improvement after six weeks of partial hospitalization, even though clinicians did not consider them to be more dysfunctional than other veterans before treatment (
33). In addition, several treatment outcome studies showed disparities between veterans' extreme self-reported symptom patterns and other data collected through clinicians' ratings, psychophysiological measures, and daily symptom frequency counts (
34,
35,
36). Finally, data from a study of veterans who were treated for PTSD within the VA system indicated that compensation-seeking status had a significant treatment effect among inpatient veterans, although no such effect was found among outpatient veterans (
6).
Future research directions. Veterans who have PTSD often experience severe psychiatric, medical, social, and occupational impairment that results in persisting financial hardships. They therefore require and deserve appropriate assistance in these areas. However, our understanding of the influence of veterans' disability compensation seeking on their use of medical, rehabilitative, and cash assistance programs remains undeveloped. Further research is needed to better understand how compensation-seeking status influences the evaluation of treatment outcome; to explore the relationship between disability, compensation seeking, and the use of general medical services in the VA health care system (
37) and the interface with other disability providers, such as Social Security Disability Insurance (
38); to test the effectiveness of state-of the-art supported employment services (
39,
40,
41), an innovative advance over standard vocational rehabilitation services offered by the VA whose effectiveness for persons with severe PTSD has been very poor (
42,
43); and to better understand the costs associated with federal disability policies and different VA disability evaluation strategies, which meet the moral imperative of reintegrating very ill, disabled, indigent, and isolated veterans into mainstream community life (
44,
45,
46).