The September 11, 2001, terrorist attack on the Pentagon left 125 Pentagon employees dead. The explosion and fire caused massive damage and placed many at risk of injury and death.
We previously studied one of the commands at the Pentagon seven months after the attack (
1). We found that among 77 responding staff members, 14 percent had possible posttraumatic stress disorder (PTSD), with higher rates of PTSD among women. PTSD was more likely to occur among staff members who had higher levels of peritraumatic dissociation, greater initial emotional response, and lower perceptions of current safety.
The study reported here assessed current symptoms of PTSD and major depression as well as current safety perceptions in a sample of Pentagon staff members 13 months after the attack. We examined the relationship between work location on the day of the attack, PTSD, and major depression. We also examined the relationship of each of these variables to perceived safety.
Methods
Thirteen months after the Pentagon attack and after approval by the Uniformed Services University of the Health Sciences' institutional review board, we sent an electronic questionnaire to approximately 680 staff members in one of the Pentagon commands. Prospective participants were notified of the voluntary nature of the study, potential risks and benefits, and alternatives to participation. They were also informed about how to obtain a referral for care if desired. The institutional review board waived the requirement for written informed consent.
The Impact of Events Scale—Revised was used to identify possible PTSD (
2). We created a binary indicator of possible PTSD—including possible subsyndromal PTSD—based on endorsement of symptoms that followed the
DSM-IV criteria of one intrusion symptom, three avoidance symptoms, and two hyperarousal symptoms (
1,
3,
4).
Probable major depression was assessed with the Patient Health Questionnaire Depression Scale (
5). Major depression was noted when five or more of the nine symptoms had been present "more than half the days" in the past two weeks and when one of the symptoms was depressed mood or anhedonia.
Perceived safety was assessed by using a total score from three questions about safety at work, safety at home, and safety throughout the day in usual activities and travel (
1). Each item was scored on a 5-point Likert scale: 1, not at all; 2, a little bit; 3, moderately; 4, quite a bit; and 5, extremely. Possible scores ranged from 3 to 15 (Cronbach's alpha=.83). Each question was also separately examined against the other variables.
Participants who were at the Pentagon or the two nearby office buildings during the attack were rated as being in the high-exposure group. Participants who were out of town, were at home, worked at other locations in the area, or had moved to the area after the attack were rated as being in the low-exposure group.
Risk factors for PTSD and major depression were evaluated by using binary logistic regression, with variables entered individually and with analysis of covariates when appropriate. The estimate of the odds ratio (OR) and its 95 percent confidence interval (CI) are reported. The Mann-Whitney test was used to evaluate differences in means for continuous variables. Statistical analysis was performed by using SPSS for Windows, version 11.
Results
We received 212 responses over the Internet. A total of 142 respondents (67 percent) were men, and 142 respondents (67 percent) were married. The respondents' mean±SD age was 39.4±10.1 years. The group was predominately white (158 respondents, or 75 percent).
A total of 120 respondents (57 percent) were in or near the Pentagon at the time of the attack, and the remainder (92 respondents, or 43 percent) were elsewhere in the metropolitan area or out of town. Forty-eight respondents (23 percent) met criteria for possible PTSD, eight (4 percent) met criteria for probable major depression, and seven (3 percent) met criteria for PTSD and major depression.
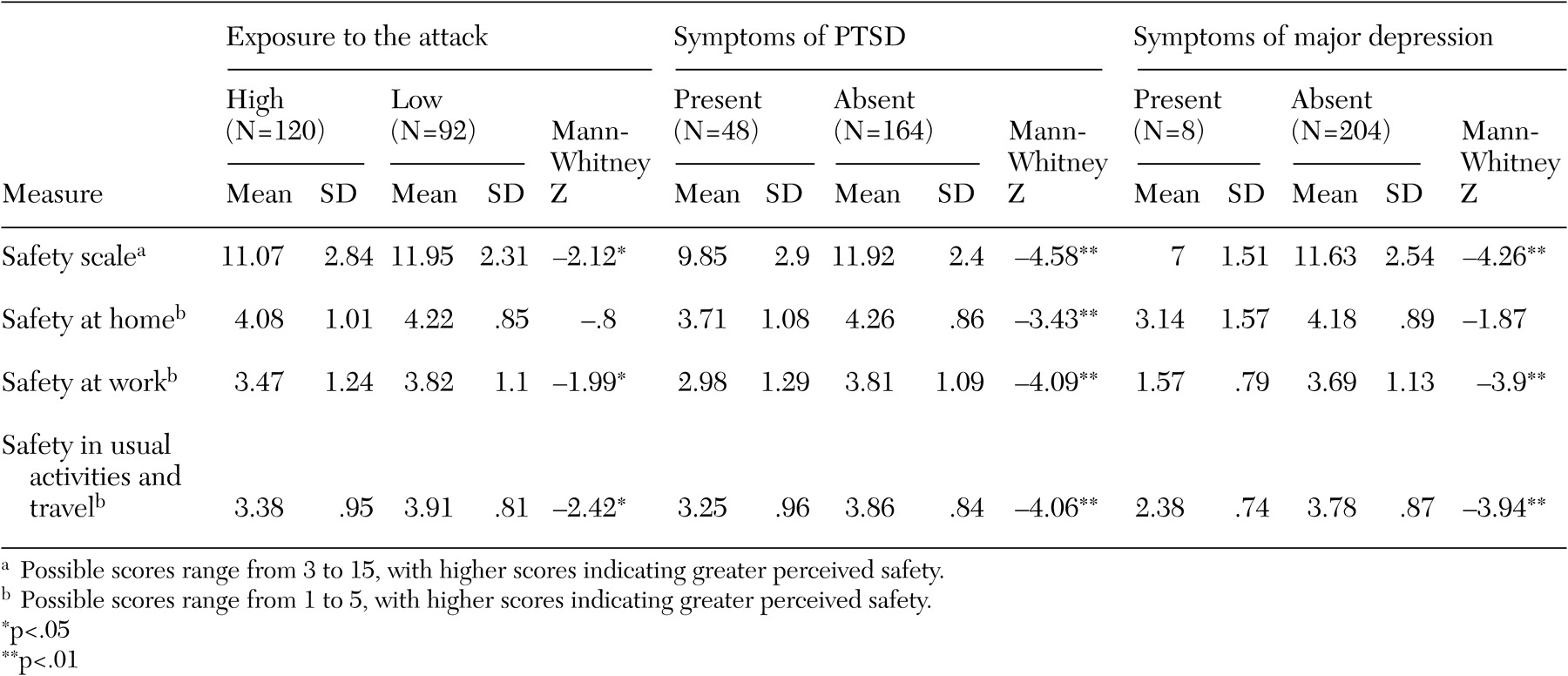
As shown in
Table 1, respondents who were in or near the Pentagon at the time of the attack were more likely than those who were at other locations to have PTSD (OR=2.50, Wald χ
2=6.47, df=1, p=.011, CI=1.23 to 5.07). All respondents with major depression were also in the high exposure group (Fisher's exact test, p=0.011). Respondents in the high-exposure group perceived lower levels of safety overall than those in the low-exposure group; however, both groups perceived similar levels of safety at home.
Respondents with PTSD were more likely than those without PTSD to have major depression (OR=27.83, Wald χ
2=9.43, df=1, p=.002, CI=3.33 to 232.56). Respondents with PTSD perceived lower levels of safety at home, at work, and in usual activities and travel (
Table 1). No gender difference was found in the rate of PTSD.
Respondents with major depression perceived lower levels of safety at work and in usual activities and travel than those without major depression (
Table 1). No gender difference was found in the rate of major depression.
Discussion
The 23 percent rate of possible PTSD that we found in one Pentagon work center 13 months after September 11, 2001, is comparable to the 14 percent rate that we found in this population seven months after the attack (
1). The 4 percent rate of major depression that we found in the study reported here is low compared with the rate found in the general population; however, the sample that we surveyed was highly educated and fully employed.
Because of the recruitment process and selection biases, the rates of illness or distress cannot be generalized to broader populations. The associations between exposure, symptoms, and subsequent perceptions of safety 13 months after the attack offer insight into the long-term burden of terrorist acts.
We found that respondents who were directly exposed to the attack were more likely to develop PTSD. However, we did not find an association between higher levels of exposure and higher rates of PTSD in our earlier study (
1). The fact that our earlier study did not show any association may have been due to the high level of exposure of the entire population sampled (70 percent) and the smaller sample. The fact that participants in the study reported here perceived lower levels of safety than participants in our earlier study indicates that the effects of the attack have persisted for more than a year.
Respondents with PTSD had high levels of comorbid depression and perceived lower levels of safety at home, at work, and in usual activities and travel. In our earlier study we found that women were 5.4 times as likely as men to have PTSD; however, we found no gender difference in the study reported here. These findings are consistent with those of other studies that showed that women were more likely than men to develop acute PTSD but not chronic PTSD (
6). In contrast to the effect of direct exposure to the attack—which affected the perception of safety at work and in usual activities and travel, but not safety at home—the presence of PTSD was associated with perceptions of lower levels of safety at home, at work, and in usual activities and travel. This finding suggests that the presence of PTSD is associated with global perceptions of environmental threat in addition to the symptoms of intrusion, arousal, and avoidance.
It is important to note that all the depressed study participants were in the high-exposure group; they may have known colleagues who were killed and experienced ongoing disruptions in the workplace.
Conclusions
Exposure to the Pentagon terrorist attack and living under chronic threat was associated with psychiatric disease, psychological distress, and altered perceptions of safety more than a year later. Further controlled study is needed to examine the effects of exposure to trauma, presence of PTSD, and presence of major depression with perception of threat, risk of engaging in activities, and assessment of safety as well as the effects of these factors on behavior and mental and physical health.