Results
Within the total treated sample (N = 89), there were 57 patients in the Major Unlocking Group with an average age of 38.8 years, 48% being male, who received on average 16 sessions. In comparison, there were 33 patients in the No Major Unlocking Group: 58% were male, the mean age was 40.9 years, and treatment length was on average 13 sessions. In total, 63 patients completed the DAPP-BQ (Livesley, 2009). Both groups reported moderate to large personality disorder burden (M = 86.3, Major Unlocking N = 43; M = 89.2, No Major Unlocking N = 20). Statistical analysis revealed no significant Group differences (p > 0.05) on age, gender, DAPP-BQ scores, or treatment length. All patients who completed pre-treatment self-report data were included in the analyses of outcome data. Statistical analyses were computed with Statistical Package Social Science version 19; all analyses were two-tailed and the threshold for significance was .05 unless otherwise specified.
Baseline Data
Random assignment of patients to
Major Unlocking versus
No Major Unlocking response was not possible with this design. Therefore, we carefully explored potential baseline differences in Pre-Scores across the two levels of the
Unlocking Group factor and also across the dichotomous
Resistance factor. Analyses of variance (ANOVAs) revealed no significant differences across levels of these two factors (
Table 1).
Outcome Data
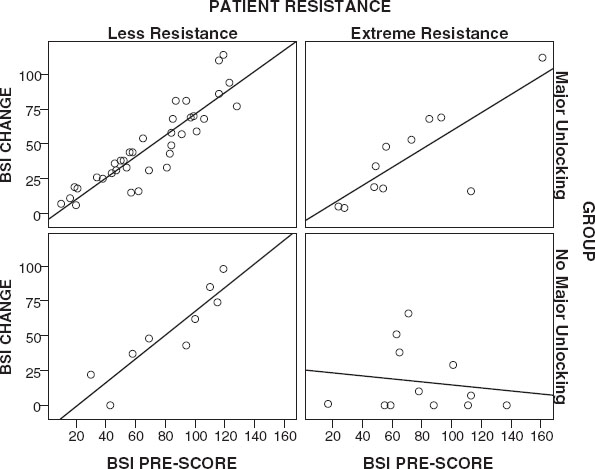
Change Scores (Pre-Scores minus Post-Scores) were used to evaluate the impact of Major Unlocking in self-reported treatment outcomes. Change Scores detect the magnitude of differences between Pre-Scores and Post-Scores but they are not sensitive to potential Group differences in outcomes caused by baseline differences in symptom severity or patients’ capacity (Resistance). Therefore, Resistance (2 levels) and Pre-Scores (continuous data) were considered as covariate factors of Change Scores, using an ANCOVA model with one Group factor (Major Unlocking versus No Major Unlocking). Given the slightly different sample sizes across the four self-report measures, one ANCOVA was computed for each of the outcome measures BSI-53, BAI, BDI and IIP-64, and the threshold for significance was adjusted to .0125 (.05/4).
For each outcome measure, the ANCOVAs revealed a significant effect of the Major Unlocking Group while holding constant baseline symptom severity and Resistance level: the magnitude of Change Scores was greater in patients with a Major Unlocking response. The strength of the relationship between Unlocking Group and magnitude of Change Scores, as assessed with partial rf revealed that the Group factor accounted for about 10% of the variance in Change Scores for the BSI-53 and the BDI, 13% for the BAI, and 20% for the IIP-64. A very strong effect size was observed for the covariate Pre-Scores entered in the statistical model (accounting for 40% to 59% of the variance in Change Scores); the covariate Resistance had a smaller effect size (accounting for 9% to 18% of the variance in Change Scores).
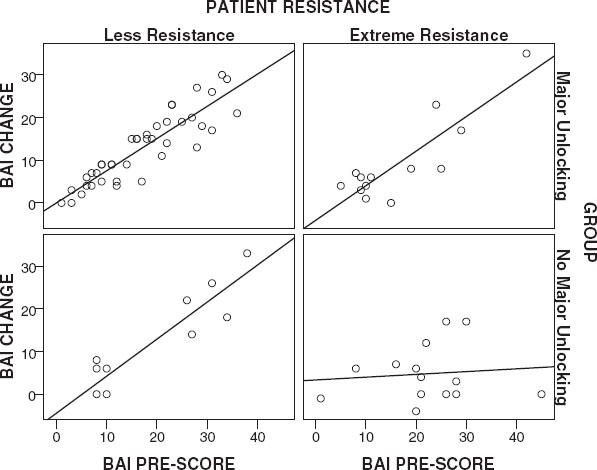
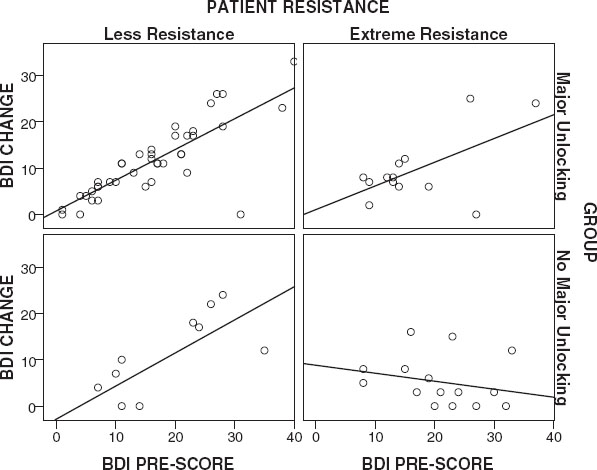
Figures 1-
4 present a visual representation of the association between Pre-Scores and Change Scores when the interaction between Group and
Resistance is considered. Inspection of the slope lines reveals a positive linear relationship between Change Scores and Pre-Scores on the BDI, BAI and BSI-53 across Groups and
Resistance, except for patients with extreme
Resistance in the
No Major Unlocking Group.
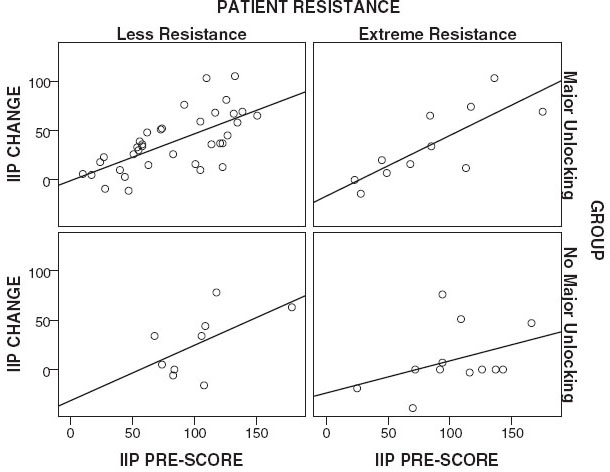
Figure 4 illustrates the result of the ANCOVA that
Resistance does not appear to be a covariate of this relationship on the IIP-32.
Relationship between Unlocking the Unconscious & Functional Improvements
To evaluate the impact of
Unlocking Group on patients’ functional improvement, two-way contingency table analyses were conducted on two indicators of patient functioning. The outcome variables of interest were patients’ return to work status and proportion of patients discontinuing all psychotropic medications. Chi square (χ
2) analyses revealed a significant effect of Group on the frequency of patients returning to work during treatment (χ
2 (1, N = 41) = 11.33,
p = 0.001, Cramer’s V = .52). Comparison of the expected and observed values within the Chi-squared cells revealed that a greater number of patients in the
Major Unlocking Group returned to work (84.6%, N = 22) and the reverse was true of patients in the
No Major Unlocking Group (15.4%, N = 4). Using Chi-squared analysis, a significant effect of Group was also found on the frequency of patients discontinuing all medications versus remaining on medication post-treatment (χ
2 (1, N = 26) = 13.48,
p = 0.000, Cramer’s V = .720). Of the fourteen patients who were on medication pre-treatment and subsequently had a
Major Unlocking within therapy, 100% discontinued medication during treatment, while 33.3% (N = 4) in the
No Major Unlocking Group discontinued medication during treatment. According to
Cohen’s (1988) criteria, both findings reported here are considered large effects (φ
>0.5 = large); however, using more conservative criteria (φ
>0.5 = moderate), these effects would be considered moderate in size (
Ferguson, 2009).
Relationship Between Healthcare costs and Unlocking the Unconscious
Mean pre-treatment healthcare costs and post-treatment cost reductions were compared between patients with
Major Unlockings (N = 57) and patients with
No Major Unlockings (N= 32), using appropriate
t tests (
Table 3). During the year prior to ISTDP treatment, there were no Group differences in baseline physician billings, hospital costs and combined total costs. Post-treatment data showed that for physician costs, the
Major Unlocking Group had a significant $273 CDN (49.2%) drop (p = .022) while patients with
No Major Unlocking had a non-significant $51 CDN (8.1%) reduction in costs. Post-treatment, a statistically significant between Group difference was found (p = .006) revealing larger cost savings in the Major Unlocking Group. In terms of hospital costs, both groups had large post-treatment reductions, each group reaching to below costs for matched population of controls ($265 CDN). However, neither of these reductions were statistically significant; likewise, there were no Group differences in post-treatment hospital costs. Finally, the post-treatment combined costs were significantly different between the two groups of patients (p = .005), whereby the
Major Unlocking Group reached to below a matched whole population norm ($407/year) while patients with
No Major Unlocking did not.
Discussion
The current study presents a preliminary attempt to operationalize the therapeutic event of accessing dynamic unconscious emotions according to a specific line of dynamic theory (
Davanloo, 1990,
2000) with a view to examining treatment effectiveness when this takes place. Naturalistic outcome data is presented, collected before and after a course of ISTDP. Patients were categorized in two groups according to whether or not they had
Major Unlocking of the Unconscious during treatment sessions. We were struck to find significant superior treatment effects in the
Major Unlocking patient Group on measures of psychiatric symptoms, interpersonal functioning, functional measures, and service utilization post-treatment. This evidence of significant diffuse outcome contributions endorses a key therapeutic role of
unlocking the unconscious and may highlight indications for understanding the complexities of change in psychotherapy.
We characterized Major Unlocking of the Unconscious as a discrete, observable, in-session event, defined by a specific therapist-patient interaction preceding a major patient communication revealing in depth, affect laden material about past attachment trauma. One can question whether or not these events exist along a continuum. Patients in the No Major Unlocking Group experienced a degree of mobilization of the unconscious but not a major access. The finding of wide-ranging and significantly larger treatment effects in those with a Major Unlocking is even more suggestive of the importance of degree of emotional processing. It could also suggest that Major Unlocking is a threshold event markedly superior to lesser degrees of mobilization. The fact that an experienced ISTDP clinician identified fifty-seven treatments from a case-series of eighty-nine treated patient in which a Major Unlocking occurred indicates that this event was common in a relatively brief treatment course of this treatment.
Previous research has highlighted the relationship between higher levels of patient affective arousal and preceding active therapist confrontation to impulse/feeling and patient defense (
Town, Hardy, McCullough & Stride, 2012) and an association between patient affect responses and outcome (
Taurke, Flegenheimer, McCullough, Winston, Pollack & Trujillo, 1990) in STDP. The nature of the specific therapist interventions, invariably involving systematic challenge to the
Resistance, preceding the breakthrough should therefore also be considered of likely significance in contributing to this finding. Theoretically, this result may point to the importance of three theoretical dynamic principles: (1) Access to painful hidden memories is proportional to degree of mobilization of the
unconscious therapeutic alliance; (2) the relevance of exploring feelings in current relationships or towards the therapist is their route to the patient’s past; (3) de-repression, experiencing, and gaining insight about painful emotions weakens unconscious associations and connections preventing repetitive, habitual and maladaptive operations, thus making way for major therapeutic benefit.
Given the significant affective component within a
Major Unlocking, the ‘common factors’ (
Wampold, 2001) literature points to the possible overlap this construct may have with common descriptions and measures of patient heightened emotional experiencing (
Klein, Mathieu-Coughlan, Gendlin, & Kiesler, 1969;
Klein, Mathieu-Coughlan, & Kiesler, 1986), and arousal (
McCullough, Larsen, Schanche, Andrews, Kuhn & Hurley, 2003;
Warwar & Greenberg, 1999). As such, the current finding may be consistent with interpretations of research evidence suggesting the utility of facilitating emotional processing (
Diener & Hilsenroth, 2009;
Salvadori, 2010;
Whelton, 2004) and evidence that it correlates with improvement (
Diener, Hilsenroth & Weinberger, 2007). Second, we note that whilst achieving a spontaneous genetic link to a patient’s past is a central issue within ISTDP and other dynamic schools, this also may represent a sophisticated description of patient insight. Limited research, generally using broad definitions of insight, suggests that amount of gain in patient insight over treatment is likely associated with improvement (
Connolly Gibbons, Crits-Christoph, Barber & Schamberger, 2007). The current findings are more consistent with the principle that the concept of insight, with its inherent complexities, is best understood through measurement of specific insights about core-conflictual relationships or salient issues.
A secondary research finding revealed that patients with extreme
Resistance seemed to require
Major Unlocking of the Unconscious to benefit. This matches the basic principle of ISTDP: that
Resistant patients need greater mobilization of the
unconscious therapeutic alliance to promote change. Previous research using standardized measures of patient defense in dynamic therapies has also shown that initial defense ratings predict outcome (
Høgland & Perry, 1998) and dynamic therapists intuitively respond to patient defences with more psychodynamic-interpersonal interventions (
Siefert, Hilsenroth, Blagys & Ackerman, 2006) leading to improved outcome (
Hersoug, Bogwald & Høgland, 2003). Whilst empirical findings support the dynamic principle that resistance opposes psychotherapeutic efforts, interfering with patients’ ability to make use of insights and tolerate affects (
Dozier & Kobak, 1992), the
Unlocking process may represent an important tool in the clinician’s kit to facilitate change and avoid protracted or interminable treatments with such patients.
Patients categorised as extreme
Resistance in this sample presented with diffuse symptoms, lifelong character pathology, many of whom exhibited immature defences based on clinical observation (
Davanloo, 1995a;
Vaillant, 1992). We suspect that it is this population, categorized as having low Quality of Object Relations (
Piper, Joyce, McCallum & Azim, 1993), that previous STDP research (
Piper, Azim, McCallum & Joyce, 1990;
Piper, Joyce, McCallum & Azim, 1998) indicated that the priority in treatment may not be examining problematic past relationships (
Joyce & McCallum, 2004). The current study points towards the importance of
unlocking the unconscious with these complex groups of patients and indicates a greater range of patients than first thought have the underlying capacity to tolerate intense therapeutic emotional experiences. These results complement recent empirical evidence suggesting transference focused dynamic interventions (
Høgland, Amlo, Marble, Bogwald, Sorbye, Sjaastad et al., 2006;
Høgland, Johansson, Marble, Bogwald, & Amlo, 2007;
Høgland, Bogwald, Amlo, Marble, Ulberg, Cosgrove et al., 2008) and treatment models (
Abbass, Sheldon, Gyra & Kalpin, 2008;
Clarkin, Yeomans & Kernberg, 1999) can be helpful for those with poor objective relations and personality disorder (
Town, Abbass & Hardy, 2011).
There are several limitations to this study that limit interpretation of the findings. First, the reliability of ratings identifying the presence of a Major Unlocking and designation of levels of Resistance are unclear. Although measurement reliability would have been enhanced by ongoing therapist videotaped supervision and reference to the original manualized description of these variables, the use of therapist ratings rather than those of an independent observer could have led to experimenter bias. This is made less likely by the fact that ratings were done a priori without knowledge of this retrospective analysis, but it cannot be ruled out. Second, the study design relied upon patient self-report for measurement of symptom and interpersonal change and patients were not randomly assigned to group. The healthcare use data was, however, provided blinded, in grouped fashion by the government of British Columbia and based on an a priori categorization by the therapist. Third, to establish a causal process-outcome relationship, further study is required using randomized allocation and a dismantling method specifying rise in mobilization of unconscious processes between treatment group. It would however be difficult to experimentally manipulate the variable of unlocking of the unconscious without inadvertently confounding the effects of other common and specific treatment factors. Nevertheless, it remains a possibility that the different treatment effects seen between Groups were not in fact associated to the presence of heightened emotional processing of unconscious material, rather some other construct not measured or existing patient differences between Groups. To adjust for the later possibility, intention to treat analyses were performed and pre-treatment self-report scores and levels of Resistance controlled for. Furthermore, neither the mean pretreatment scores on the BSI, IIP, BAI, BDI, DAPP-BQ nor cost measures 1-year pre-therapy differed significantly between the groups: thus, patient Groups appear more similar than different.
Based on the above, future research into
Major Unlocking is warranted. Future research should clarify if the theoretical distinction between a
Major Unlocking, complete with visceral experiencing of guilt laden rage, grief and the insight gained with a genetic image transfer, is empirically justified and if so, to what extent such differences between in-session treatment events contribute to the relative size of treatment effects. Improvements in future research methodologies can include multiple assessments of in-session process and post-session outcome to examine the temporal relation between the presumed putative change variables and proposed outcome. Second, blinded standardized ratings of
Unlocking events and patient
Resistance should be established. Such a rating guide is in development now to be piloted (Town & Abbass). Although preliminary data in developing an adherence guide for ISTDP supports that the events can be reliably coded from videotaped sessions (
Abbass et al., 2008).