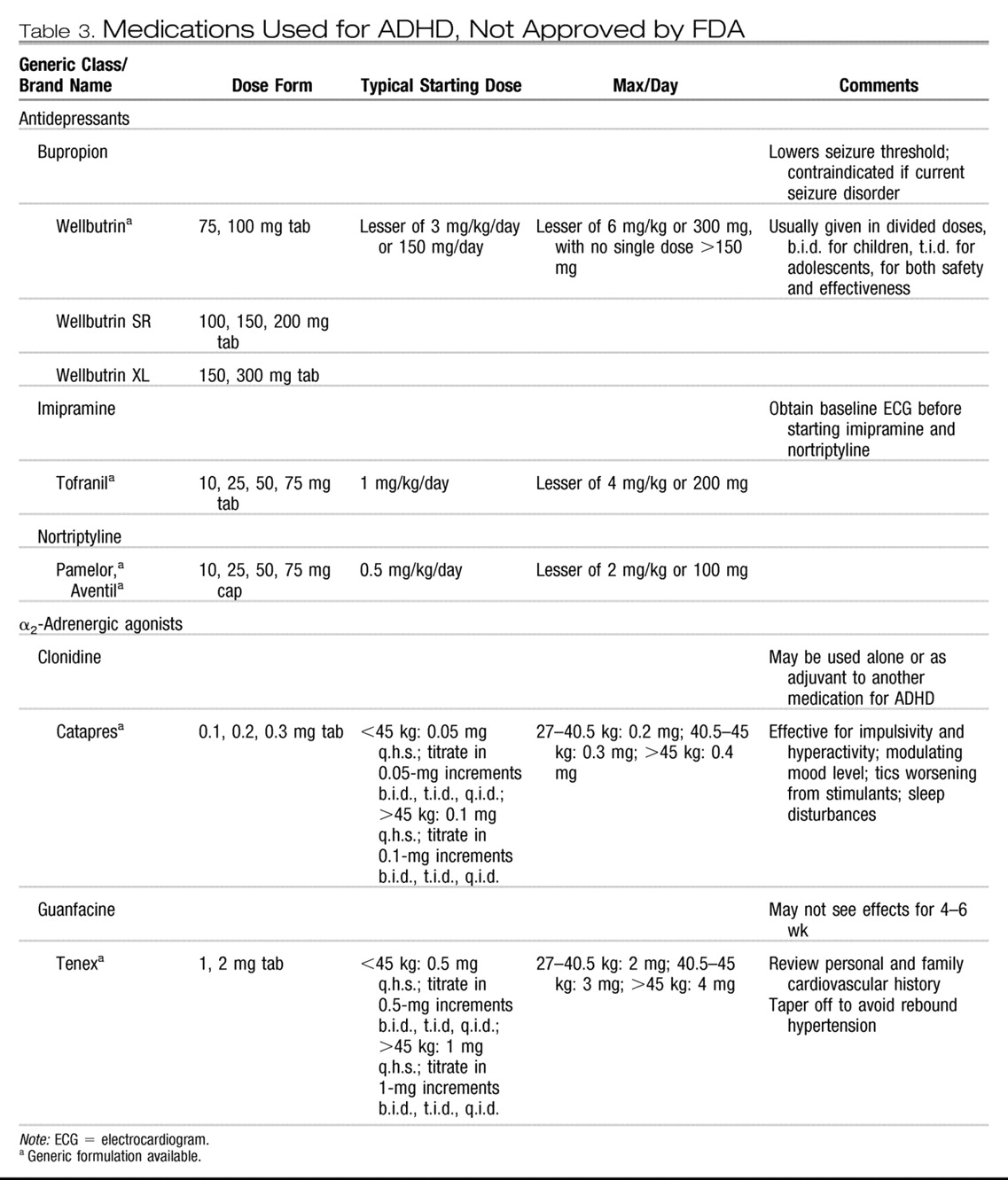
Bupropion may cause mild insomnia or loss of appetite. Extremely high single doses (>400 mg) of bupropion may induce seizures even in patients without epilepsy. TCAs frequently cause anticholinergic side effects such as dry mouth, sedation, constipation, changes in vision, or tachycardia. Reduction in dose or discontinuation of the TCA is often required if these side effects induce impairment. Side effects of α-agonists include sedation, dizziness, and possible hypotension. In the previous decade there was controversy over the safety of the use of α-agonists, particularly clonidine, in children.
Swanson and colleagues (1995) noted about 20 case reports of children suffering significant changes in heart rate and blood pressure, particularly after clonidine dose adjustment. Four cases of death were reported in children taking a combination of MPH and clonidine, but there were many atypical aspects of these cases (
Popper, 1995;
Swanson et al., 1995,
1999b;
Wilens and Spencer, 1999), and
Wilens and Spencer (1999) doubted any causative relationship between the stimulant-agonist combination and the patients' deaths. There have been no further reports of severe cardiovascular adverse events associated with clonidine use in ADHD patients. Nonetheless, physicians must be cautious. The patient's blood pressure and pulse should be assessed periodically (
Gutgesell et al., 1999), and abrupt discontinuations of the α-agonist are to be avoided. The patient and family should be advised to report any cardiac symptoms such as dizziness, fainting, or unexplained change in heart rate.
Recommendation 10. If a patient with ADHD has a robust response to psychopharmacological treatment and subsequently shows normative functioning in academic, family, and social functioning, then psychopharmacological treatment of the ADHD alone is satisfactory [OP].
Whether combined medication and psychosocial treatment of uncomplicated ADHD yields improved outcome relative to medication treatment alone remains a contentious issue. For children with ADHD alone who do not have significant comorbidity, the MTA and M+MPT studies do not for the most part show an additive effect of the psychosocial interventions. In the first set of analyses of the MTA data, the four groups were compared over time on quantitative measures of ADHD symptoms; there was no significant difference between the comprehensive medication management group and the combined treatment group. In a subsequent set of analyses, an advantage for the combined treatment was seen.
Swanson et al. (2001 [rct]) created a “categorical” outcome measure using the Swanson, Nolan, and Pelham (SNAP) behavior rating scale. Successful treatment was defined as having an average symptom rating no greater than 1.0 (“just a little”). Using this definition, 68% of the combined group was optimally treated, compared with 56% of the medication-only group, a statistically significant difference. Behavioral treatment alone remained inferior to medication management, with only 34% of the behavioral treatment group maximally improved.
Combined treatment did not yield superior outcome to medication only in the M+MPT study. After 2 years of intensive psychosocial intervention and MPH, children with ADHD (without learning problems or comorbidities) were no different from those treated with medication alone in terms of ADHD symptoms (
Abikoff et al., 2004b [rct]), academics (
Hechtman et al., 2004 [rct]), or social skills (
Abikoff et al., 2004a [rct]). Children in the MTA study were studied for 1 year after the end of active intervention. No benefit of combined treatment was found over medication alone, and stopping medication was strongly related to deterioration (
MTA Cooperative Group, 2004a [rct],
2004b [rct]). Overall, the data suggest that for ADHD patients without comorbidity who have a positive response to medication, adjunctive psychosocial intervention may not provide added benefit. Therefore, if a patient with ADHD shows full remission of symptoms and normative functioning, it is not mandatory that behavior therapy be added to the regimen, although parental preferences in this matter should be taken into account.
Recommendation 12. Patients should be assessed periodically to determine whether there is continued need for treatment or if symptoms have remitted. Treatment of ADHD should continue as long as symptoms remain present and cause impairment [MS].
The patient with ADHD should have regular follow-up for medication adjustments to ensure that the medication is still effective, the dose is optimal, and side effects are clinically insignificant. For pharmacological interventions, follow-up should occur at least several times per year. The number and frequency of psychosocial interventions should be individualized as well. The procedures performed at each office visit will vary according to clinical need, but during the course of annual treatment, the clinician should review the child's behavioral and academic functioning; periodically assess height, weight, blood pressure, and pulse; and assess for the emergence of comorbid disorders and medical conditions. Psychoeducation should be provided on an ongoing basis. The need to initiate formal behavior therapy should be assessed and the effectiveness of any current behavior therapy should be reviewed.
The history of medication treatment of ADHD now spans nearly 70 years, which is longer than the use of antibiotics (
Bradley, 1937). The MTA clearly showed that once the study treatments ceased at 14 months, the combined and medication groups lost some of their treatment gains, in part because of medication discontinuation and in part because the medication was now being given in the community with less careful monitoring and dose adjustment (
MTA Cooperative Group, 2004a [rct],
2004b [rct]). In contrast, in the M+MPT study, all of the medication treatment was performed in the study. There was no deterioration in clinical effect or compliance, even in the second year, when the intensity of psychosocial treatment was greatly reduced (
Abikoff et al., 2004b [rct];
Klein et al., 2004 [rct]). Given the high level of maladaptive behavior among adolescents with ADHD (
Barkley et al., 2004), continued psychopharmacological intervention through this developmental period is likely to be highly beneficial. At the time of the 1997 AACAP practice parameter on ADHD, few long-term medication treatment studies of children with ADHD were available. One of the first controlled long-term stimulant studies studied the effects of DEX (
Gillberg et al., 1997 [rct]). Children with ADHD (
n = 62) were successfully treated with DEX in a short-term, open-label trial and then randomized to either placebo or DEX in a double-blind, parallel-group design for up to 1 year of treatment. Significantly more children relapsed in the placebo group (71%) than in the DEX group (29%), and the stimulant group showed significantly more improved ratings on the Conners Parent Rating Scales than the placebo group as the study progressed.
Charach et al. (2004) followed 79 of 91 participants from a clinical trial of MPH for an additional 5 years; 69 of these subjects remained in the study through year 5. Adherence to stimulant (defined as taking the medication at least 5 days a week since the last evaluation with no drug holidays that exceeded 14 weeks) was assessed at each year of the study. At 5 years, adherents showed greater improvement in teacher-reported symptoms than nonadherents; nonetheless, many subjects had discontinued their stimulant medication.
With the introduction of long-acting stimulants and atomoxetine, longer term (1–2 years) open-label follow-up safety studies have been performed. Caution needs to be used when interpreting many of these studies due to their open-label nature and high rates of attrition. Follow-up data from long-term, open-label Concerta studies are available from both the first (
Wilens et al., 2003a [ut]) and second year of treatment (
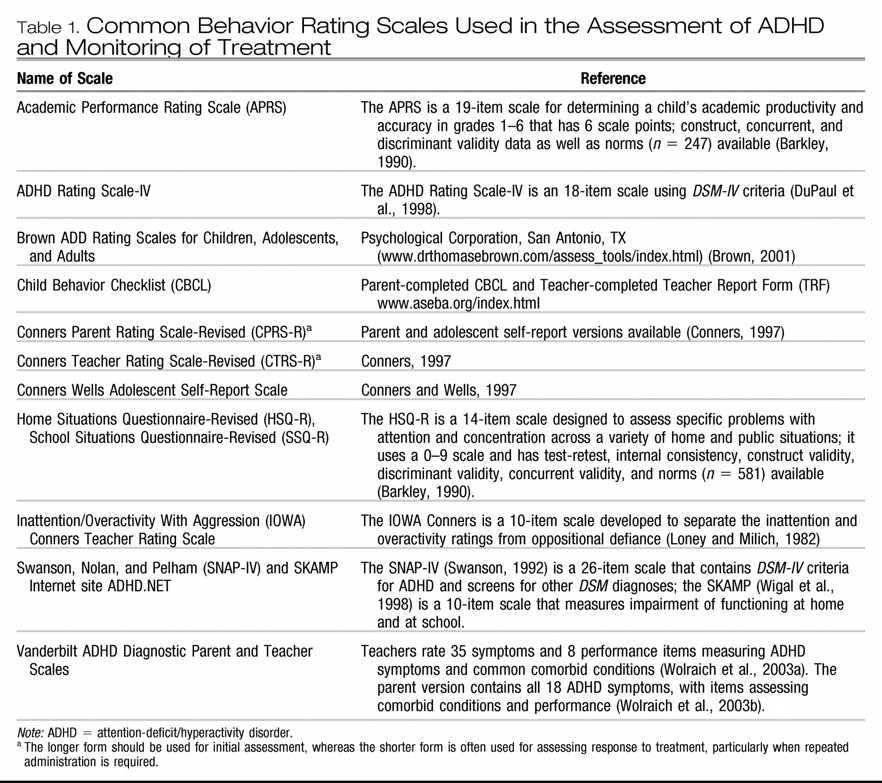
Wilens et al., 2005 [ut]). In these studies, 497 children ages 6–13 years who had participated in double-blind, placebo-controlled studies of Concerta were studied regularly over the study period. Patients received adjustment of their daily dose of Concerta according to clinical need. Teacher and Parent Inattention/Overactivity With Aggression (IOWA) Conners Rating Scales were obtained monthly in year 1, and in year 2, global evaluations of the effectiveness of the Concerta were made by parents and teachers every 3 months. In year 1, the subjects' mean Inattention/Overactivity and Aggression/Defiance ratings done by both parents and teachers remained in the normative range throughout the study period. The mean prescribed dose of Concerta rose from 35 mg to 41 mg by the end of year 1. Thirty-one subjects (7.6%) discontinued because of lack of effectiveness. Overall, 289 subjects completed year 1 of treatment. Two hundred twenty-nine subjects completed year 2; none of these dropped out because of lack of efficacy. Using the last observation carried forward, 85% of parents rated the effectiveness of the medication at the study's end as good or excellent.
A 24-month follow-up study of Adderall XR showed similar long-term effectiveness (
McGough et al., 2005 [ut]). Subjects
(N = 568) began treatment with Adderall XR with 10 mg/day, and investigators individually titrated doses up to a maximum of 30 mg/day; 273 (48%) completed treatment. By 24 months, the mean dose of Adderall XR was 22.4 ± 6.9 mg. Each quarter of the study period, subjects' parents completed the 10-item Conners Parent Rating Scales; these ratings remained in the normative range throughout the 2-year period.
Long-term atomoxetine treatment was studied in 416 patients ages 6–15 years (
Michelson et al., 2004 [ut]). Patients were treated in an open-label study of atomoxetine for 12 weeks, and then they were randomized to either placebo or atomoxetine for 9 months. Atomoxetine was superior to placebo in preventing relapse, with 22.3% of atomoxetine subjects showing a return to baseline severity versus 37.9% in the placebo group.
Wilens et al. (2004 [ut]) reported on the follow-up of 601 adolescents with ADHD treated with atomoxetine, of whom 219 had completed 2 years of treatment. Subjects took doses of atomoxetine beginning at 1.2 and 2.0 mg/kg/day with a mean dose of 1.4 mg/kg/day. Ninety-nine (16.5%) discontinued the atomoxetine because of a lack of efficacy. Mean Parent ADHD Rating Scale-IV scores (assessed every 3 months) for the group fell into the normative range by the third month of treatment and remained until the end of the study.
Recent controlled trials of long-acting stimulants have confirmed the lack of any major medical adverse events with this class of medications, with no short-term abnormalities of hematological or chemical measures (
Biederman et al., 2002 [rct];
Greenhill et al., 2002 [rct];
McCracken et al., 2003 [rct];
Wolraich, 2000 [rct];
Wolraich et al., 2001 [rct]). Although stimulants are a controlled substance, a meta-analysis of open-label long-term studies of stimulant treatment in ADHD concluded that stimulant treatment does not increase the risk of substance abuse and may even have a protective effect (
Wilens et al., 2003b). Side effects that tend to persist in long-term treatment with all stimulants include insomnia, decreased appetite and/or weight loss, and headache (
Charach et al., 2004 [ut];
Gillberg et al., 1997 [rct];
McGough et al., 2005 [ut];
Wilens et al., 2005 [ut]). In the long-term Adderall XR study (
McGough et al., 2005), 84 patients (15%) discontinued medication because of side effects. In the 2-year Concerta study, 28 (6.9%) discontinued the study because of side effects in the first year, and an additional three subjects did so in the second year (
Wilens et al., 2005). Two studies (
Gillberg et al., 1997;
Law and Schachar, 1999 [rct]) compared outcomes of children with ADHD treated with stimulant or placebo during a 6-month period. Neither study showed that DEX or MPH produced tics at a rate exceeding that of placebo.
Gillberg et al. (1997) did not find that DEX-treated children have higher rates of anxiety or depression than those on placebo after 6 months of treatment. Although side effects to medications used in the long-term treatment of ADHD can be problematic and require the attention of the clinician when they occur, they are without serious medical sequelae and of mild to moderate intensity, and generally respond to dose adjustment or change of medication.
As patients with ADHD enter late adolescence, clinicians and the family face the question of whether symptoms of ADHD and social functioning have improved to the point that medication intervention is no longer needed. Long-term follow-up of MTA subjects (now followed for 8 years after they started treatment with data analyzed at the 2-year follow-up point published) has begun to shed some light on this issue. Subjects showed marked improvement during the first 14 months of the active study period, with more gradual improvement thereafter (
Jensen, 2005 [ut]). Children who continued to be impaired were more likely to have ODD or CD, both at baseline and at follow-up. For the entire MTA group, treatment group effects (medication versus no medication, combined treatment versus medication alone) at 22 months were no longer significant. Secondary analyses of these data were performed to explore possible reasons for the loss of the effectiveness of the MTA medication management over the longer period of time (
Swanson, 2005 [ut]). These analyses found that the ADHD sample fell into three groups: children with initial small improvements followed by gradual improvement over time, children with a large initial improvement who maintained improvement over the 36 months, and children who showed initial improvement but then deteriorated. This third group had higher levels of aggression and lower IQs at baseline. Medication effects on functioning were significant at follow-up only in the first two groups. The first group showed improved performance if they were on medication at follow-up, whereas the second showed more improvement if they had received the MTA medication titration algorithm at the start of treatment. Interestingly, in the second group, current medication status did not affect outcome, meaning that some children maintained gains even though they were no longer taking medication. This implies that the clinician must be alert to the fact that some patients with ADHD deteriorate in spite of medication (and these are more likely to have comorbidity at baseline), whereas others do show remission of symptoms and may no longer require medication management.
If a patient with ADHD has been symptom free for at least 1 year, then inquiries should be made about whether the patient and family still think the medication provides a benefit. Signs that the ADHD has remitted include lack of any need to adjust dose despite robust growth, lack of deterioration when a dose of stimulant medication is missed, or new-found abilities to concentrate during drug holidays. Low-stress times such as vacations are a good time to attempt a withdrawal from medication, but parents should assign some cognitively demanding tasks (reading a book, practicing mathematics problems) to be sure that remission has occurred. The start of a new school year is not a good time to attempt a drug holiday, but once a patient's school routine is established, the medication can be withdrawn and teacher input solicited. Medication should be reinstituted if the patient, parents, or teachers report deterioration in functioning.
Recommendation 13. Patients treated with medication for ADHD should have their height and weight monitored throughout treatment [MS].
The effect of stimulant treatment on growth has been a concern for many years. The 1997 practice parameter on ADHD noted that stimulants were associated with small decreases in expected height and weight gain, which were rarely clinically significant (
American Academy of Child and Adolescent Psychiatry, 1997). In the late 1990s concern about effects on growth abated, particularly because follow-up studies did not show any long-term effect on ultimate adult height (
Gittelman-Klein and Mannuzza, 1988;
Kramer et al., 2000;
Weiss and Hechtman, 2003). Recently, however, two major reviews (Faraone et al., unpublished data, 2006; Poulton, 2005) examined all of the available data and concluded that stimulant treatment may be associated with a reduction in expected height gain, at least in the first 1 to 3 years of treatment. It is difficult to determine the clinical significance of such changes. The MTA study showed reduced growth rates in ADHD patients after 2 years of stimulant treatment compared with those patients who received no medication (
MTA Cooperative Group, 2004b [rct]), and these deficits persisted at 36 months (MTA Cooperative Group, 2006 [rct]). The PATS study followed a group of 140 preschoolers who received MPH for up to 1 year for ADHD (
Swanson et al., 2006 [rct]). The subjects had less than expected mean gains in height (−1.38 cm) and weight (−1.3 kg). Interestingly, in both the PATS and MTA studies, ADHD subjects were larger than average (∼0.2 SD above the mean) for both height and weight compared with controls or normative data before entry into the study, especially for treatment-naïve subjects.
Swanson et al. (2006 [rct]) hypothesized that children with ADHD are bigger, on average, than an age-matched sample of children without ADHD. Thus, clinicians may not observe growth deficits in stimulant-treated children because treatment does not slow the height acquisition rate enough to bring them below the mean height for age. In a review and analysis of cross-sectional data,
Spencer et al. (1996) compared the heights of ADHD patients with those of controls in three separate age samples. They found no height deficits relative to controls in childhood, a small but statistically significant reduction in height relative to controls at puberty, but no difference in height in adulthood. There was no relationship between stimulant treatment and height measures, and
Spencer et al. (1996) hypothesized that ADHD itself was associated with a slower tempo of growth, which resolved by adulthood, and the shorter stature was unrelated to medication effects. There is also evidence that stimulant-induced growth delays are greater in the first year of treatment but attenuate after that (
Faraone et al., 2005a;
Spencer, 2003).
Charach et al. (2006) found that higher doses of stimulant correlated with reduced gains in height and weight; indeed, the effect did not become significant until the dose in MPH equivalents was >2.5 mg/kg/day for 4 years.
Pliszka et al. (2006b) did not find that children with ADHD treated with monotherapy with either amphetamine or MPH showed any failure to achieve expected height; furthermore, the two stimulant classes did not have any differential effect on height, but amphetamine had somewhat greater effects on weight than MPH. The subjects in this study had drug holidays averaging 31% of time during their treatment course, which may have contributed to the lack of effect of the stimulant on height.
In assessing for clinically significant growth reduction, it is recommended that serial plotting of height and weight on growth charts labeled with lines showing the major percentiles (5th, 10th, 25th, 50th, 75th, 90th, and 95th) be used (
Mei et al., 2004). This should occur one to two times per year, and more frequently if practical. If the patient has a change in height or weight that crosses two percentile lines, then this suggests an aberrant growth trajectory. In these cases a drug holiday should be considered if return of symptoms during weekends or summers does not lead to marked impairment of functioning. The clinician should also consider switching the patient to another ADHD medication. It is important for the clinician to carefully balance the benefits of medication treatment with the risks of small reductions in height gain, which as of yet have not been shown to be related to reductions in adult height (
Gittelman-Klein and Mannuzza, 1988;
Kramer et al., 2000;
Weiss and Hechtman, 2003).