One might expect that LBD patients would present with a combination of parkinsonian and Alzheimer-like features, and this seems to be the case.
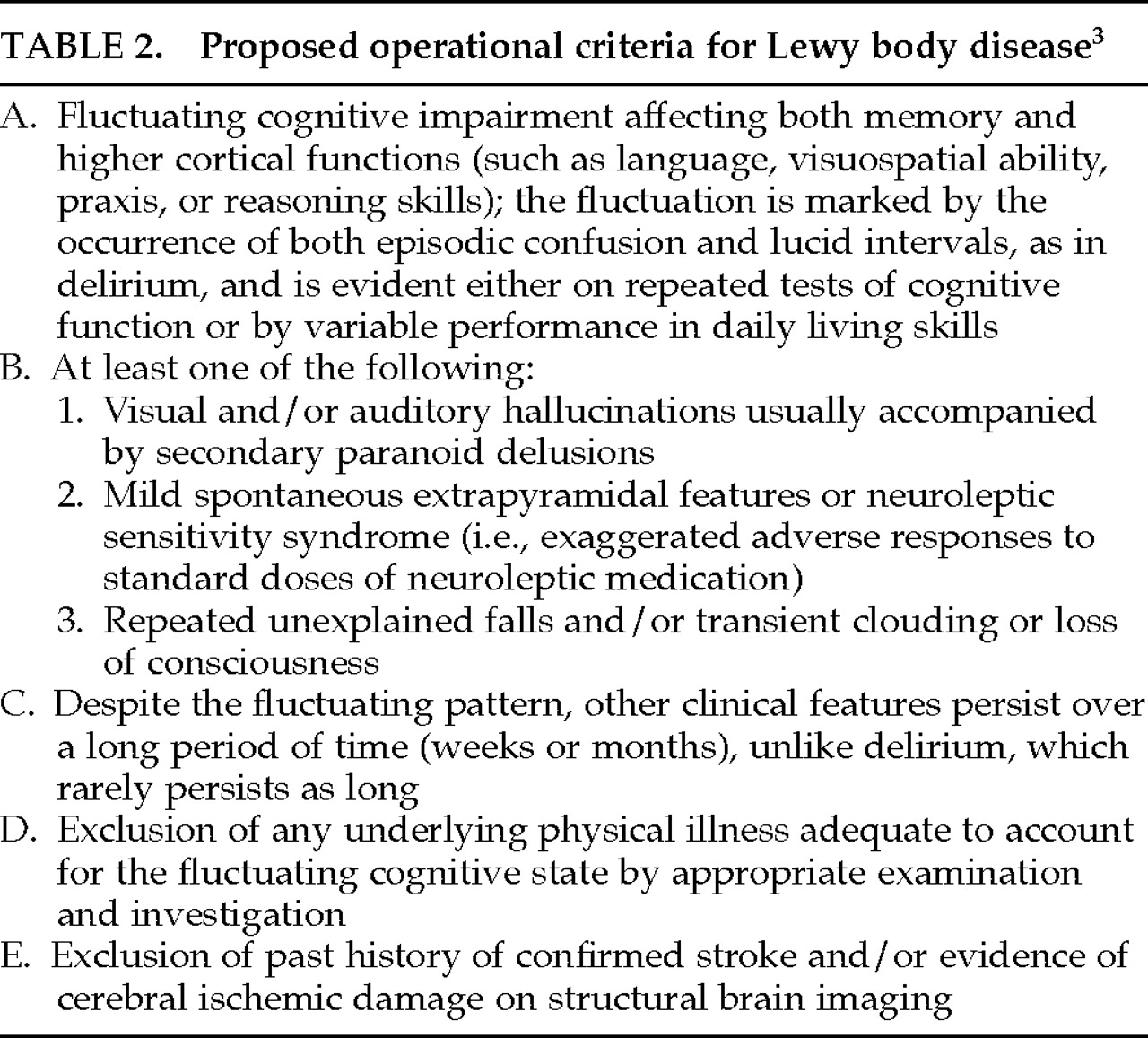
2 The clinical profile emerging from independent, retrospective studies based on autopsy diagnosis includes 1) a cortical Alzheimer-like dementia characterized by loss of memory, orientation, and visuospatial skills; 2) extrapyramidal signs of a more mild nature than seen in classic PD; and 3) psychiatric symptoms including hallucinations, delusions, and/or depression. Fluctuations in cognitive state and disturbances in consciousness have also been reported,
3,4 as have adverse reactions to antipsychotic agents.
3,27–30 Each of these categories of behavioral symptomatology is discussed in more detail in the following sections. Other, less commonly reported symptoms are severe weight loss
31,32 and orthostatic hypotension.
33Demographics
The prevalence of this disease appears to be higher in males than in females,
3,6,24,27,33–37 in a ratio of about 2:1
31,37 or higher.
27,33,35 The age at onset ranges between 50 and 83 years,
31,33,38 and the reported mean age at death varies from 68.4 years to 92 years.
33 The reported duration of the illness is equally variable, ranging from less than 1 year to 20 years,
31,38 with a mean of 3.3
4 to 6 years.
34,38,39 The crude prevalence and incidence are not yet known.
A positive family history for AD in at least one first-degree relative of patients affected with LBD has also been reported.
2,34 Recent evidence suggests that the apolipoprotein E4 (APOE E4) allele, in particular, is a major risk factor for developing LB pathology.
40,41 However, in one study of 122 autopsied patients, 39.2% of AD cases had the APOE E4 allele, compared with only 6.25% to 29% of LBD cases.
42 Hence, further investigation of a genetic predisposition for developing LBD is warranted.
Neuropsychological Features
The distinguishing characteristics of dementia associated with LBD have not been well studied or described, although impairments of memory,
27,33,38 language, and visuospatial skills
27,38 have been noted. Since this pattern of cognitive deficits is similar to that observed in AD,
43 clinicians face the difficult issue of differentiating these two dementing illnesses. Because extrapyramidal features are also common in LBD, the differential diagnosis is further complicated by dementia associated with PD, which typically is characterized by impairments in short-term memory, concept formation, and mental flexibility.
44 Despite the reportedly high prevalence of dementia in PD,
45 systematic comparisons of LBD and demented PD patients are lacking in the literature.
Across studies assessing differences between LBD and AD dementia, results have been mixed and seem to vary with differing methodologies. Some evidence from retrospective studies suggests that the dementia of LBD is less severe than that of AD when patients are matched on the basis of age. For example, on gross screening measures such as the Blessed Information-Memory-Concentration test (IMC),
46 LBD patients have evidenced less severe impairments than AD patients,
3,4 particularly on questions involving short-term memory.
3 In addition, AD patients showed more severe deterioration than LBD patients.
4 However, when matched on the basis of disease duration,
47 LBD and AD patients performed comparably on gross cognitive screening measures, including the Mini-Mental State Examination (MMSE),
48 the IMC, and the Dementia Rating Scale.
49Few studies are available in which performance on comprehensive neuropsychological test batteries was used to make comparisons between these populations. In one such study, where patient groups were first matched on the basis of IMC scores, LBD patients evidenced greater impairments than AD patients on standardized measures of attention, verbal fluency, and visuospatial/constructional skills.
2 Unfortunately, the matching procedure used in this study may have conferred a bias against the AD patients, who typically perform more poorly on the IMC.
3,4 In another study using a standardized neuropsychological test battery, significant performance differences between AD and LBD patients were not found.
47Our impression from these studies is that methodological differences, including differing definitions of the disease (e.g., differing neuropathologic criteria), limit between-study comparisons, and consequently no clear neuropsychological profile of LBD has emerged. Procedurally, the basis on which subjects are matched—age or disease duration—is one variable that critically affects the obtained results. Furthermore, it appears that gross and standardized psychometric tests may not be sensitive to the morphologic differences between LBD and AD dementia.
Prospective studies using more refined tests have revealed greater impairments in LBD than AD patients on some cognitive tasks.
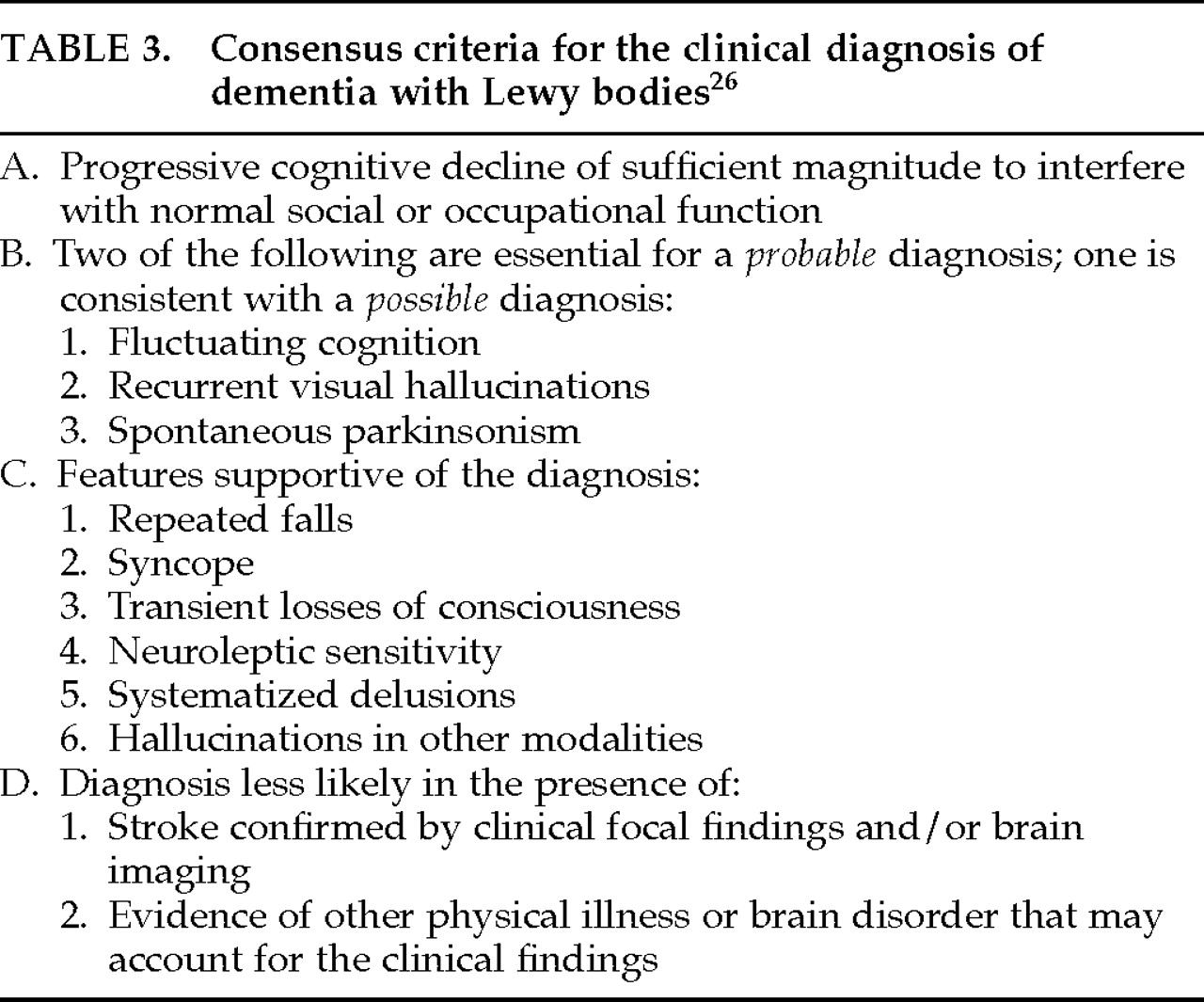
50,51 LBD patients (diagnosed with criteria of McKeith et al.
3) performed more poorly than AD patients on delayed-matched-to-sample,
51 a task requiring subjects to remember a presented stimulus over a designated delay and then to select that stimulus among a choice of distractors. The poorer performance of LBD patients may suggest the early involvement of temporal lobe structures, which are critical substrates to the successful completion of this task.
52 LBD patients also have shown greater impairments than AD patients on a conditional learning paired associate task.
50Certainly, further exploration is needed of the characteristic differences between AD dementia and LBD dementia. Such studies should also include PD patients with dementia, since comparisons with this group are currently lacking and are needed to facilitate accurate differential diagnosis of LBD. A prerequisite for the success of this proposed research will be more precise neuropathologic criteria for LBD. Future investigations should include quantitative and qualitative assessments of AD, PD, and LBD patients across multiple cognitive domains. In addition, it seems likely that standardized psychometric tests may be insufficient for detecting differences between these patient populations and that more sensitive measures will have to be developed and used.
The underlying neuropathological mechanisms of the dementia associated with LBD also need to be elucidated. Whether the observed dementia is due to cortical LBs, brainstem LBs, neuronal loss, and/or AD-like neuropathology is not known. A few studies have revealed a relationship between cortical LB density and severity of dementia,
47,53 but the predictive relationship between these variables has not always been observed.
43 There is still no consensus on the relative contribution of AD-like plaques and tangles, also common in LBD,
2,4,33–35 to LBD dementia.
47,54–55 Although counts of neurofibrillary tangles in neocortex have been shown to be significantly correlated with dementia in AD patients, Samuel et al.
47 reported that this relationship was comparatively weak in LBD patients. Subcortical pathology, such as neuronal loss in the nucleus basalis of Meynert, has been associated with other dementing syndromes,
35,56 although researchers have thus far failed to support the relationship between brainstem LBs and degree of dementia.
4Cognitive Fluctuations and Disturbances of Consciousness
In findings related to dementia, some investigators consistently have noted characteristic fluctuations in cognitive ability in patients with LBD,
3,16,38 leading some to suggest that this feature may be a distinguishing clinical feature of this illness.
4 These fluctuations are reported to occur in the presence of periods of relative lucidity and intact memory function and may be followed by an acute or subacute confusional state. During these episodes, patients have been described as “glazed looking” and showing “generalized twitching,”
3 “muddled” one day and “alert” the next.
38 Furthermore, it has been suggested that this type of fluctuation is not restricted to cognitive functioning, but may generalize to other mental, physical and behavioral capacities, causing extreme reductions in consciousness and arousability.
3 Some researchers suggest that this type of “switching off” does not occur until later stages of the disease,
3 whereas others report a 67% incidence of fluctuations early in the progression of LBD, compared with an incidence of 13% during later stages.
57There is not yet a consensus on the significance of this feature, nor on any standardized measure for its occurrence. Certainly, not all researchers have observed fluctuations in cognitive state in affected patients, and we conclude that the incidence of cognitive fluctuation in LBD is unknown. Most clinicians are not likely to observe these fluctuations firsthand in the context and time limitations of an office visit, or possibly not even during a short-term hospital stay. Relying on the accounts of caregivers may also be troublesome, particularly if informants do not offer the verbatim description “fluctuations in consciousness,” which few are likely to do. Directly asking caregivers about the presence of this feature may be leading, as all patients are bound to experience higher and lower points throughout a given period of time. Studies aimed at establishing objective means of assessing cognitive fluctuations in relevant patient populations are needed.
Neurological Findings
Extrapyramidal signs commonly appear during the LBD disease course, affecting at least 80% of this population.
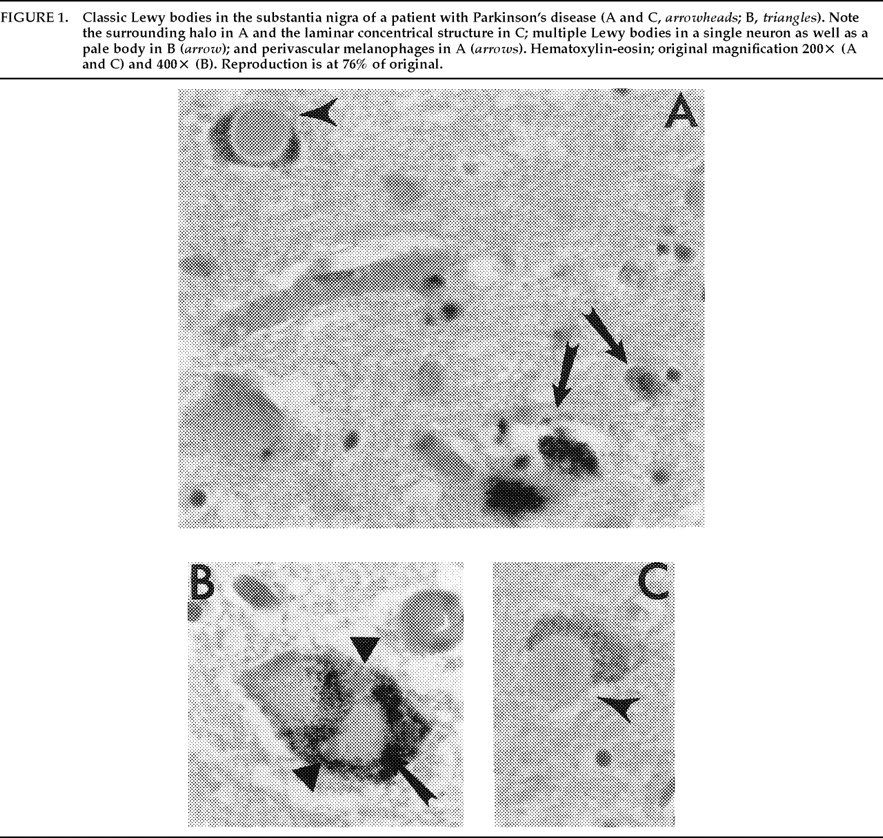
4 These neurological findings are not surprising given the common neuropathologic finding of LBs in the substantia nigra of affected individuals.
38 It is generally agreed, however, that the parkinsonism observed in LBD is more mild than that observed in PD patients
2,3,31,32 and that the classical PD triad of tremor, akinesia, and rigidity is not likely to appear.
4 Some researchers suggest that parkinsonism may be more likely to occur at later stages of the disease, a suggestion that seems supported by the finding that patients who do not show extrapyramidal signs have shorter survival durations.
27,58 We do not yet know with any reliability the course of extrapyramidal findings in LBD or their diagnostic and prognostic significance.
The extrapyramidal signs observed in LBD may be qualitatively different from those exhibited in PD, although consensus is lacking as to the characteristics of these differences. Determination of the most prominent extrapyramidal feature of LBD has varied across investigators, from rigidity
24,31 to gait impairment
32 to falling.
3 In one recent study,
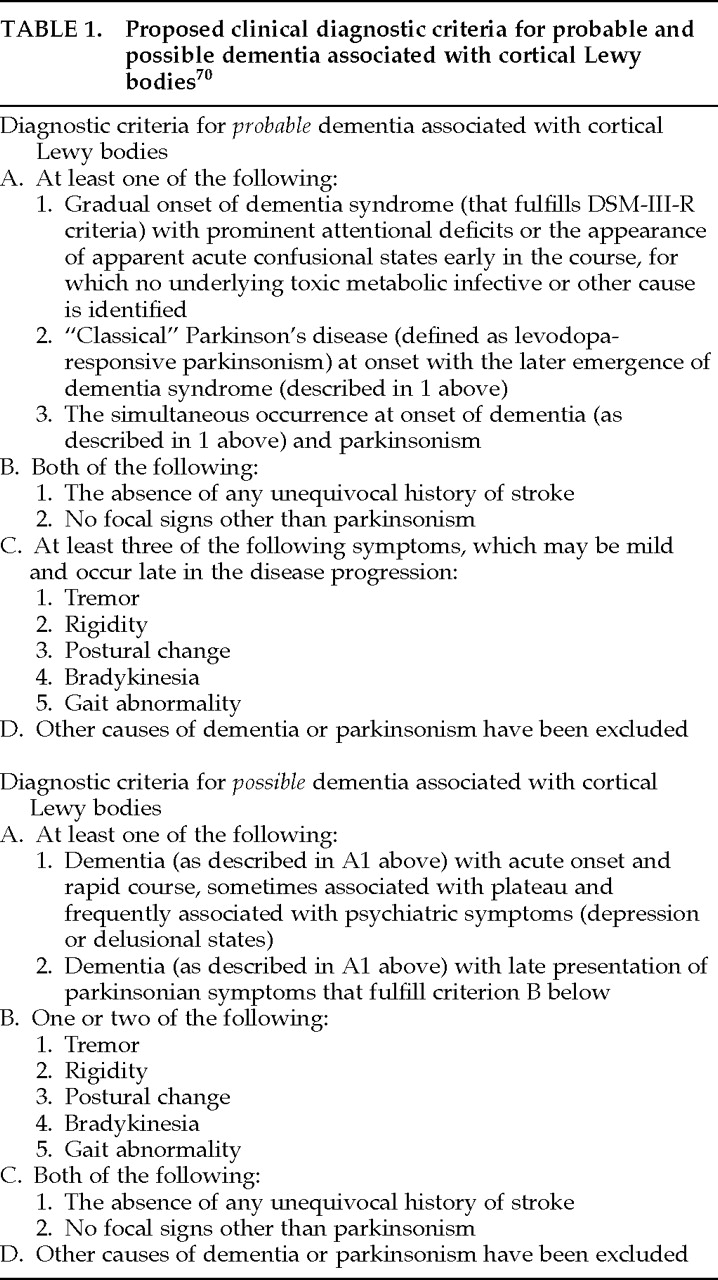
59 the presence of myoclonus, absence of rest tremor, or no trial or response to levodopa was 10 times more likely to occur in LBD than in PD. However, another study by some of the same researchers revealed a higher frequency of bradykinesia in LBD patients compared with PD patients, a nonsignificant trend toward less resting tremor in LBD patients, and a similarly high response to levodopa in both populations; taken together, these characteristics could not reliably distinguish LBD from PD patients.
60 Contrary to the latter findings regarding resting tremor, the absence of resting tremor in LBD was not supported by a separate study in which the majority of 70 autopsied LBD patients had presented with tremor onset.
61Hence, reliable qualitative characteristics of the extrapyramidal features observed in LBD cannot be determined. Some researchers even contend that at least 30%
31 to 40%
38 of LBD patients show extrapyramidal symptoms that are indistinguishable from PD. Further research investigating qualitative differences in extrapyramidal signs between PD and LBD patients is still needed.
Falls
In relation to observed parkinsonism, some researchers propose that repeated, unexplained falls are a prominent feature of LBD.
3,36 In one retrospective study of 21 LBD cases, repeated falling was reported by 38% of patients during the initial clinical visit. For 3 of these patients, episodes of falling were frequent, occurring approximately 20 times per week during the time period immediately preceding the clinical consultation. The progression of clinical symptoms was not different for LBD patients who experienced falling compared with those who did not.
3Although impaired cognition, rather than age, has been shown to be related to the incidence of falls in the elderly,
62,63 falling may be significantly more prevalent in LBD than in other age-related dementias, such as AD
3,36 and multi-infarct dementia (MID).
36 In one retrospective study comparing the clinical histories of patients affected by different age-related dementing illnesses, 50% of LBD patients, compared with 23.8% of AD and 33.3% of MID patients, had recorded histories of repeated, unexplained falls.
36 Research comparing the extrapyramidal symptoms of LBD and PD
59,60,64 has not specifically included repeated falling as a measure.
Although some researchers have described these repeated falls as “unexplainable,”
3,36 the documented extrapyramidal features of LBD, including rigidity,
31 postural instability,
2 and orthostatic hypotension,
33,65 may account at least in part for episodes of falling. Nonetheless, rigidity
66 and postural instability,
2 as well as dementia, have been observed as frequently in AD patients, in whom falling is not as prevalent.
3,36 These findings suggest that neither dementia nor these extrapyramidal signs alone can account for the frequency of reported falls in LBD patients. Significant neuronal loss in the substantia nigra of LBD cases
24 may account for at least some of the observed falling in these patients. Comparisons of falling rates between PD and LBD patients are still needed and would be useful in determining the relationship between substantia nigra neuronal loss, corresponding extrapyramidal features, and falling.
Psychiatric Correlates
Psychiatric symptoms of depression, hallucinations, and delusions have almost always been reported as a feature of LBD.
3,32,33,37,38 However, the reported rate, severity, and profile of psychiatric symptoms exhibited by LBD patients have been inconsistent. In one study, more than 83% of LBD patients presented with prominent psychiatric symptoms, even in the context of mild to moderate dementia.
32 Others have reported a lower rate of psychiatric symptoms in LBD, ranging from 17.9% to 22.2%
34 to 53%.
38 These differences in observed prevalence of psychiatric symptoms in LBD may reflect differences in methodology, including thoroughness of examination and clinical notes, size of the sample, and neuropathologic criteria for diagnosing LBD.
The specific profile of psychiatric symptoms exhibited by LBD patients varies across studies and individuals. Several researchers have reported hallucinations and delusions in up to 80% of LBD patients,
3,33 but others report a lower incidence of these two symptoms.
24,31,34 In one group of LBD patients, neither hallucinations nor delusions were experienced by any patient, and only a minority were depressed.
2 A similarly low frequency of depression was reported in another sample;
31 however, hallucinations were observed in 15% and paranoia in 12% of cases. Again, there does not seem to be a consensus yet concerning features and frequency of psychiatric symptomatology.
The psychiatric dimension of LBD is important for diagnosis because hallucinations, delusions, and depression are reported also in AD and in PD. In one study comparing the rates of different psychiatric symptoms across AD, PD, and LBD populations, investigators found that LBD patients had rates of depression and hallucinations similar to those of PD patients (50%–60%), but rates of delusions comparable to those observed in AD (approximately 50%).
37 The LBD patients described in that study also tended to experience visual hallucinations, paranoid delusions, and depression refractory to treatment. The quality (auditory versus visual) of hallucinations and delusions did not differ across groups. In that particular patient cohort, the absence of psychiatric symptoms in LBD was rare, suggesting that psychiatric features (hallucinations, delusions, depression) may be especially useful in making the diagnosis of LBD. Additional research comparing psychiatric symptomatology in LBD, PD, and AD populations is necessary to facilitate accurate clinical and differential diagnosis of LBD.
Adverse Reactions to Antipsychotic Agents
Adverse reactions to antipsychotic and tricyclic antidepressant agents by LBD patients have also been frequently reported, so much so as to be recommended by some investigators as a clinical clue to the diagnosis of LBD.
3,28 These reactions have included confusion,
27 mental impairment, and hallucinations
29,30 and have even been fatal.
28 In one retrospective study,
28 81% of 16 LBD patients given antipsychotic agents such as haloperidol, thioridazine, trifluoperazine, flupenthixol, and sulpiride had adverse reactions, compared with only 7% of AD patients. Fifty-four percent of the affected LBD patients had reactions that were considered severe. Patients receiving antipsychotic agents showed a higher mortality rate than those who did not receive antipsychotic agents or those who had mild reactions to these drugs.
The utility of known adverse reactions to antipsychotic agents in the clinical diagnosis of LBD requires further validation. Because patients other than those with LBD also may experience adverse reactions to antipsychotic drugs, comparisons of incidences of adverse reactions across different patient populations are needed.
Progression of Clinical Symptoms
The clinical progression of LBD is not clear and may vary across individuals. In general, LBD patients initially present with a dementing syndrome and possibly some neuropsychiatric disturbance
27,31,33,35,58 and/or mild parkinsonism. A smaller percentage of patients initially present with parkinsonism, which is followed by dementia.
24,35,38 The general rate of progression has not been well documented.
It is likely that what is now collectively categorized as LBD will require further refining as more is learned about both the clinical and the neuropathologic correlates of the disease. Filley,
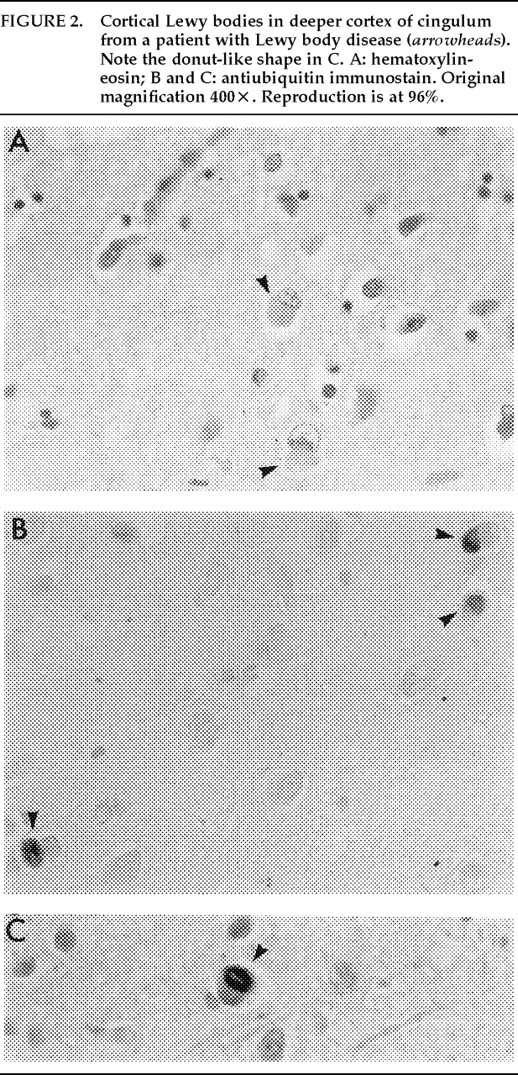
65 for example, has proposed an association between density and location of LBs and specific syndromes, ranging from incidental LBs (which are asymptomatic) to PD to diffuse LBD. He associates brainstem LBs with movement disorders, cortical LBs with dementia, and the involvement of limbic areas with psychosis and depression.
Kosaka
34 suggests instead that differences in the clinical manifestation of LBD reflect differences between proposed “common” and “pure” forms of this disease, in which “common” cases are characterized by the coexistence of cortical LBs, plaques, and neurofibrillary tangles, and “pure” cases consist of cortical LBs only. According to Kosaka, “common” cases, comprising 75% of LBD patients, initially present with memory disturbance or a psychotic state followed by dementia. “Pure” LBD patients, in contrast, present with parkinsonism as an initial symptom and are usually young adults.
Additional classification indices have been proposed by Perry et al.,
4 who distinguish “senile dementia of the LB type” from “LBD” on the basis of extent and loci of neuropathologic lesions. The phenotypic variability of this disease is also being explored.
67 The description and diagnosis of subcategories or separate nosologic entities of LBD have yet to be established; these will likely be refined with continued research and understanding of the disease process.