Managed care has reduced the mean length of stay for psychiatric hospitalizations (
1,
2), which has resulted in decreased costs and has raised concerns about the quality of care (
3,
4,
5,
6,
7,
8). There are no commonly accepted length-of-stay guidelines for inpatient care of psychiatric conditions, as there are for some medical conditions, and the length of inpatient psychiatric treatment could be subject to substantial variation (
9).
Studies that have evaluated the relationship between length of stay and rate of readmission have reported contradictory results. Wickizer and colleagues (
7) reported that children and adolescents whose length of stay was restricted by utilization management were more likely to be readmitted. More recently Heeren and colleagues (
6) observed that in a psychogeriatric unit, when length of stay decreased the readmission rate increased. Another study found that patients with schizophrenia who were discharged before 30 days of admission had higher recidivism rates (
13). On the other hand, some studies did not find a negative correlation between length of stay and readmissions (
14,
15)—that is, a shorter stay with a higher readmission rate—and some studies even found a positive correlation between length of stay and readmissions (
16,
17,
18)—that is, a shorter stay with a lower readmission rate.
Because patients are not randomly assigned to groups with shorter or longer hospital stays, it is difficult to make causal inferences about length of stay and readmission rate. A potential selection bias exists, because patients who stay longer in the hospital are more likely to be sicker or homeless or to lack social supports. Patients who are hospitalized longer could also be more likely to be readmitted, not because of the longer length of stay but because of these other factors that are positively correlated with longer stays and higher rates of readmission. Because of this positive bias, the negative effect of length of stay on readmission rate could be underestimated, or if the positive bias is larger than the therapeutic impact of length of stay on readmission rate, the effect could be inverted and a positive effect of length of stay on readmission rate could be found.
Methods
Data
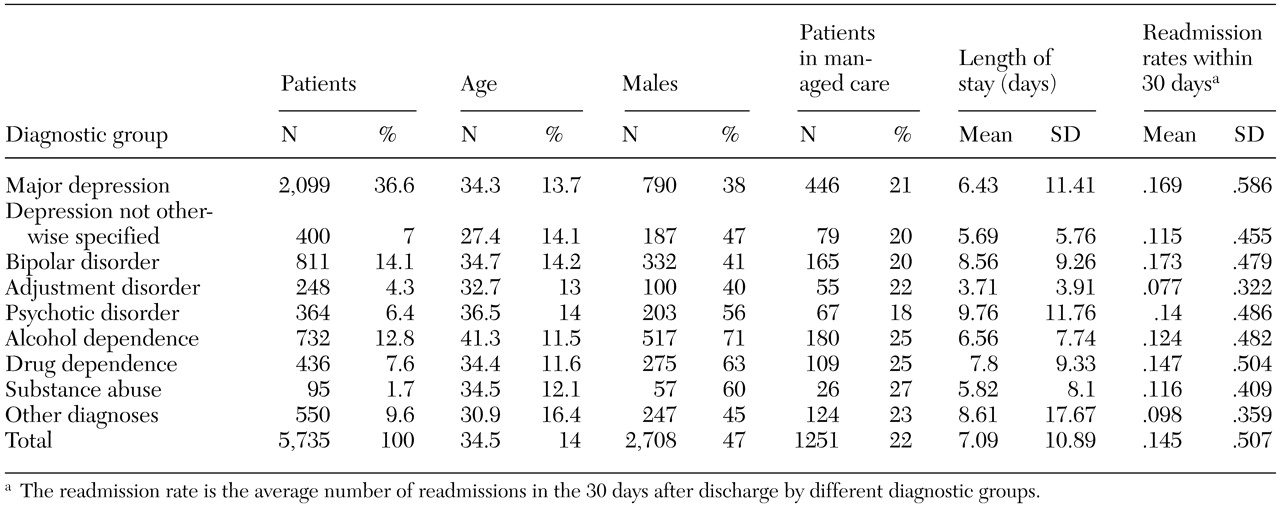
We used the MarketScan data set collected by Medstat. Medstat is a health care information company that provides market intelligence and benchmark databases for managing the cost and quality of health care. The MarketScan data set included claims data on hospitalizations from 5,735 persons across the United States who had one or more discharges with a primary psychiatric diagnosis during 1997 and 1998. These data were not intended to be nationally representative. The data set included only information from employer-based private health insurance companies that share their data with Medstat. A disproportionately high percentage of the discharges analyzed occurred in Michigan (24 percent), Massachusetts (11 percent), Georgia (9 percent), and Florida (8 percent).
Inpatient hospitalizations with a primary diagnosis of a psychiatric disorder were identified by using International Classification of Diseases, 9th Revision clinical modification codes.
We created dummy variables for patient demographic characteristics; diagnostic categories, for example, psychotic disorders, adjustment disorders, major depression, and bipolar disorder; and the type of primary payer, that is, whether patients used a fee-for-service plan or a managed care plan. For patients who had more than one admission for a psychiatric disorder during this two-year period, we used information on these characteristics from the first admission. Also, for patients with multiple admissions, we calculated length of stay only for the first admission. We counted the subsequent number of readmissions that each patient had during the 30 days that followed the index hospitalization. Hospitalizations that ended during December 1998 were used to identify readmissions but were otherwise excluded from the analyses.
Patient characteristics
Patients were classified as living in an urban or a rural metropolitan statistical area, as defined by the Bureau of the Census and the U.S. Office of Management and Budget, and by the type of primary payer. Gender and age were also included as variables in the analyses.
Statistical analyses
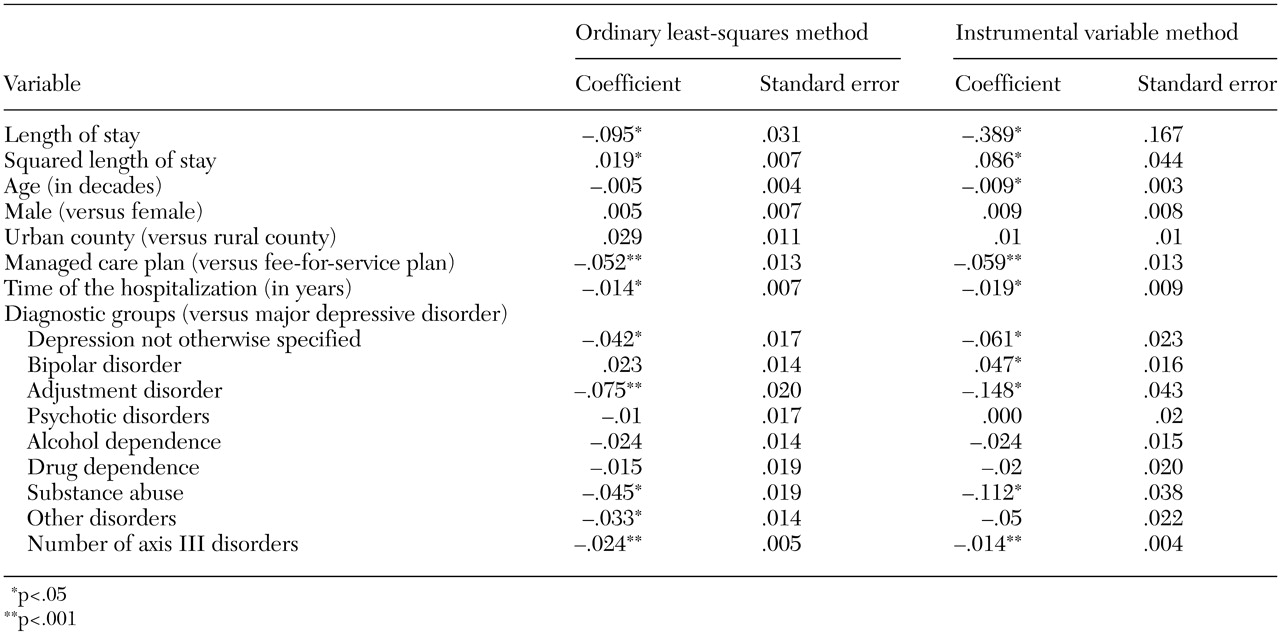
Because ordinary least-squares analyses would give a biased estimate of the impact of length of stay on readmission rate, a two-stage regression that used instrumental variables was necessary. If length of stay was correlated with unobserved severity of the illness (that is, a higher suicide risk or poorer social supports, which are not accounted for in the diagnostic information available in administrative data and would influence the readmission rate), any estimated impact of length of stay on readmission could actually result from severity of illness, as opposed to length of stay. A standard method for correcting this problem is the instrumental variable method (
20). With this method, instead of using length of stay as an explanatory variable in the regression, we used the predicted value of length of stay. In order to have a useful value of the predicted length of stay, it was necessary to use a variable that strongly predicted length of stay—that is, a variable that worked as a proxy for length of stay—but that did not have a direct impact on the readmission rate. This variable is called the instrumental variable. The two stages of the technique are two regressions. In the first one, the instrumental variable was used to predict length of stay. In the second regression, the predicted value of length of stay—from the first regression—was used as an explanatory variable for readmission rate. In both regressions, we also controlled for demographic characteristics and diagnostic information.
We used as the instrumental variable the mean length of stay for all psychiatric admissions in the zip code of the hospital where the hospitalization occurred. This mean length of stay is a good instrumental variable because the mean length of stay at the regional level has a direct and strong impact on the length of stay for a particular patient, and it does not directly affect the readmission rate.
Because admissions in the same region are not completely independent events, we corrected the standard errors for clustering by hospital zip code. Alternatively, we also ran an ordinary least-squares regression analysis, controlling for demographic characteristics and diagnostic information, to compare this estimation with the instrumental variable method model.
Because both length of stay and readmission rate had very skewed distributions, before running the ordinary least-squares regression or the two-stage instrumental variable method model, we transformed length of stay to its logarithm and transformed readmission rate by adding 1 and then taking its logarithm. Because of these logarithmic transformations, when we obtained the predicted values of readmission rate for each value of length of stay, we adjusted the estimations by multiplying by a smearing factor (
21). Because we found heteroscedasticity of the residuals in the regression of readmission rate on length of stay, we obtained a different smearing estimate for each possible length of stay (
22).
Discussion and conclusions
In this study we estimated the impact of length of stay for psychiatric hospitalizations on readmission rates by using two alternative methods. First, using ordinary least-squares analyses, we found that length of stay and readmission rate were significantly negatively correlated. As noted above, we believe that because of the problem of self-selection, patients who are sicker are more likely to have longer admissions and more readmissions, and thus the ordinary least-squares analyses estimation would have a positive bias. Despite this positive bias, we found a negative impact of length of stay on readmission rate. Thus this method underestimated the impact of length of stay on readmission rate. To address the self-selection bias, we used a two-stage instrumental variable model, and, as predicted, we found that the negative impact of length of stay on readmission rate was even larger. In both models, we found that the effect of length of stay on readmission rate is not linear. Changes in length of stay had a significantly larger impact on readmission rate when length of stay was shorter.
The results of previous studies contradict our findings. Two studies found that patients with multiple admissions had significantly longer stays (
16,
17). A study by Kessing and colleagues (
18) found that patients with affective disorders whose admissions were longer had higher rates of readmission. Another study by Lyons (
14) examined predictors of readmission for 255 patients who were admitted to seven different hospitals in a regional managed care program and found no evidence that premature discharge was associated with readmission risk. These studies controlled for severity of illness to various extents, but the source of variation in length of stay was from unobserved factors that are subject to self-selection. The results of these studies are consistent with our argument that estimating with ordinary least-squares analyses gives biased estimations. This bias is explained by the fact that both length of stay and readmission rate are indicators of, or correlated with, the severity of illness.
Previous studies have also postulated that the regulations of managed care plans that decrease length of stay for inpatient treatment of depression could have a negative impact on outcomes. In 1998 Wickizer and Lessler (
23) analyzed the effect of shortening length of stay and found that patients whose hospitalizations were restricted by utilization review had higher rates of readmission during the 60 days following discharge. In addition, Heeren and colleagues (
6) recently reported a temporary association between decreasing length of stay and increasing readmission rate in a psychogeriatric unit. It should be noted that severity of illness, which is an important source of variation in length of stay, was not a factor in these studies. Variation was attributable to utilization reviews (
23) or to when the hospitalization occurred (
6), and therefore self-selection played a less important role in the determination of length of stay. When comparing the outcomes of patients that had short or long hospitalizations, it is important to understand what determined the length of stay. The ideal design for causal interpretation is when the length of stay is determined randomly and thus is not correlated with severity of the illness. In nonexperimental, natural settings one of the major determinants of length of stay is the severity of the illness, not external factors, such as utilization reviews, changes in hospital policies over time, or randomization of patients into groups. Therefore, it is very likely that the patients who stay longer are sicker. This produces the most biased results. We believe that in two studies (
6,
23) the results were less likely to be biased, because the determination of hospitalization stay was due to specific external reasons that were less likely to be correlated with severity of the illness (that is, utilization reviews or changes in the targeted length of stay over the time of the study, which could be due to managed care or hospital policies). In other words, patients who stayed longer did so, at least in part, because of external reasons (that is, less strict review practices or being hospitalized in a year when all hospitalizations were longer) and not necessarily because they were sicker.
The mechanisms by which longer inpatient stays reduce the readmission rate are beyond the scope of this study. Patients who are allowed to have longer stays are likely to be more stable at the time of discharge, to be better engaged, and to be more likely to follow up with outpatient care. The specific mediators of the effect of length of stay on readmission rate need to be further studied and eventually be set as goals of inpatient psychiatric treatment, regardless of how these mediators would affect the length of stay. Stabilizing the patient and having appropriate discharge planning before discharge are already well-known goals of inpatient treatment teams, and it is possible that we found a sharp increase in the readmission rate among patients with shorter stays because excessively short stays—that is, less than four or five days—make these goals unlikely to be accomplished successfully.
Our study has several limitations. Administrative observational data are subject to certain inherent limitations. Even though we believe that using the instrumental variable method could give us a better estimate of the impact of length of stay on readmission rate than has been previously reported, our calculations are subject to assumptions and do not replace being able to randomly assign persons to groups that have longer or shorter stays. If the mean length of stay at a hospital (identified by zip code) was correlated with other unobserved variables that were themselves correlated with higher readmission rates, our estimations would be biased. Because a higher mean length of stay can result from greater severity of illness or drug and alcohol dependence in the area, we determined whether any correlation existed between these possible sources of bias and the mean length of stay in a particular hospital (identified by zip code) and found none. The actual source of bias would be the unobserved variables—severity of illness or substance dependence—which we could not test for. However, the fact that the observed severity indicators were not correlated with the mean length of stay is encouraging.
A further limitation intrinsic to administrative data analyses is the lack of direct clinical assessments of the outcomes. Inpatient readmissions are a common but controversial measure of outcomes in psychiatry (
4,
10). We argue that a readmission is an adverse outcome because of its cost to the providers, patients, and society and because it shows that other less restrictive treatments have failed or that the safety of the patient is at risk (
11,
12). We believe that the controversy about the use of readmission rate and other outcome measures that are related to service use is due, in part, to studies that have tested the utility of readmission rates without addressing the problem of self-selection (
14). We also agree that readmission rate or other use of services would not be a good outcome measurement if the problem of self-selection as a factor in the variation of length of stay were not addressed. Finally, although the data were drawn from hospitals across the United States, the sampling strategy was not designed to produce nationally representative estimates. It is possible that the association between length of stay and readmission rate found in this study is not be generalizable to all hospitals.
In summary, the continuous decrease in length of stay for inpatient psychiatric treatment could be deleteriously affecting outcomes of treatments for psychiatric disorders, and studies that do not address the problem of self-selection are misleading. Further studies that use different data sets and different instrumental variables are necessary to better identify the impact of length of stay on readmission rates.