Clinical context
Since their respective beginnings, psychiatry and pain medicine have been closely linked. For instance Sigmund Freud was the first physician to publish on the local anesthetic properties of cocaine, whereas anesthesiologist Henry K. Beecher provided early evidence to support the placebo effect, one of the most profound psychological constructs in medicine. Both fields have embraced the biopsychosocial approach to medical education and care, pioneered by George Engel (
1).
Chronic pain disorders and psychiatric disorders share a commonality from both descriptive phenomenology and underlying biology. Chronic pain is not merely acute pain that lasts for some predetermined time, just as major depression and generalized anxiety do not represent protracted sadness or fear. Chronic pain is described in terms of being excessive, relentless, and unbearable. It is often shown on the face and in the body habitus of its sufferer. Too often it disrupts psychological and physical functioning, potentially leading to self-destructive thoughts and even suicide. Such descriptors sound familiar to psychiatrists because one could easily substitute the words “depression” or “anxiety” for “chronic pain.” Whereas many patients with chronic pain exhibit mood and anxiety disturbances, the converse is also true (
2). Biologically, pain, mood, and anxiety disorders overlap in the limbic, hypothalamic, prefrontal cortex, locus ceruleus, and spinal centers (
3). Loss of neurochemical homeostasis is a hallmark of these disorders that results in or is the result of maladaptive neuroplasticity (
4,
5). It remains unclear whether the observation of chronic pain and chronic affective disorders frequently occurring simultaneously reflects comorbidity of distinct disease states or expression of the same underlying biological disease. Most likely this phenomenon is the result of both.
There is a high incidence of chronic pain in the general population. Estimates suggest that about one in every four to six persons has chronic pain (
6–
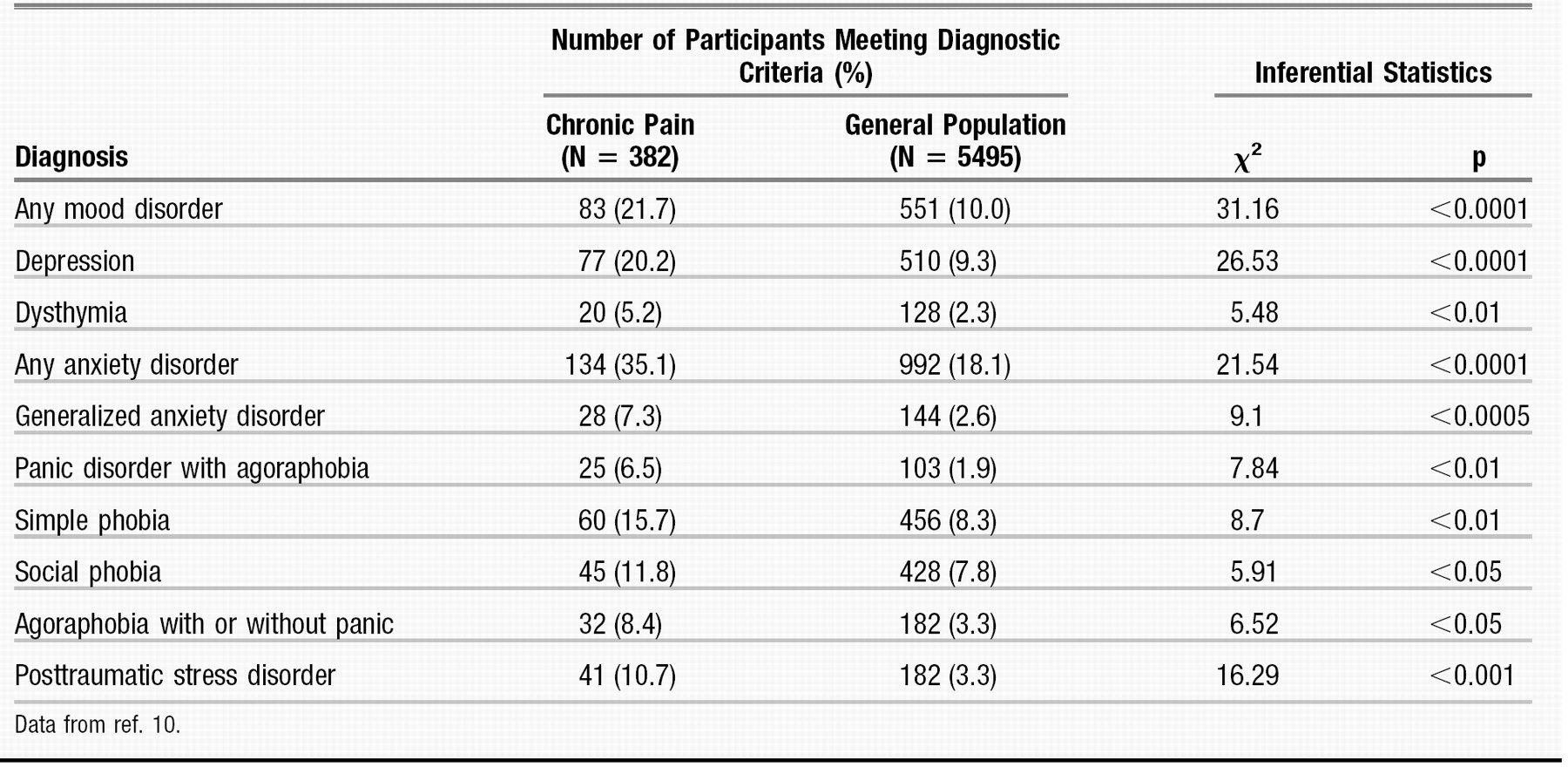
9). There is increasing evidence that psychological disorders such as depression or anxiety often coexist and may be correlated with chronic pain (Table 1). One study found that patients in chronic pain meet the criteria for an anxiety disorder at almost twice the rate of the general population (35% versus 18%) (
10). The number of patients with chronic pain and comorbid depression is even more impressive. Almost two thirds of patients with persistent pain have a lifetime history of major depression. In untreated and treatment-resistant depression the number of patients who exhibit chronic pain is between 30% and 50% (
11–
13).
Pain is a complex physical and emotional experience that is unpleasant and may represent actual or potential tissue damage (
14). Price (
15) pointed out that acute pain engenders the emotional responses of fear and anger, whereas chronic pain is more likely to elicit despair and hopelessness. In acute pain the brain and spinal cord collaborate to perceive the sensation, react to minimize the potential damage, and dampen the actual experience. With chronic pain, these built-in mechanisms fail through a process of excessive neuronal activation in the spinal cord and brain, in part due to a phenomenon known as wind-up. This results in an amplified perception of pain relative to evoked peripheral stimuli and impaired down-regulation of pain via normal descending modulatory mechanisms in the CNS. The concurrent emotional response is also out of proportion, and the pain and emotional systems form an unfortunate positive feedback loop that escalates and perpetuates the pain disorder.
The neuroanatomy involved in chronic pain demonstrates substantial overlap in systems subserving pain and emotion. Pain processing in the brain occurs via the spinothalamic tracts and occurs in multiple deep brain and cerebral areas. Thalamic relays to hypothalamic and limbic systems pass further upstream to the prefrontal cortex, anterior cingulate cortex, posterior cingulate cortex, insula, posterior parietal complex, somatosensory cortex, and supplementary motor cortex. This results in a broad response to pain including emotional, neuroendocrine, arousal, autonomic, and somatosensory responses (
16).
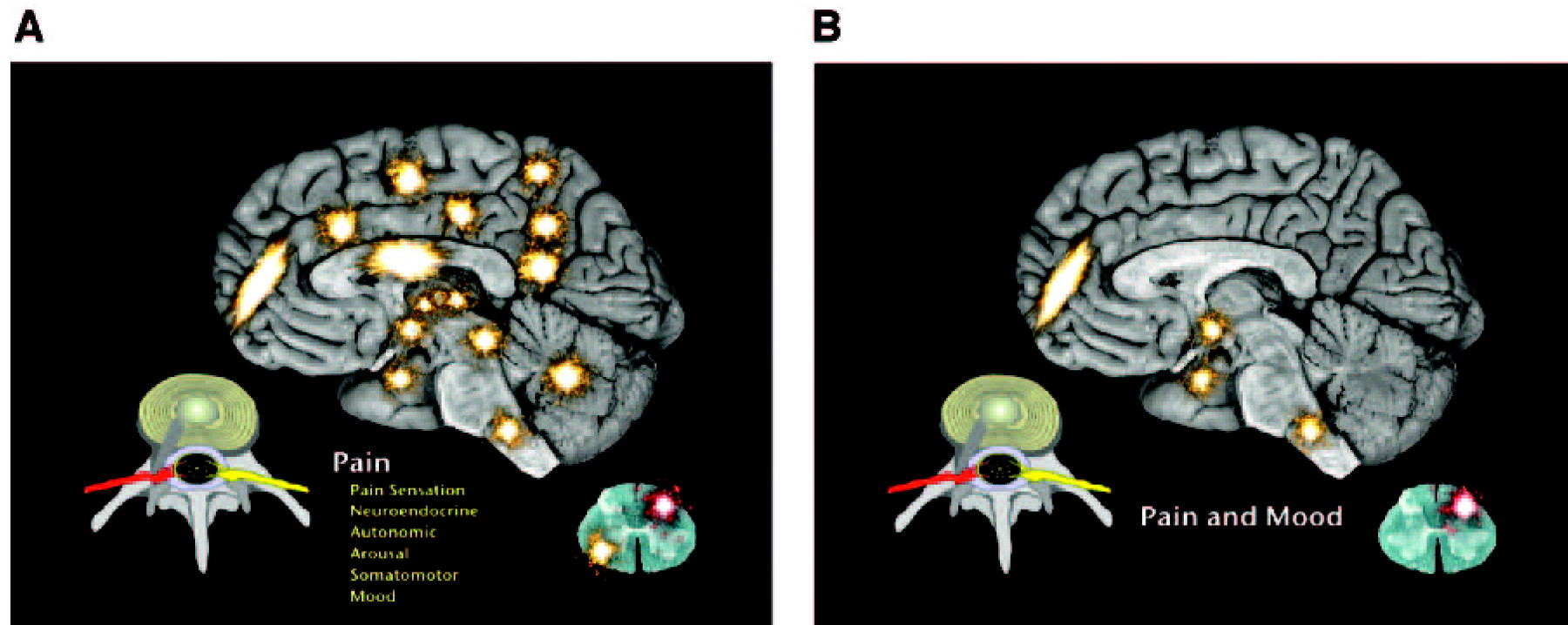
Psychiatrists have long known that the limbic system is only a part of the overall emotional response system. The emotional response to pain involves the ascending reticular activating system, which sends fibers to the frontal cortex, limbic system, hypothalamus, cerebellum, and dorsal horn of the spinal cord (
17). Anatomically the pain-processing areas of the brain include the same areas seen in mood and anxiety disorders (
18) (Figures 1, A and B).
What is the difference between acute and chronic pain? There is no one answer to this important question. However, answers may be found through comparing the differential physiological and cellular molecular biological characteristics of acute versus chronic pain.
In acute pain, a signal generated at peripheral nociceptors (specialized nerve receptor endings embedded throughout peripheral tissues) is sent to the CNS via nerves that end at the spinal cord. Synaptic processes pass the signal to second-order neurons in the dorsal horn of the spinal cord, which pass the signal to third-order neurons in the dorsal horn. These cross to the contralateral side of the spinal cord and travel via nerve tracts to the brain, where the signal diffuses to multiple areas evoking a varied response. The brain sends a counter signal to the dorsal horn and suppresses the incoming pain signal (
19).
In chronic pain, these processes break down peripherally and centrally, resulting in problems ranging from increased peripheral activation, release of increased neurotransmitters, activation of normally inactive receptors leading to amplified signaling (termed wind-up), and abnormal neuroplastic reorganization. The CNS becomes sensitized as amplified signals are sent to the same brain centers as in the acute state, but subsequent regulation from the brain is frustrated by maladaptive sensory processes, such as those that wind up at the dorsal horn. The end result is an experience of pain unpleasantness that is more robust and enduring than the peripheral stimulus, which sustains itself independently of ongoing peripheral input. Unlike the normal process in which pain is a symptom of a normally activated alarm that registers harm, potential harm, or ongoing healing in the body, this pain is evidence of an injured alarm system. Therefore, chronic pain is usually not just a symptom but is the manifestation of a chronic disease process resulting from runaway neuroplasticity (
20).
The neuroplasticity and loss of neural regulatory control seen in pain, mood, and anxiety have striking overlap. γ-Aminobutyric acid (GABA) is the major inhibitory neurotransmitter that regulates sleep, pain, anxiety, and seizures. Chronic pain results in loss of GABAergic control, leading to disproportionate excitation of the CNS mediated by unleashed glutamate (
21). Substance P is excessively released at presynaptic terminals due to inflammation, pain, emesis, depression, and anxiety (
22). Activation of
N-methyl-
d-aspartic acid (NMDA) receptors is currently considered to be a central event in the neuroplasticity of pain (
23) and affective disorders (
24). In either case, normally dormant postsynaptic NMDA receptor complexes become activated by excessive peripheral stimuli (release of high levels of Substance P and glutamate in pain and high circulating serum cortisol levels in affective disorders). As glutamate attaches to internal sites, excessive calcium flows through the activated NMDA receptor complexes into the postsynaptic nerve cell, leading to threshold changes at the cell membrane and chemical alteration within the cell (
25). Malfunction of serotonin and norepinephrine centers in the brainstem may result in depression and anxiety in patients with pain (
26) and pain in depressed and anxious patients (
2). All of these changes result in decreased brain-derived neurotrophic factor, which, in the face of excitatory CNS tone, is postulated to result in nerve cell death and loss of dendritic arborization (
24).
Treatment and evidence
Assessing and treating mood disorders and pain simultaneously is the best strategy for improved outcomes and often involves an approach of rational polypharmacology (
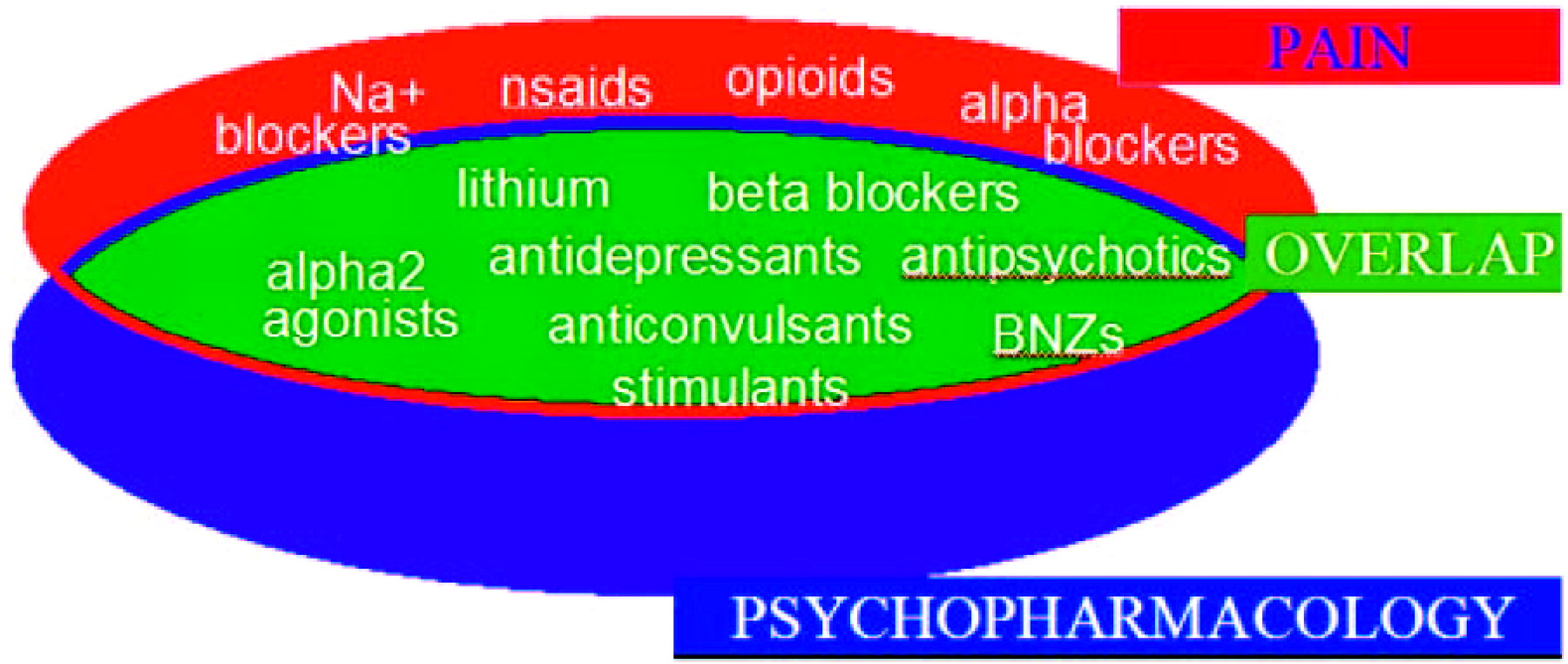
27). It is notable that the pharmacopeia for the disciplines of pain medicine and psychiatry have major overlap. Figure 2 reveals that most major drug groups used in psychiatry are also used as analgesics. Whereas some analgesics used for treating chronic pain work on peripheral pain targets, most have mechanisms of action in the CNS. The major classes of medication to treat chronic pain include opioids, antiinflammatory agents, antidepressants, antiepileptic drugs, and antiarrhythmic agents. The use of many antidepressant, antiepileptic, and antiarrhythmic drugs for neuropathic pain may be viewed as use of a single drug class, as agents in each of these drug groups possess membrane stabilization properties such as those seen in local anesthetics. The use of tricyclic antidepressants (TCAs) as part of this group may be perplexing to some until their sodium channel blockade properties are considered. This sodium channel blockade is identical to the properties of local anesthetics and almost certainly contributes to the neuropathic analgesic effects of TCAs as well as to their potential cardiotoxicity. Drugs such as venlafaxine and duloxetine appear to reduce neuropathic pain independent of their antidepressant effects. However, unlike all of the other drugs mentioned above, these do not appear to be membrane stabilizers and their exact mechanism of neuropathic analgesia is not clear.
In patients with comorbid pain and affective disorder, it is often impossible to determine which is primary and which is secondary. The overlap of the pharmacopeia for pain and psychiatric disorders is the result of the many commonalities of the underlying neurochemistry (Figure 2). Some pharmacological effects that are beneficial for analgesia may be viewed as side effects of the medications when they are used for psychiatric purposes, such as TCA-related sodium channel blockade or sedation induced by mirtazapine. Others are direct therapeutic benefits, but on alternate pathways than those seen for normal treatment, such as serotonergic and noradrenergic effects of serotonin-norepinephrine reuptake inhibitors (SNRIs) or TCAs on the dorsal horn of the spinal cord to regulate pain. Still other effects reflect a shared response for pain and affective disorders in the brain itself, for example, the calcium channel-blocking effects of lamotrigine. For these reasons and others, treating the affective component of patients with chronic pain usually reduces pain and treating the painful component of patients with affective disorders often reduces mood and anxiety disturbances.
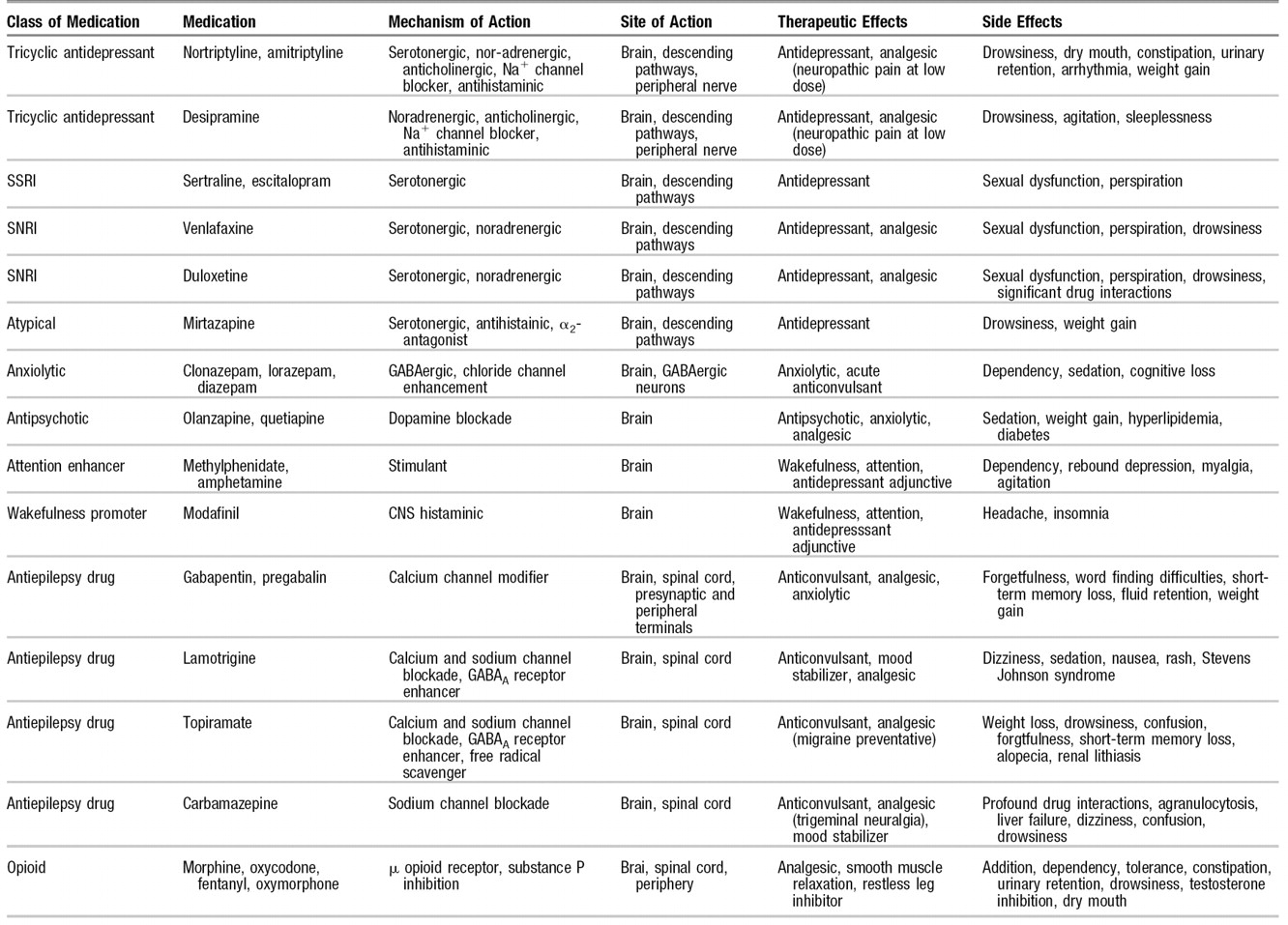
Table 2 highlights medications used for pain with strong psychotropic effects. Opioids are included in this group, with their major psychotropic actions being undesirable. The medications are reviewed by their class, mechanisms of action, site of action, therapeutic effects, and side effects. Although not an exhaustive list, this list can be used as a reference when one is considering monotherapy and polypharmacology for treating comorbid pain and affective disorders. Although it provides a compendium of drugs, this table does not cover all medications available for either pain or psychiatric treatment. The art of treating these pain and psychiatric disorders is in the selection and combination of agents that maximize efficacy, while minimizing side effects and drug interactions.
Questions and controversies
Most major psychiatric drug groups are also used for analgesia (Figure 1). This confluence of therapeutic effect is unlikely to be a coincidence; the
algesic effect of major affective disorders and the
analgesic effects of treating these conditions would predict this overlap. New medications, such as pregabalin and duloxetine, hold promise as single agents to treat disorders that comprise anxiety, depression, and pain as comorbidities (
28).
For a drug to be directly analgesic, the analgesia must be independent of the drug’s other psychiatric effects. The classic examples are the TCAs that, with their sodium channel blockade properties, are demonstrably analgesic, whereas selective serotonin reuptake inhibitors (SSRIs) have not convincingly been shown to be better than placebo for neuropathic pain. Nonetheless, many patients whose depression improves from SSRI therapy also report a decrease in pain. What is it about the SNRIs duloxetine and venlafaxine that make them analgesic independent of their antidepressant action? Perhaps this efficacy has to do with the SNRI norepinephrine blockade that usually occurs only at higher doses than serotonin blockade, and may be predictable by the mechanism of action of SNRIs, despite their lacking the sodium channel-blocking effects of tricyclic antidepressants. On the other hand, there have been colossal failures in both pain medicine and psychiatry when clinical studies have attempted to predict efficacy based on mechanism of action. For instance, recently tested Substance P inhibitors failed as antidepressants and analgesics.
In treating a patient with an affective disorder and pain, there is a natural tendency to want to treat with monotherapy. This often does not work, because dosing for the affective disorder and pain often requires different titrations. When dealing with patients with comorbid conditions, practitioners need to recognize that patients are in an amplified state. Affective symptoms, as well as side effects, are going to be even less well tolerated. For instance, in treating a patient who has postherpetic neuralgia and depression, a low-dose TCA may be effective for pain relief, but treatment of the depression may require a much higher dose that may be accompanied by unacceptable side effects. Use of a TCA at low dose or an anticonvulsant for pain and separate antidepressant dosing of an SSRI for mood may result in greater efficacy and fewer adverse effects.
Although the analgesics with the broadest efficacy are opioids, their use for treating chronic pain remains controversial. Opiophobia remains a reality for many physicians, although this is slowly yielding to a more balanced use of drugs in this therapeutic class. Opioids are useful in long- and short-acting forms, are delivered via every route of administration, treat nociceptive and neuropathic pain, have few drug interactions, and are relatively safe if treatment is properly supervised. They are, however, highly abused and diverted for profit, leading to their heightened state of regulation. Such need for pharmacovigilance, as well as their stigma as abusable drugs is too often seen as a reason to avoid using opioids. Instead less regulated or scrutinized drugs are frequently substituted, despite less efficacy or greater risk.