Study participants
We contacted military and civilian staff in one of the Washington, D.C., metropolitan area military hospitals after obtaining permission from senior hospital administrators and after review and approval by the institutional review board. The hospital provides a full range of inpatient and outpatient services and is the site of multiple graduate medical education programs. Fifty percent of the staff is military, and approximately 50 percent of the staff are involved in direct patient care, with the remainder serving in support and administrative areas. None of the sniper victims was admitted to this hospital, and, to our knowledge, none was related to any member of the staff.
An electronic questionnaire was distributed to 2,400 employees who had e-mail accounts. The questionnaire informed potential study participants of the voluntary nature of the study, discussed risks and benefits, and provided a contact point should participants have questions or concerns. To preserve confidentiality, the institutional review board waived the requirement for written informed consent. The questionnaire was distributed five days after the apprehension of the sniper suspects. Responses were collected during the next two weeks. Responses were routed anonymously through an Internet server. Of 415 responses received (response rate of 17 percent), we discarded 33 because major portions of the survey were incomplete, leaving 382 valid responses.
Of the 382 respondents, 209 (55 percent) were women, 207 (54 percent) belonged to the military, 233 (62 percent) were married, and 230 (60 percent) had children. The respondents' mean±SD age was 39±10.9 years. The group was predominately Caucasian (268 respondents, or 71 percent). All participants had at least a high school education; 207 (55 percent) had a college degree. The respondents included 49 physicians (13 percent), 53 nurses (14 percent), 55 medical technicians (14 percent), and 223 administrative employees (59 percent). The demographic distribution of the final sample closely resembled that of the overall sample of staff contacted.
Assessments
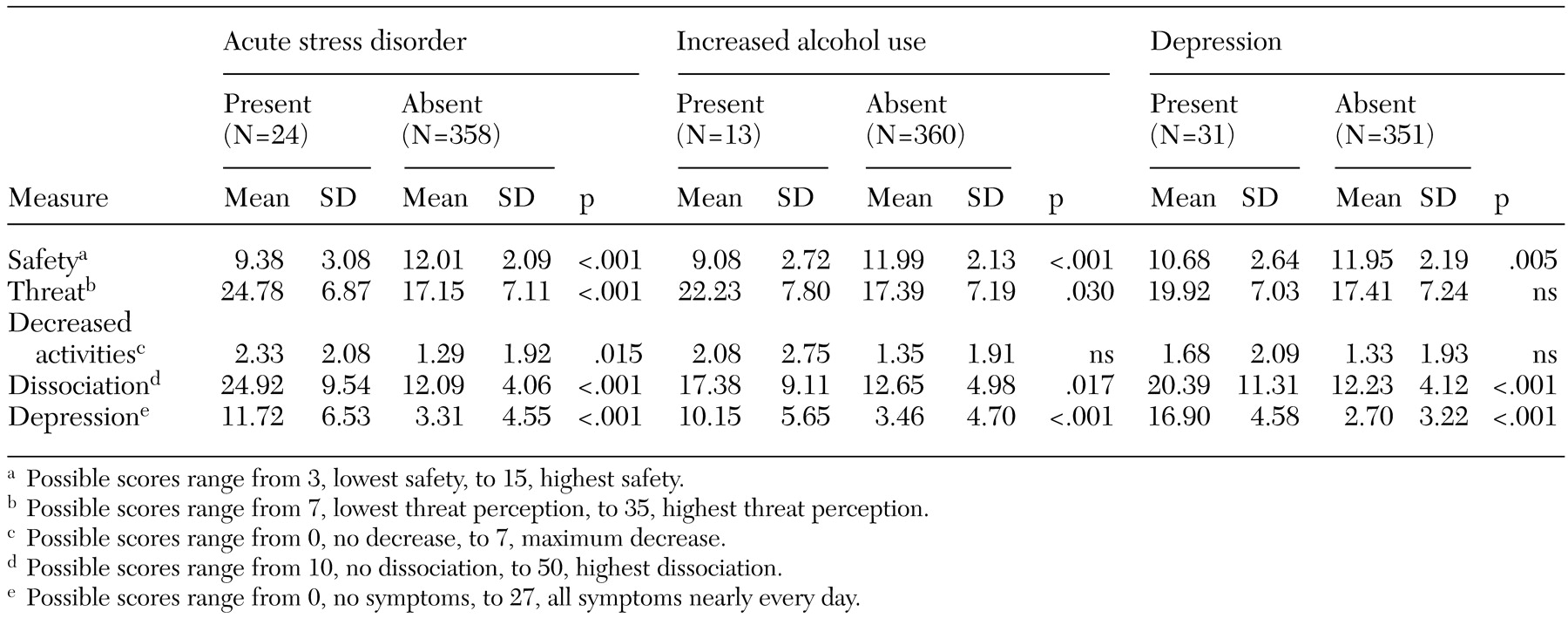
Acute stress disorder. Acute stress disorder was assessed for the week before the survey with use of the previously validated Acute Stress Disorder Inventory (
10). This inventory requires endorsement of symptoms of intrusion, avoidance, hyperarousal, and dissociation in accordance with
DSM-IV criteria.
Alcohol use and abuse. Presence of previous substance abuse was assessed with use of the CAGE questionnaire, with responses directed to the year before October 2002. The cutoff score of 1 was used to identify possible substance use problems. This cutoff score provides a sensitivity between .86 and .90 and a specificity between .52 and .93 (
11). Alcohol use since October 2 was assessed with one question, "Did you increase your alcohol use for a period of two weeks or more?"
Depression. Depression was assessed with use of the Patient Health Questionnaire Depression Scale (PHQ-9) (
12). A person is considered to be depressed when five or more of the nine symptoms have been present for more than half the days in the previous two weeks and one of the symptoms is depressed mood or anhedonia. Severity of depressive symptoms was measured with the sum of the responses to the PHQ-9, with nine items scored from 0, not at all, to 3, nearly every day, for a total score ranging from 0 to 27. A score of 10 or more indicates the potential need for treatment.
Peritraumatic dissociation. Peritraumatic dissociation was scored with use of an abbreviated version of the Peritraumatic Dissociative Experiences Questionnaire (PDEQ), with endorsement of symptoms ranging from 1, not at all true, to 5, extremely true (
13). The full scale was used in a previous study with a similar population of persons who had been exposed to the September 11, 2001, attack on the Pentagon (
14). Analysis of those data showed that Pearson correlations between the first five questions and the total score ranged from .62 to .83. The Pearson correlation between the five-item abbreviated scale and the ten-item scale was .97 (p<.001, Cronbach's alpha=.84). The score of the abbreviated scale was adjusted to produce a score consistent with the original ten-item scale (ranging from 10, no symptoms, to 50, high dissociation).
Perceived safety, perceived threat, and changes in activity. Respondents' general sense of safety was assessed with use of the Perceived Safety Scale. This scale was previously used in the study of the survivors of the Pentagon attack. The scale uses a total score from three questions: safety at work, safety at home, and safety throughout the day in usual activities and travel. Each item is scored on a 5-point Likert scale ranging from 1, not at all, through 5, extremely, with a range for the overall scale of 3, low safety, to 15, high safety (Cronbach's alpha=.78).
Perceived threat was assessed by using seven questions in which respondents were asked to rate the impact of the sniper attacks on their degree of concern about routine activities for themselves and their family—being in public places, buying gas, sending children to school or to extracurricular activities, attending large public gatherings, traveling by public transportation, traveling by car, and attending faith-based activities. Each item was scored on a 5-point Likert scale ranging from 1, none, through 5, extreme, with a range for the overall scale of 7, low perceived threat, to 35, high perceived threat (Cronbach's alpha=.92). Change in activity level was assessed with use of the same routine activities with choices of decrease, no change, increase, and not applicable. The number of activities decreased per person was totaled for a score ranging from 0 to 7.
Health care use. Use of health care services was assessed with two questions. One question asked for the number of visits to health care providers since the first sniper attack. Another question asked about the number of visits to mental health care providers since the first attack. Responses to these questions were converted to binary variables ("some visits" or "no visits").