The time frame for evaluating outcomes may vary with the domain that is being considered. For example, symptoms generally remit before improvements are seen in social or work functioning (
72). During the first few months of treatment, clinicians focus primarily on reducing symptoms of disease while causing as few side effects as possible. Three to 12 months after initiating a treatment intervention, the focus will shift toward relapse prevention; treatment adherence; minimizing potential medical health risks; social, educational, and vocational reintegration; and patient and family satisfaction with treatment gains. Beyond a year the focus extends to longer-term goals, such as promoting full recovery, independent living, and physical health and optimizing the quality of life. Thus the first two outcome domains take a leading role early in treatment, and the third and fourth domains become increasingly important as treatment progresses.
Numerous tools can evaluate the effectiveness of schizophrenia treatment. In a real-world treatment setting clinicians need tools that are relatively quick and simple to administer, sensitive to change, and easily interpreted. Global ratings of clinical effectiveness may be the fastest and most practical type of tool for day-to-day clinical use. Beyond that, some clinicians may find it useful to employ instruments that examine specific outcome areas.
Global ratings of clinical effectiveness
The Global Assessment of Functioning (GAF) scale produces a single, composite score of psychological, social, and occupational functioning on a hypothetical continuum from mental health to severe illness (
15). The GAF is a widely used reliable and valid measure of psychiatric disturbance among patients with severe mental illness (
73). A modified version includes more detailed criteria and a more structured scoring system and may be particularly appropriate for use by raters with varying skills and backgrounds (
74).
Alternatively, the Clinical Global Impressions (CGI) scale can be used to assess overall clinical changes in symptoms, behavior, and function (
75). The subscales of the CGI include a measure of current severity and overall global change from a specific reference point (usually the beginning of treatment).
The GAF and CGI scales do not examine the progression of independent domains. For instance, symptoms of disease may progress differently from the ability to live independently. Therefore, a slightly expanded CGI tool that measures progress in each of the four domains by using a 7-point scale may offer a better view of how a specific patient is progressing. The panel of schizophrenia researchers proposed an expanded global assessment grid, called the Global Outcome Assessment of Life in Schizophrenia (GOALS) scale, which broadens the evaluation to consider each of the proposed four outcome domains. In using GOALS, clinicians rate each of the four domains on a scale of 1, very much improved, to 7, very much worse. (The instrument is available on request from the first author.) Clinicians can use specific rating instruments, as described below, in conjunction with clinical interviews of the patient and involved family members or caregivers to score the grid and use it in the treatment planning process.
Rating instruments for specific outcome domains
Table 2 suggests domain-specific measurement tools that may be appropriate for assessing symptoms of disease (first domain), treatment burden (second domain), disease burden (third domain), and health, quality of life, and health and wellness (fourth domain). Although some quantifiable methods can be used to assess the third outcome domain (for example, assessments of cost of treatment or resource use and caregiver burden scales), interviews with the patient and family may be more revealing. In fact, rating scales cannot supplant the importance or value of clinical interviews with the patient and information gathered from family members.
Symptoms of disease. Two scales are often used to measure severity and change in positive and negative symptoms. The Brief Psychiatric Rating Scale (BPRS) was developed to assess change in severity of psychopathology among patients with psychotic illness, such as schizophrenia and psychotic major depression (
76). The Positive and Negative Syndrome Scale (PANSS) was developed to assess psychopathology among patients with schizophrenia, with an emphasis on positive and negative symptoms but without neglecting other general psychopathology features (
77). In the recovery model of Liberman and colleagues (
9) symptom remission is defined as a score of 4 or less (moderate symptoms) for two consecutive years on each of the positive and negative symptom items on the PANSS.
No consensus exists about an appropriate office-based assessment of cognitive function. Full-scale cognitive test batteries are beyond the scope of ordinary office-based practices, and it is not clear whether abbreviated tests are satisfactory (
78). Clinicians may want to refer some patients for specialized neurocognitive assessments. Nevertheless, it is important to evaluate the impact of treatment interventions on cognitive function as well as the impact of cognition on other outcomes. The following queries might help in this assessment. To what extent have critical cognitive functions (for example, executive function and working and verbal memory) improved since the initiation of treatment? Have functional skills altered as a result of changes in cognitive capacity? To what extent has adherence to treatment benefited from better insight? To what extent have medications (for example, anticholinergics) adversely affected cognitive function?
Mood symptoms can be measured with the Calgary Depression Scale for Schizophrenia, a reliable and validated instrument developed specifically for assessing mood among patients with schizophrenia (
79,
80). Questions to assess mood symptoms might include the following: To what extent do depressive symptoms or persistent anxiety impede social, vocational, or occupational function? Are negative symptoms related to underlying depression?
Treatment burden. One clear measure of the consequences of treatment burden is adherence to drug treatment, because patients are more likely to continue taking their medication if the treatment burden is tolerable. Discontinuation of treatment also contributes to increased burden on others.
Movement disorders or extrapyramidal side effects are one of the most well recognized components of treatment burden. A number of scales are available to measure emergent or persistent extrapyramidal side effects. These include the Barnes Akathisia Rating Scale (
81), the Simpson-Angus Extrapyramidal Side Effects Scale (
82), and the Abnormal Involuntary Movement Scale (
83).
Subjective distress related to extrapyramidal side effects may be a better predictor of treatment adherence than the commonly used extrapyramidal side effects scales (
84,
85,
86). A new scale to measure side effects was recently developed by the Approaches to Schizophrenia Communication (ASC) steering group to address these shortcomings (
87). The ASC-SR is a self-report checklist to be completed by the patient, and the ASC-C is a clinician-administered version to be completed by the physician and the patient together as part of a semistructured interview (
87,
88,
89). The short list of items in these questionnaires (see box on this page) are designed to help the patient better verbalize concerns about side effects and to help the treatment team gain a better understanding of what side effects are most bothersome to the patient.
Disease burden. Schizophrenia can have a tremendous impact on the patient and his or her family. Effective treatment may help alleviate some of the negative repercussions of schizophrenia on the patient's social network. An assessment of the burden of illness requires interviews with the patient and family to assess changes since the onset of the illness. The following questions are examples of how to assess this domain: Has there been a change in the level of interpersonal or family function? Has there been a change in the cost of treatment (for families or the health care system)? Has there been a change in vocational or educational function (productivity) of family members?
Health and wellness. This broad category may require several different types of assessment. Instruments to measure health and wellness among patients with severe mental illness include the Multnomah Community Ability Scale (
90), the Quality of Life Interview (
91), the Quality of Life Scale (
92), the Wisconsin Quality of Life Index (
93), and the Schizophrenia Outcomes Module (
94). Although such detailed rating scales may not be suitable for use in day-to-day practice, clinicians should be alert for changes in the key areas assessed by these scales. Because this domain assesses successes rather than burdens, assessment questions need to include the following: Is there a change in the level of satisfaction with life, with work, with school? Is the patient more capable of independent living (self-management)? Is there a change in social relationships and intimacy with others? Is there a change in self-care (instrumental living function)? Is there a change in motivation and sense of purpose? Is there a change in health care practices—for example, smoking, substance abuse, and exercise?
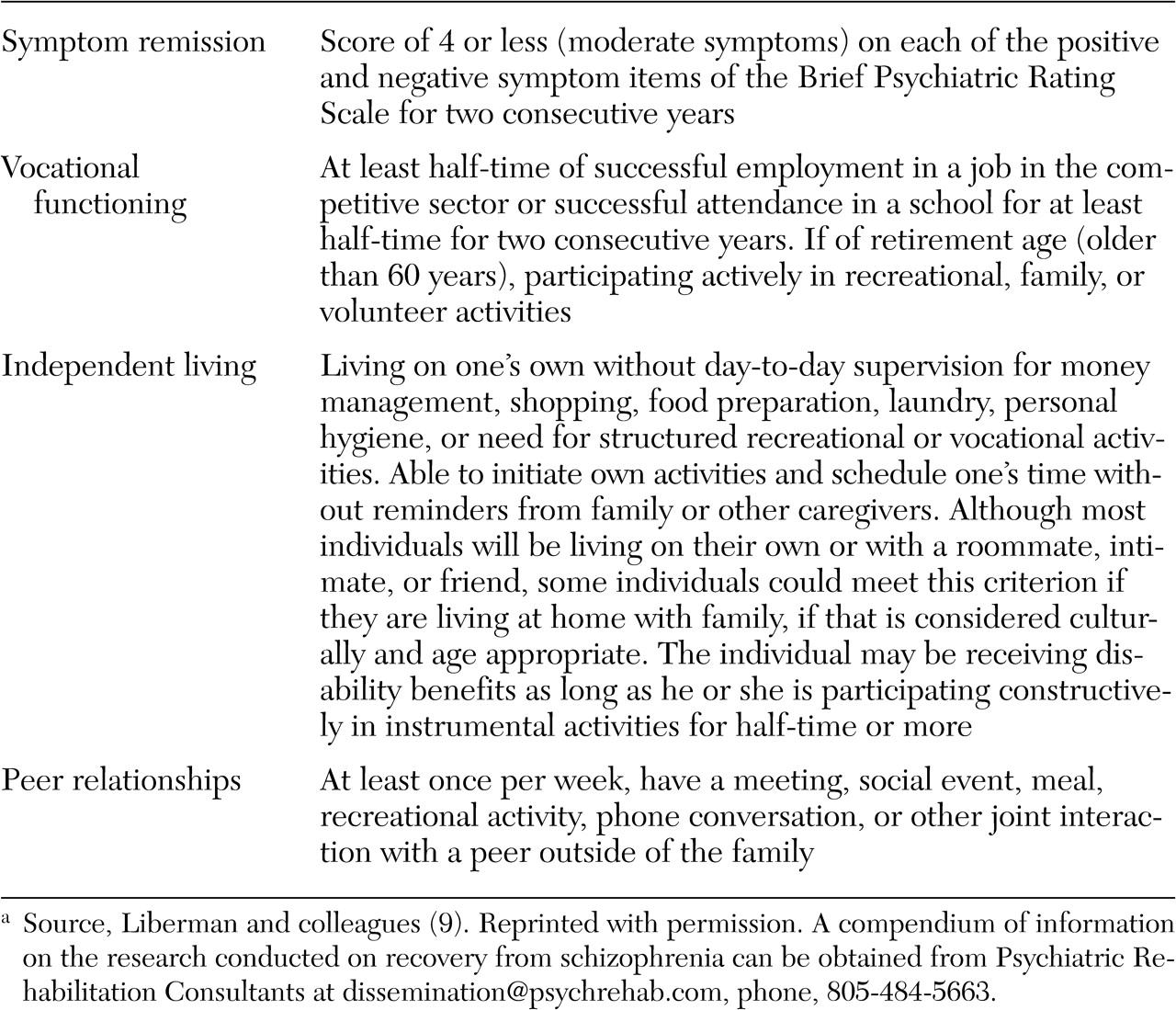
The operational definitions of recovery proposed by Liberman and colleagues (
9) may be helpful in assessing vocational functioning, independent living, and peer relationships (
Table 1). However, the overall GOALS grid score for the domain of health and wellness also anticipates consideration of the impact of treatment on quality of life.