Schizophrenia is a worldwide disorder with an incidence of about 1 percent (
1). Although there are similarities in the way schizophrenia presents globally (
2), there are significant differences in prognosis across developed cultures (
3,
4). Culturally determined processes, either social or environmental, may be partly responsible for these differences (
3). Although some differences exist among cultures, surveys show that many antipsychotic prescription practices are similar. For example, independent studies in different countries have reported the underuse of depot antipsychotics, the use of higher-than-recommended dosages of first-generation antipsychotics, the frequent use of antiparkinsonian medication in the absence of parkinsonian symptoms, and the combined use of different antipsychotics (
5,
6,
7,
8,
9).
A few studies have compared prescription patterns of second-generation antipsychotics for people with schizophrenia across different countries and cultures (
9,
10). Examining prescription patterns in different countries may assist in the development of more systematic research in international psychiatric pharmacoepidemiology (
9) and of improved practice guidelines; it may also show how different systems of care may affect outcomes (
11,
12). Furthermore, reports of clinical practice and real-world use of antipsychotics are important because they can define and guide research questions (
13).
Clozapine is the only second-generation antipsychotic that has been shown to have consistent superiority over first-generation antipsychotics for the treatment of chronic schizophrenia and for patients who are treatment intolerant. According to current treatment recommendations and guidelines, clozapine should be used after two failed optimized trials of antipsychotics (
14,
15,
16). Nonetheless, clozapine likely has been underused in the United States, probably because it has a higher side effect burden than other second-generation antipsychotics (
17,
18,
19,
20). In fact, in the United States the use of clozapine has been decreasing since the introduction of other second-generation antipsychotics. For example, clozapine accounted for 11 percent of prescriptions for second-generation antipsychotics in 1999; this rate decreased to approximately 9 percent in 2000 and to less than 5 percent in early 2002 (
21,
22,
23). In the United States we would expect to observe the highest rate of clozapine use in inpatient treatment facilities because of the severity and chronicity of illness among patients in these facilities. To assess use and treatment differences across different cultures and different systems of care, we wanted to compare clozapine use for the treatment of schizophrenia in inpatient settings in the United States and in similar settings in another country. In Australia inpatient mental health facilities have closed and people with treatment-resistant schizophrenia are managed exclusively as outpatients. Thus this study compared inpatients from Maryland, United States, with outpatients from Victoria, Australia.
Methods
This cross-sectional study examined clozapine prescriptions in January 2000. In Maryland data were gathered from patient records at all six inpatient state mental health facilities in the state from a central state database for antipsychotic use. Patients from these facilities were included in our study if they had been given a prescription for clozapine, risperidone, olanzapine, or quetiapine during this period. In Australia data from a medical records database were collected for all patients in two large community outpatient clinics in Victoria who were given a prescription for antipsychotics during this period. All diagnoses were assessed according to DSM-IV criteria.
The use of antipsychotics by racial or ethnic groups is not reported here because of the small samples in each racial or ethnic category. However, we did not find significant differences between whites and persons from minority groups (African American, Hispanic, and Asian) in the overall sample. Aboriginal, Maori, and Pacific Islanders were not represented in this sample.
Most of the data were descriptive. Chi square and Fisher's exact tests were used to compare the categorical demographic and clinical variables between the systems. Continuous variables were compared with Student's t test. Statistical significance was set at p<.05.
The study was approved by the respective institutional review boards, and a waiver of informed consent was granted in Maryland because of the nature of the data gathered.
Results
Data were available for 761 inpatients in Maryland and 467 outpatients in Victoria who received second-generation antipsychotics in January 2000. Data on the use of first-generation antipsychotics are not presented here. However, our study found that in Victoria 740 of 1,207 of the prescriptions for antipsychotics (61 percent) were for first-generation antipsychotics. In accordance with national statistics, it is estimated that the rate in Maryland was approximately 30 percent (
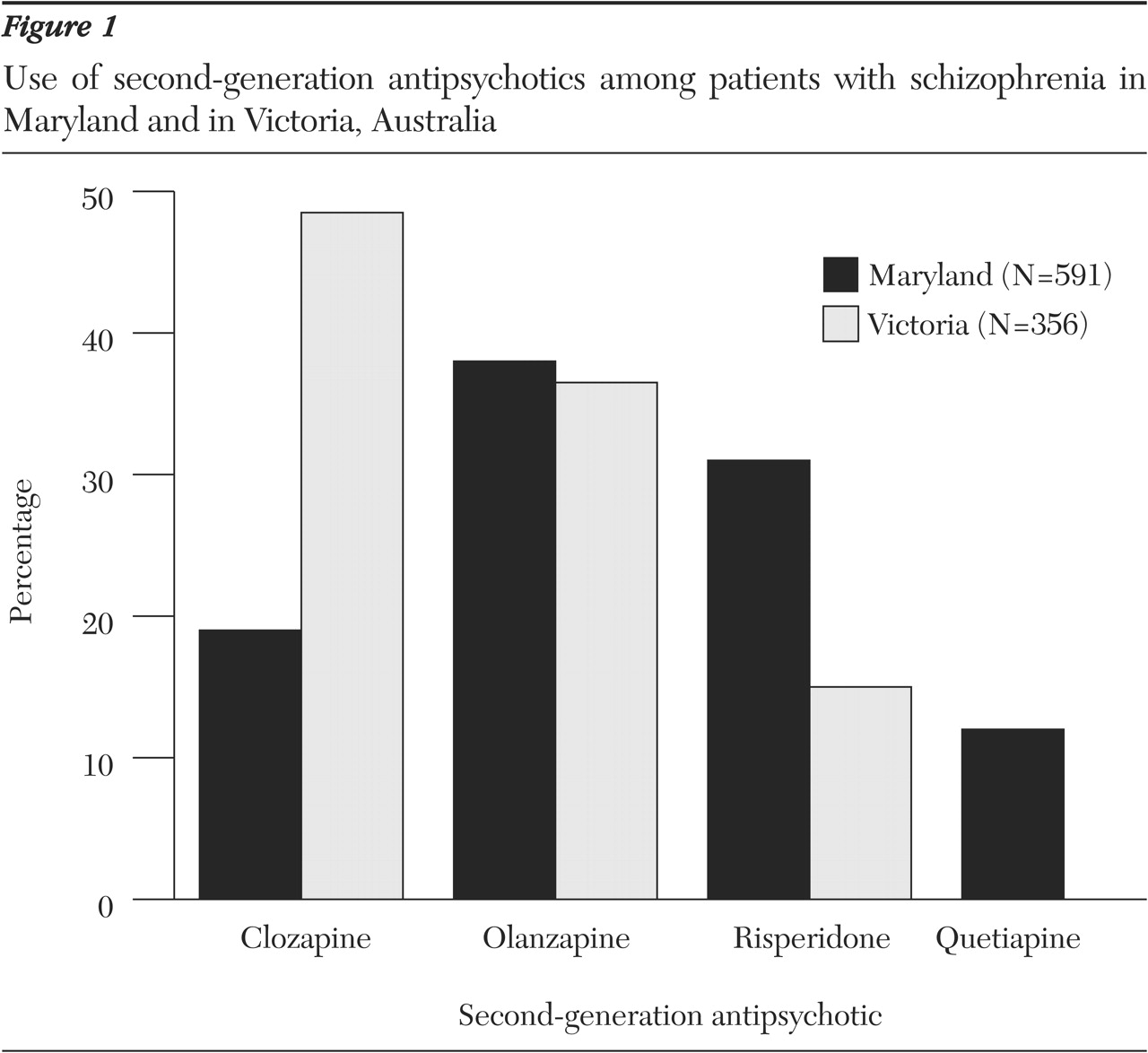
21). In Victoria the most frequently prescribed second-generation antipsychotics were olanzapine (193 prescriptions, or 41 percent) and clozapine (184 prescriptions, or 39 percent); 90 of the prescriptions (19 percent) were for risperidone. In Maryland the most frequently prescribed second-generation antipsychotics were olanzapine (288 prescriptions, or 38 percent) and risperidone (248 prescriptions, or 33 percent); 130 of the prescriptions (17 percent) were for clozapine. Although quetiapine was marketed in both countries, our study found that it was used only in Maryland (95 prescriptions, or 12 percent).
Figure 1 shows the use of second-generation antipsychotics for the treatment of schizophrenia. In Victoria 356 of the prescriptions for second-generation antipsychotics (76 percent) were for the treatment of schizophrenia; in Maryland 591 prescriptions (78 percent). Clozapine use in both Victoria and Maryland was almost exclusively for the treatment of schizophrenia (94 percent in Victoria compared with 88 percent in Maryland). Among the second-generation antipsychotics used for the treatment of schizophrenia, clozapine was the preferred agent in Victoria (173 of the prescriptions, or 49 percent); clozapine was not used as frequently in Maryland (114 prescriptions, or 19 percent; χ
2=90.3, df=1, p<.001).
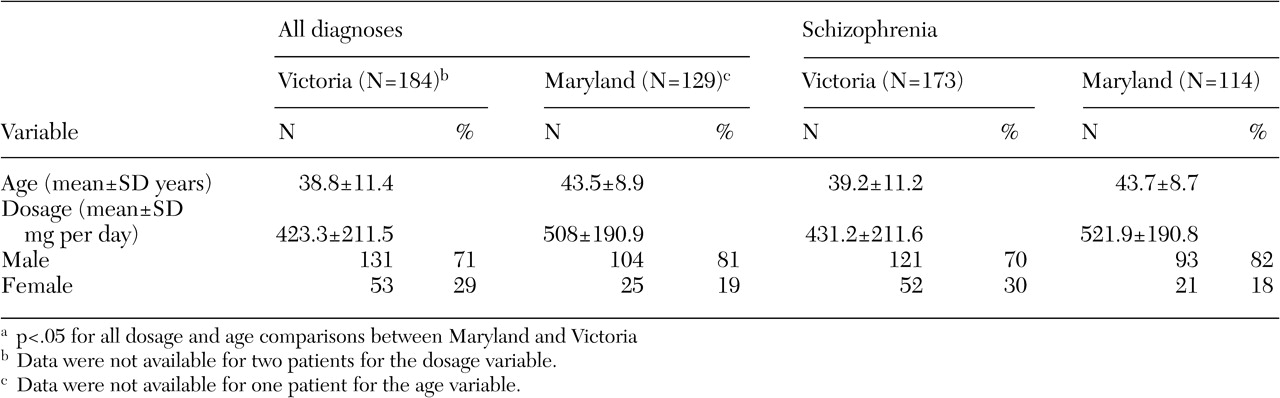
Table 1 lists the mean age of patients treated with clozapine and the dosages of clozapine that were prescribed for them. The mean age in both systems was between 39 and 44 years. Patients who were treated in Victoria were slightly younger than those in Maryland (t=-3.76, df=273, p<.001). In Maryland significantly more patients with schizophrenia who were treated with clozapine were male (χ
2=30, df=1, p<.001). Also, mean clozapine dosages for patients with schizophrenia were higher in Maryland than in Victoria (t=-3.85, df=284, p<.001).
Discussion
The results of this study show that among the second-generation antipsychotics used to treat schizophrenia in 2000, clozapine was used more frequently in Victoria than in Maryland. This finding is especially interesting given that, compared with outpatients in Victoria, inpatients in Maryland, in light of the fact that they are inpatients, might be more ill, easier to start on clozapine treatment, and easier to monitor. Furthermore, clozapine was used almost exclusively for the treatment of schizophrenia in both countries, which demonstrates that the lower dosages in Victoria and lower usage in Maryland are not driven by diagnostic differences.
It is possible that inpatients were given higher dosages, because higher dosages tend to be used in these settings. Also, the comparability of the samples may have been affected by the use of different treatment settings, which is a limitation of the study. However, regardless of the severity of illness of the outpatients in Victoria, the lower rate of prescription of clozapine in the United States is of concern. Inpatients with treatment-refractory illness may be the group that is the most in need of clozapine therapy and may benefit the most from its use. It is likely that increased use of clozapine may allow some patients who would otherwise be hospitalized to have modest gains in quality of life and be managed in community settings (
24,
25,
26). Rehospitalization rates are known to be lower with clozapine than with other second-generation antipsychotics; thus the potential exists for lowering overall costs with greater use of clozapine (
27,
28,
29).
In our study it was not evident why clozapine use was higher in Victoria than in Maryland. Rates of agranulocytosis appear to be similar in both countries (
30). However, in Australia, once patients complete the first 18 weeks of clozapine therapy, monthly monitoring of blood cell counts is all that is required, whereas in the United States twice-monthly monitoring is required (
31). Furthermore, reports from Australia note that using clozapine in the community setting leads to large cost savings, significantly reduced hospital and hostel bed use, and continued improvements in symptoms for up to five years (
32).
The dosages of clozapine used in Maryland were higher than those used in Victoria. This echoes a 1994 study by Fleischacker and colleagues (
33) that demonstrated that the mean dosage of clozapine used in Europe was significantly lower than that used in the United States (284 mg per day compared with 444 mg per day). Our study also found that in Maryland clozapine was prescribed more frequently to men than to women compared with in Victoria. This finding may reflect differences between an inpatient and an outpatient population. In the United States more men than women are hospitalized, even though the incidence of schizophrenia is similar across genders (
34) and medication dosages may be higher among men. However, the data from our study, based on widespread clozapine use and lower dosages, suggest that the lower antipsychotic dosages in the United States require more consideration.
Limitations of this study include the lack of data on concomitant medications and information on symptom severity. Strengths include the sample size and the inclusiveness of data within the system of care. Specifically, the Maryland data included all the public facilities within the state. The Victoria data included the two main community mental health centers in the state. Furthermore, this study adds to the limited body of data that compares clozapine use and dosages between different cultures or care systems.
Conclusions
Significant differences in use and dosages of clozapine were found in two populations (inpatients in Maryland and outpatients in Victoria) that were similar in diagnoses and demographic characteristics. More research is needed to discern prescribing behavior and how it may differ among cultures—for example, how pharmaceutical company detailing, and costs influence prescribing. More important, discerning how differences in prescribing patterns may affect outcomes is needed to assist in advancing evidence-based practice. Current evidence-based approaches have generally been overly reliant on clinical trials; recommendations more applicable to real-world populations are needed (
12,
35,
36). Actual data on prescription patterns can play a valuable role in helping to determine drug selection and dosages, rather using extrapolations from clinical trials to make this determination (
37).
Acknowledgments
The authors thank Yang Yu, M.A., Shelda Alcock, B.Sc., and Nerelie Freeman, B.Sc., for data analysis and maintenance. They also thank Robert P. McMahon, Ph.D., for statistical review. This work was supported in part by the grant P-50-MH-4027-9 from the Advanced Center for Intervention and Services Research and by the Stanley Medical Research Institute. Initial data collection and database infrastructure for the Australian data was supported by Eli Lilly and Company, Janssen-Cilag, and Novartis.