Delphi consultation
The Delphi consultation method, developed by the RAND Corporation in the 1950s (
13), is used to obtain consensus, especially in areas in which there is little other evidence. Members of a panel of experts anonymously respond to specific questions about a particular problem. Their responses are analyzed and fed back to the same experts in the next consultation round. This iterative consultation provides an opportunity for the experts to reevaluate their opinions in light of the average ratings of the group (
14). The result of a Delphi consultation is a composite of the group's expert knowledge. The three main features of the method are anonymity, iteration, and controlled feedback (
15). The method has been effectively used to identify the components of assertive community treatment (
11,
16) and to determine the threshold of severity of mental illness in making decisions about access to mental health services (
17).
A literature search informed the questions for the Delphi consultation. The search used MEDLINE, PsycINFO, EMBASE, and OVID, using the terms "forensic," "community." and "mental health." We also hand searched for relevant cross-referenced articles. Using information abstracted from the literature review, we developed a list of candidate categories for defining integrated and parallel service models, including staffing, supervision arrangements, organization of referral meetings, links with other services, and the method of funding. The study was conducted between September 2002 and June 2003.
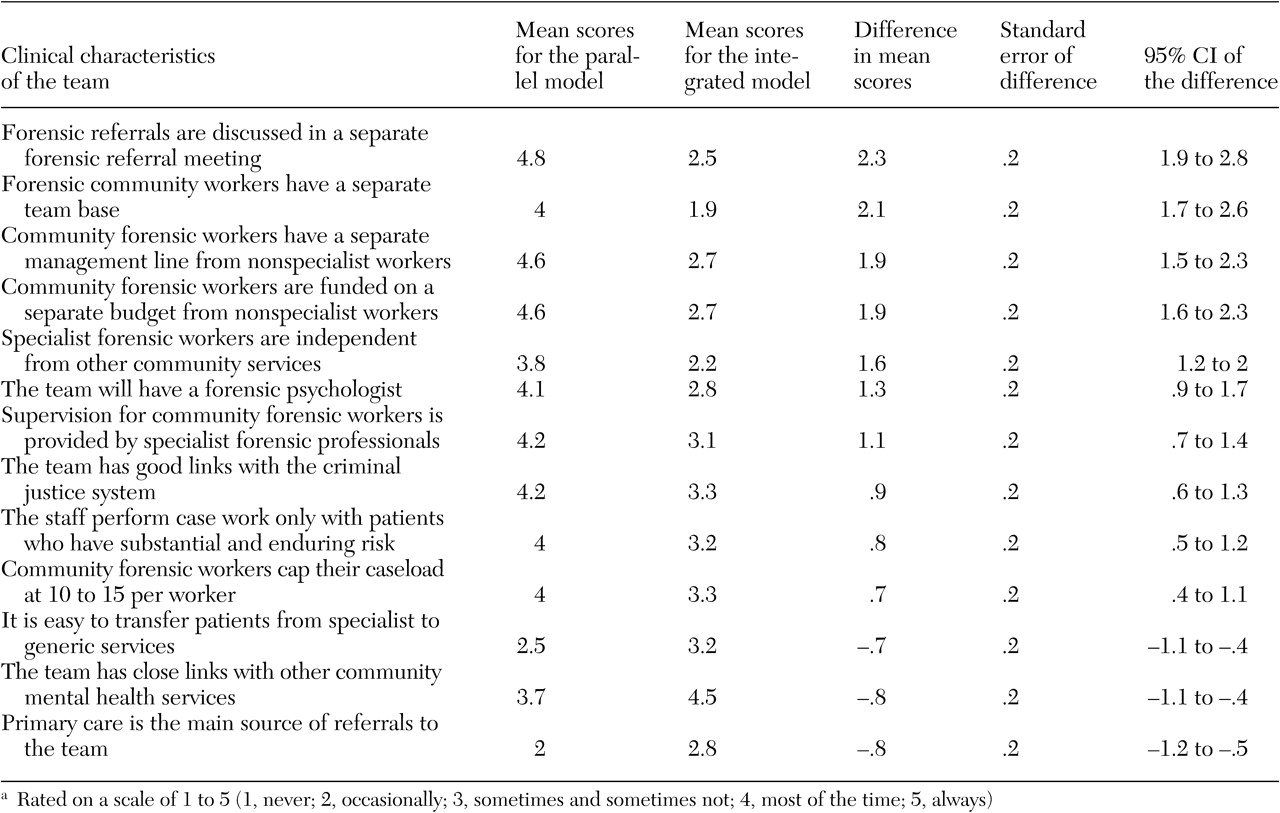
A focus group was then conducted to validate the preliminary characteristics identified from the literature review and to identify other characteristics of community forensic teams. The ten-member group included three forensic psychiatrists, three forensic nurses, two service managers, one forensic psychologist, and one general psychiatrist who worked closely with forensic teams from local services. The focus group discussions were audiotaped, transcribed, and analyzed to identify the themes that indicated the service characteristics of the two models. Focus group participants were asked to comment on a written summary of the discussion and to provide terms or phrases to label the key characteristics of the two service models. This approach ensured that the terminology used in the questionnaire came from the participants. In the first-round questionnaire we applied the 31 service characteristics separately to both integrated and parallel models, resulting in a total of 62 statements. This approach enabled the panelists to rate the two models on each of the characteristics separately. The items were rated on a scale of 1 to 5, with 1 indicating never; 2, occasionally; 3, sometimes and sometimes not; 4, most of the time; and 5, always. The questionnaire was piloted to ensure conceptual clarity and wording of the questions.
The panel members were selected from around England from specialist forensic teams and generic teams with forensic specialists from local services and through a snowballing sampling technique, to identify professionals who had at least five years of experience working with mentally ill offenders in the community. We chose this method rather than constituting this panel randomly to help ensure that the panel had specialist expertise in managing mentally ill offenders in the community.