Depression can have a serious impact on cognitive, social, and physical functioning (
1). The United States loses between $30 billion and $44 billion in direct medical, mortality, and productivity costs each year as a result of depression (
2,
3,
4). Moreover, studies show that depression is related to work impairment (
5), disability and lost work days (
6,
7,
8,
9), and reduced productivity on the job (
10).
Many effective treatments and management protocols are available to ease the symptoms of depression (
11,
12,
13,
14), although only about 20 percent of persons with major depression are adequately treated (
15). Depression treatment has also been shown to be cost-effective (
16), to keep depressed persons employed (
17,
18), and to improve the productivity of depressed persons who are already working (
19). Moreover, it has been hypothesized that the amount of money saved by treating depressed workers could result in savings to employers that would more than make up for the costs of treatment (
20,
21,
22,
23).
Consequently, in this cross-sectional study we used a large nationally representative sample of depressed persons to examine the sociodemographic, health, functional, and disability characteristics of persons who work and those who do not work. The purpose of the study was to compare working depressed persons and nonworking depressed persons and to identify the factors that are associated with depressed persons' working.
Methods
Data source
We used data from the 1994 and 1995 National Health Interview Survey Disability Supplement (NHIS-D) to identify persons with depression. The NHIS is an annual survey sponsored by the National Center for Health Statistics (
25). The NHIS-D was a special supplement to the NHIS core. The supplement was administered during 1994 and 1995 and collected detailed information on functional limitations, limitations in daily activities, disability, and mental health.
NHIS data were obtained by in-person interviews of household members. Interviews were conducted with a probability sample of households by using a stratified multistage probability design (
25). A total of 107,469 persons were in the 1994 sample, and 95,091 persons were in the 1995 sample.
Population
All working-age persons, aged 18 to 69, were included in the study. Persons were considered to have depression if they responded "yes" to the question "During the past 12 months, did [you or the household member] have major depression? Major depression is defined as 'depressed mood and loss of interest in almost all activities for at least two weeks.'"
Variables
Working was defined as participation in the labor force. Participants in the labor force included those who were currently employed and had worked in the past two weeks; those who had a job but had not worked in the past two weeks, for example, were not on layoff or looking for a job; and those who were looking for a job or who had been laid off.
Disability was examined in two ways. We used the NHIS-D variable on ability to work to examine four possibilities: unable to work, limited in the amount or kind of work a person could perform, limited in other activities, and not limited. We also defined disabled by using a two-part algorithm: answering "yes" to the question "Does any impairment or health problem keep [you or the household member] from working at a job or business?" and reporting not working in the past two weeks. In other words, disability was an impairment or health problem affecting the ability to work and not working in the past two weeks.
Self-reported health status was operationalized with the question "Would you say [your or the household member's] health in general is excellent, very good, good, fair, or poor?" A person was considered to have an attributable health condition if a condition was reported as the main or secondary cause of inability to work or of limitation in working. Additionally, an attributable health condition was defined when it was reported as the cause of a problem with an activity of daily living—for example, bathing, dressing, or eating—or an instrumental activity of daily living—for example, preparing meals, managing money, or grocery shopping—or as the cause of a functional limitation—for example, a social, cognitive, or physical limitation. The number of attributable health conditions reported for each person was then summed.
A person with social limitations was described as having trouble making or keeping friends, a lot of trouble getting along in social settings, or serious trouble coping with day-to-day stresses (
26). A person was deemed to have cognitive limitations when that person was described as having a lot of trouble concentrating for long enough to complete tasks or as being frequently confused, disoriented, or forgetful (
26). To be included as a cognitive or social limitation, the problem had to interfere seriously with the person's life. A person with a physical limitation was described as having one or more problems with activities of daily living or as having one or more physical functional limitations—for example, lifting something as heavy as ten pounds, walking about a quarter of a mile, or holding a pen—or as being in fair or poor health (
26).
Sociodemographic characteristics included age, gender, race, residential description, that is, urban and suburban areas versus rural areas; living arrangement; and education level. For the purpose of our study, urban and suburban areas were grouped together, because access to and type of treatment for these areas are likely different than for rural areas. It was hypothesized that job flexibility would be an important factor in the association between working and not working for depressed persons (
27). Such flexibility might provide a depressed person with the ability to work reduced hours, rearrange work schedules and work procedures, and take time off during depressive episodes. We used education level as a proxy for job flexibility. In addition, for persons who were in the labor force, we categorized the reported job into categories that appeared to be related to job flexibility: white collar, for example, executive, administrative, and managerial occupations; blue collar, for example, farming, forestry, fishing, transportation, handlers, and laborers; and a middle category that could not be categorized as either white or blue collar, for example, sales, protective services, and other service jobs. White collar jobs were considered to be more flexible than blue collar jobs.
Statistical analysis
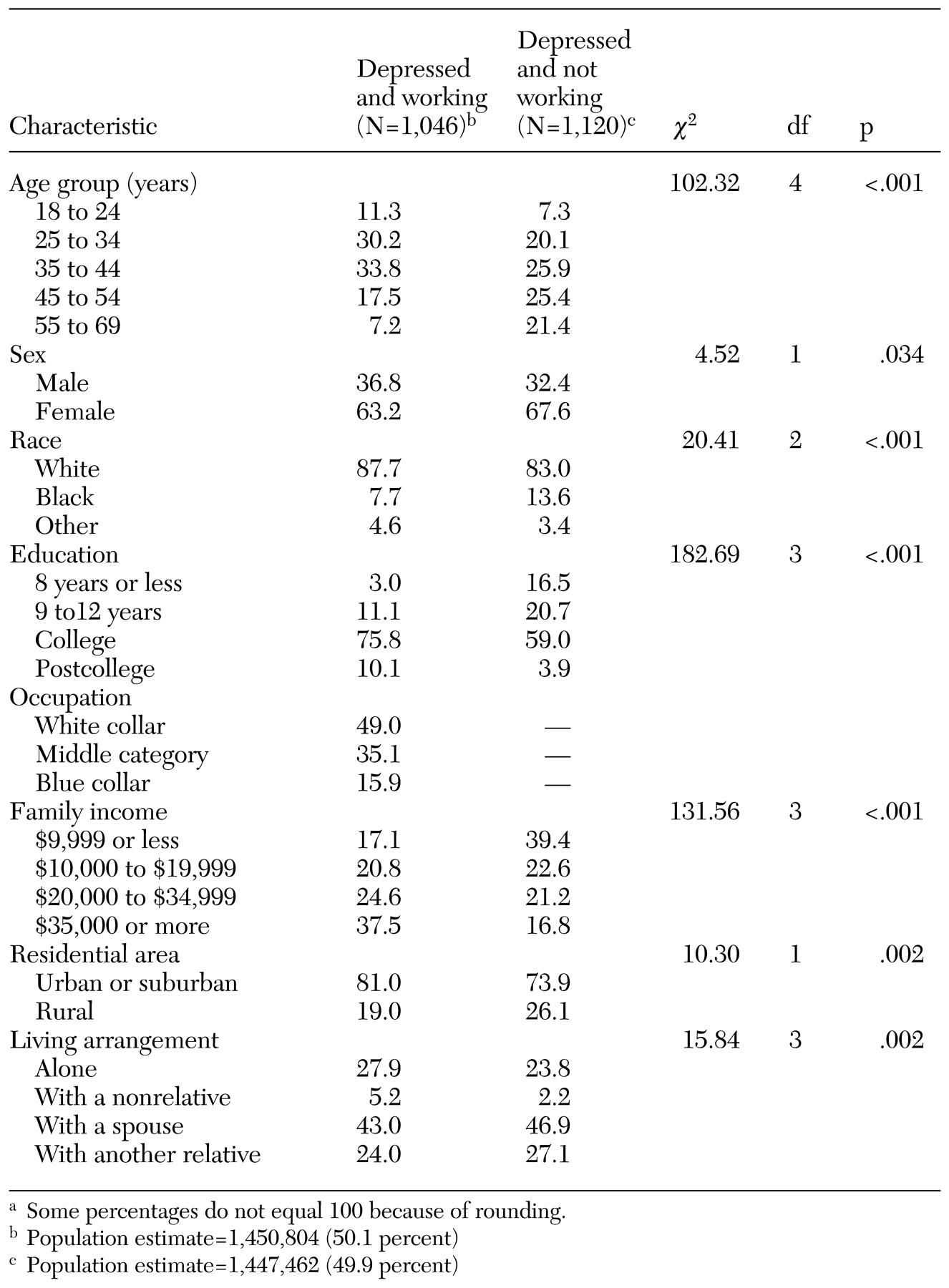
We calculated population estimates of employment and disability status among depressed persons. We then compared working depressed persons with nonworking depressed persons by sociodemographic, disability, health, and functional characteristics by using a chi square statistic.
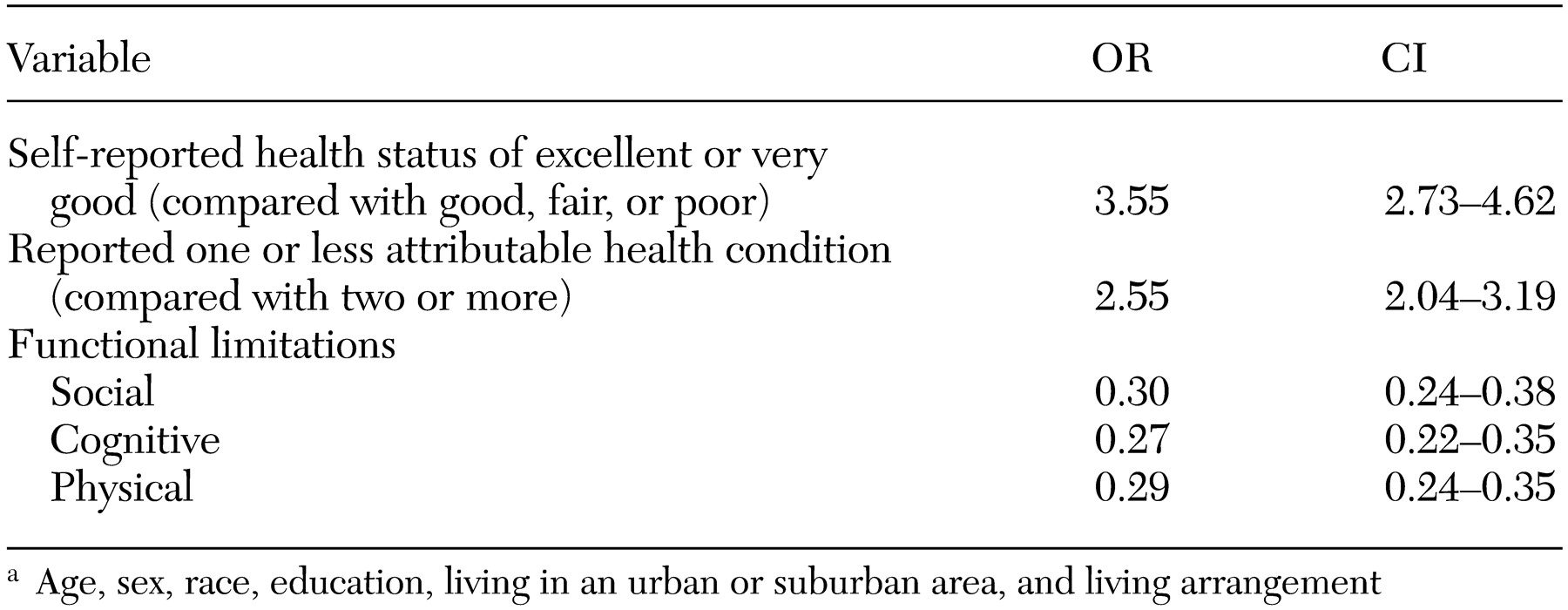
Finally, we conducted a multiple logistic regression analysis by using labor force participation as the dependent variable. Independent variables consisted of sociodemographic characteristics in one model. We then produced separate models for each health and functional characteristic while adjusting for sociodemographic characteristics. Odds ratios and 95 percent confidence intervals are presented.
In order to provide nationally representative estimates and to account for the complex survey design, all analyses used the SUDAAN statistical package, release 7.5, with appropriate weighting.
Discussion
Currently, considerable evidence exists to demonstrate the serious impact that depression can have on the ability to work, absenteeism, and workplace productivity, as well as the usefulness of depression treatment to reduce depressive symptoms and improve function and employment. An understanding of the characteristics of persons with depression who are unable to work or who continue to work at reduced productivity may assist in the development of programs to improve access to health care and adherence to depression treatment.
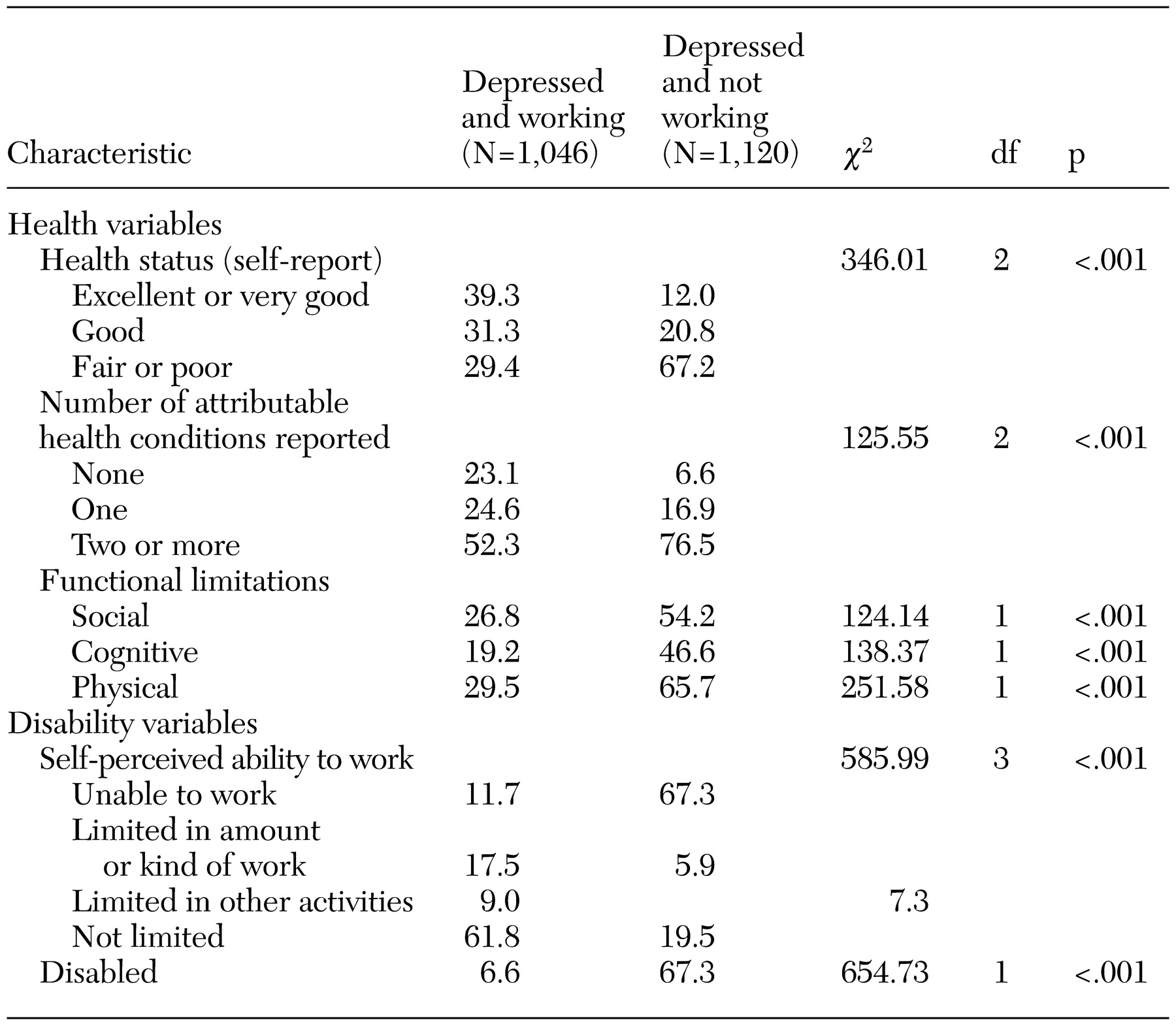
Our study found that approximately half of the estimated 2.9 million people who considered themselves to have major depression participated in the labor force and showed that depressed persons who work and who do not work are considerably different. Compared with depressed persons who do not work, depressed persons who work are significantly more likely to be younger, to be male, and to be better educated, to have a higher income, to live alone or with a nonrelative, and to live in an urban or suburban location. A large percentage of depressed persons who are employed work in white collar jobs and are less likely to perceive themselves as unable to work or to be disabled. Finally, depressed persons who work are healthier than their nonworking counterparts. Working depressed persons perceive themselves to have a better overall health status, report fewer health conditions that limit their ability to work or to perform activities of daily living and instrumental activities of daily living, and have fewer social, cognitive, and physical limitations than nonworking depressed persons.
In addition to this composite of depressed persons who work, we found that health status and education level were strongly associated with depressed persons' working, even after controlling for other related factors, such as age, gender, race, living arrangement, and residential area. Depressed persons who perceived themselves to be in excellent or very good health were 3.6 times as likely to be in the labor force as those who perceived themselves to be in good, fair, or poor health. Those with one or no attributable health conditions were 2.6 times as likely to work as those with two or more attributable health conditions. Those who reported at least one social, cognitive, or physical limitation were about one-third as likely to be in the labor force as those who did not report these limitations.
This study had some weaknesses. All information obtained in the NHIS-D was based on self-report or from a knowledgeable adult reporting for absent members of the family (
25). Depression may have been underreported as a result of stigma or failure to recognize or accept depression in oneself or in a family member.
Identification of depression was based on a single-item question. From this question, it was estimated that 1.7 percent of the population aged 18 to 69 had been depressed in the past 12 months. The National Comorbidity Survey found a 12-month prevalence of major depression of 6.6 percent among persons aged 18 and older when using a modified version of the Composite International Diagnostic Interview (
15). The Epidemiologic Catchment Area study of five communities found a cross-site mean for major depression for the past month among adults aged 18 and older of 1.6 per 100 persons when using the Diagnostic Interview Schedule, a highly structured interview designed for use by lay interviewers in epidemiologic studies in which items were consistent with the
DSM-III definition of depression (
28). Our results were more consistent with those of the Epidemiologic Catchment Area study, even though our results were based on a less sophisticated method for identifying depression and used a working-age group of adults. However, unlike the Epidemiologic Catchment Area study, our study could not make distinctions between level of depression severity, and it was based on reports of depression in the past 12 months.
Although the NHIS-D did not provide specific information on job flexibility, the finding on the relationship between education and work status among depressed persons is consistent with the hypothesis that job flexibility may be associated with work status among depressed persons. Further studies will need to elucidate this issue with more direct questioning on the subject.
Despite the above limitations, this study had a number of strengths. Data from the NHIS-D provided a large sample for studying depressed persons who work and who do not work. In addition, this sample is representative of the U.S. population, with a few exceptions, so that conclusions can be drawn for the general population. Persons excluded from this sample were patients in long-term-care facilities; persons on active duty with the U.S. Armed Forces, although their dependents were included; and U.S. nationals living in foreign countries (
25). Excluding patients in long-term-care facilities may exclude the elderly population, which should not have interfered with our study's results, because the cutoff in this study was 69 years of age to examine the working-age population.
The health status and functional variables were consistently related to work status among depressed persons. Although it could be argued that the health status and functional limitation measures may be proxies for severity of depression rather than for independent risk factors, our findings on depression were consistent with findings from studies of other chronic diseases (
29,
30,
31). For example, in an analysis of the same NHIS-D database to determine the factors associated with employment among all persons with disabilities, Zwerling and colleagues (
29) found several sociodemographic variables, such as age, race, and education, to be associated with workforce participation, as well as with perceived health status and difficulties with activities of daily living and instrumental activities of daily living. In another study, Yelin and Katz (
30) used the NHIS data for the period 1970 to 1987 and found that the labor force participation rate was higher among persons with activity limitation and musculoskeletal conditions only when compared with those with musculoskeletal conditions plus other chronic conditions. Finally, in a study of musculoskeletal conditions in a population aged 51 to 61, Yelin (
31) found that persons with musculoskeletal conditions and no comorbid conditions were less likely to have a work disability than persons with musculoskeletal conditions plus other comorbid conditions. Moreover, a multiple logistic regression analysis indicated that work disability was related to comorbidity, older age, being female, and having less education and fewer functional limitations (
31).
Our study found that at least 1.7 percent of the working-age population was depressed within the past 12 months—an estimated 2.9 million individuals. However, this finding does not include persons whose depression was in remission in the past 12 months or whose depressive episode may have occurred before this 12-month period. Moreover, despite the fact that nearly 50 percent of depressed persons reported that they were in the labor force, nearly 30 percent of depressed persons who worked considered themselves unable to work or limited in the amount or kind of work that they could do. This amounts to a substantial proportion of depressed persons in the labor force who may be in need of improved treatment or better access to treatment.
Conclusions
The populations of depressed persons who work and who do not work are clearly different along important parameters. These populations differ in virtually every sociodemographic characteristic, as well as by health status, functional status, and disability characteristics. Factors strongly associated with depressed persons' working are related to their health and functional status, with education level also playing an important contributory role in the likelihood of a person with depression continuing in the workforce. In particular, it may be important to focus on individuals with depression and comorbid general health conditions.
The results of this study help to underscore the societal burden from depression by confirming the large number of depressed persons in the U.S. population. Health care policy makers need to be aware of the cost-effectiveness of depression treatment and the increased likelihood of employment with improvement in depressive symptoms. Employers need to be aware that although at least half of the working-age population who are depressed will continue to work, depression can have a serious effect on the workplace in terms of absenteeism, short- and long-term disability costs, and lower productivity. Employers may wish to develop programs to identify persons who are depressed and to ensure, through benefits packages and health insurance, that depressed persons will receive effective treatment. A better understanding of the characteristics of depressed persons who work and the factors associated with continuance in the labor force will help to shape health care benefit packages, employee assistance programs, disability programs, and treatment programs. Such interventions will be of benefit to workers and employers alike.