Human immunodeficiency virus (HIV) globally affects the central nervous system, although it appears to have a predilection for subcortical structures, especially the frontal-subcortical systems (e.g., the basal ganglia).
1–5 Damage to these structures can cause specific motor and cognitive abnormalities, including poor fine-motor precision, hypophonia, memory deficits, and difficulties performing complex cognitive tasks.
6–10 These symptoms are also common among patients with neurological disorders with cortical-subcortical involvement, such as Huntington's disease and Parkinson's disease (PD).
11–14 Damage to these systems can also cause significant neuropsychiatric syndromes, including depression, obsessive-compulsive disorder, mania, and apathy.
11,15,16 One aspect of subcortical neurological disease is the presence of motor and cognitive retardation (including deficits in mental speed and agility, spontaneity of action, spontaneity of speech for comment or question, initiative, and enthusiasm).
12–14Studies of correlation between HIV-seropositive (HIV+) subjects' perceptions of their own cognitive problems and their actual clinical status have been conducted to detect subclinical neurological or cognitive deficits.
17–23 These studies are particularly important in early stages of the HIV infection, when specific complaints may be related to early cerebral dysfunction that eventually may respond to antiviral medication. Stern et al.
17 reported a correlation between complains of neurological/cognitive problems and neuropsychological performance in asymptomatic HIV+ patients. By contrast, other studies have found complaints to be correlated with psychiatric symptoms, but not with neuropsychological performance.
18,19,21,22 In some cases motor complaints were correlated with abnormal motor performance, but not with psychiatric symptomatology.
20 Therefore, it has been suggested that there may be two groups of HIV-infected individuals who complain of problems: those whose subjective cognitive and motor complaints reflect true cognitive impairment, and those whose complaints reflect affective disorders.
20Clearly, self-reported cognitive and motor deficits in HIV infection are subject to multiple influences, including psychiatric and medical conditions and patients' own perceptions of their medical problems. However, the most common approach to the study of self-reported symptoms has been the correlation of complaints—neurological, psychiatric, cognitive, and concerning performance in activities of daily living—with actual psychiatric syndromes or cognitive measures.
17–23 Consequently, how the disease as a whole (including effects of medication) affects reports of medical problems has not been examined in detail. Most research has centered on asymptomatic patients.
17,19,20,23 Few studies included patients with acquired immunodeficiency syndrome (AIDS),
18,21,22 and only one of them examined the effects of severity of the infection on the association between psychiatric complaints and actual psychiatric syndromes.
21 Furthermore, as noted above, motor and cognitive retardation appear to be the core of the neuropsychological characteristics of the HIV infection. Although some studies have included items that investigate this aspect of the disease in their research questionnaires for self-reported symptoms,
17,20,22 none of them have examined the issue of slowness in isolation.
In this study, we examined the relationship between complaints of mental and motor slowness to medical and cognitive and psychiatric disorders, using a self-rating scale designed to assess psychomotor retardation in the subjects' activities of daily living. We hypothesized that subjective complaints of psychomotor retardation would correlate with objective clinical signs of central nervous system involvement.
METHODS
The neuropsychological and psychiatric characteristics of 72 HIV-infected individuals who completed the self-reported slowness scale were examined. These patients were part of a larger cohort that is being followed every 6 months (the Allegheny County Neuropsychiatric Survey).
24 Each patient was assessed with detailed neuropsychological, neurological, and psychosocial examinations. In addition, each had a complete physical examination, medical history, and laboratory testing focusing on HIV/AIDS-related conditions. Centers for Disease Control and Prevention (CDC) criteria for AIDS
25 were the presence or history of one or more AIDS-defining illnesses and/or a CD4 cell count of less than 200/mm
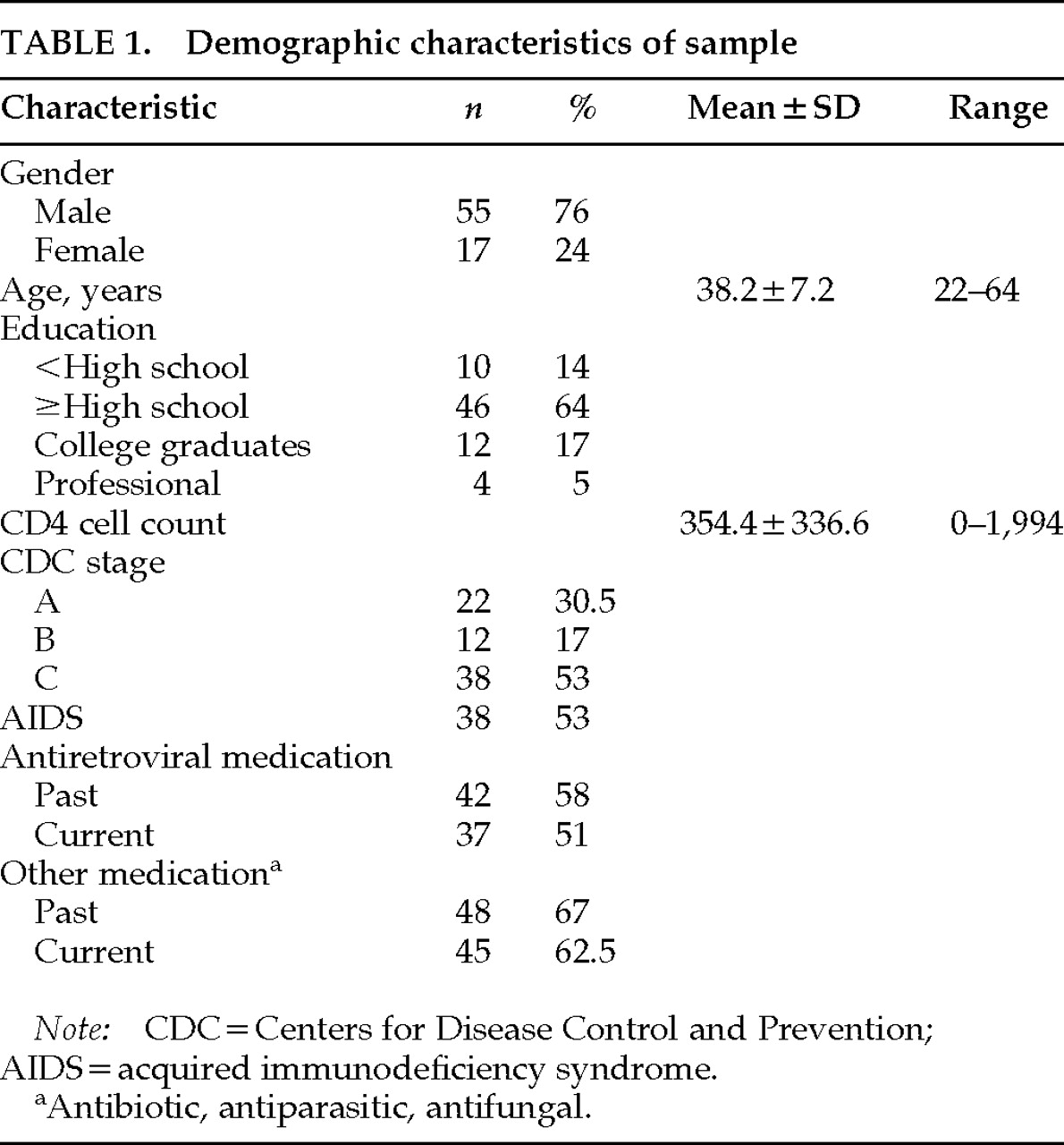
3. Demographic characteristics and CDC staging of the subjects are shown in
Table 1.
Each subject was examined for specific DSM-III-R disorders
26 including major depression, generalized anxiety disorder (GAD), adjustment disorder with depressed and/or anxious mood, alcohol abuse/dependence, and drug abuse/dependence. These disorders were assessed with the appropriate sections of the Structured Clinical Interview for DSM-III-R.
27 Interviewers were trained to assess mental health in physically ill subjects. In addition, we reviewed all medications taken by the patient before or during the presence of psychiatric symptoms and eliminated medication-induced symptomatology for purposes of determining diagnosis. Details of the psychiatric examination have been published previously.
28Each subject was tested by a trained examiner with experience in assessing physically ill, cognitively impaired adults. Each subject was assessed with a battery that included components of the Wechsler Adult Intelligence Scale–Revised,
29 Wechsler Memory Scale–Revised,
30 Controlled Oral Word Association,
31 Category Test,
32 National Adult Reading Test,
33 Word Verbal Free Recall Task,
34 Trail Making Test,
35 and Rotary Pursuit Learning Test.
36 Details of the neuropsychological battery are described elsewhere.
24 Because different patients completed the slowness questionnaire at different visits to our clinic, we have included in this study the neuropsychological measures common to all patients. Fifty patients had the neuropsychological assessment at study entry and 22 at the 6-month follow-up examination.
A medical history and physical and neurological exams were conducted by a neurologist with experience in HIV/AIDS or by a specially trained nurse. The semistructured exam included a review of systems and covered the entire central nervous system, with particular emphasis on signs and symptoms relevant to HIV-associated neurological conditions. Systemic signs included oral/throat mucosa lesions (including oral hairy leukoplakia), eyes/skin lesions (including Kaposi's sarcoma [KS]), adenomegaly, abnormal chest, lung, heart, and extremities, enlarged liver and spleen, and signs of systemic infections (such as pneumonia, upper respiratory tract infection, or genital infections). Neurological signs included abnormal cranial nerves, abnormal speech, abnormal motor tone, abnormal movements, motor deficits, sensory deficits, stereoagnosia, agraphesthesia, clonus, abnormal deep tendon reflexes (DTRs), abnormal plantar response, release signs, abnormal cerebellar testing, and abnormal gait.
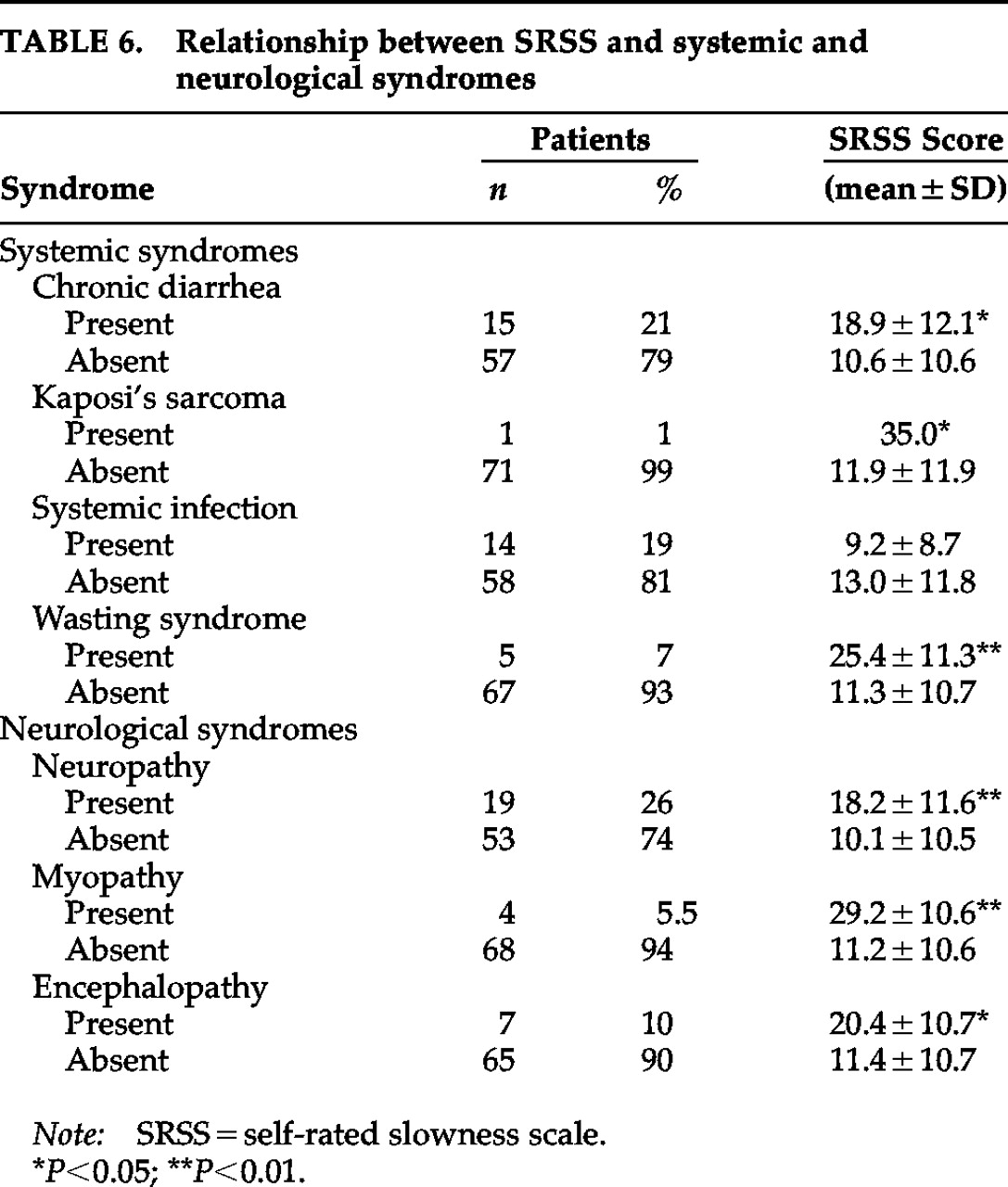
On the basis of the medical history and exam, we further investigated the relationship between slowness and the presence of four debilitating conditions: KS, chronic diarrhea, wasting syndrome, and systemic infections (such as histoplasmosis, Pneumocystis carinii pneumonia, esophageal and lung candidiasis, upper respiratory tract bacterial infection, toxoplasmosis, and cytomegalovirus), current or within the last 6 months. In addition, we investigated the relationship between slowness and the following neurological syndromes commonly associated with HIV infection: 1) neuropathy: includes history of numbness or burning sensations, with documented sensory and/or motor deficits in the neurological examination; DTRs could be diminished or absent, with or without trophic changes; 2) myopathy: includes a gradually progressive muscle weakness, symmetric and with a predominantly proximal pattern; DTRs could be diminished or absent; 3) encephalopathy: includes the presence of neurological signs indicative of generalized CNS involvement (such as release signs, abnormal cerebellar exam, generalized hyperreflexia, or extrapyramidal signs), with or without cognitive deficits. None of these patients exhibited HIV-myelopathy or HIV-associated inflammatory demyelinating polyradiculoneuropathy.
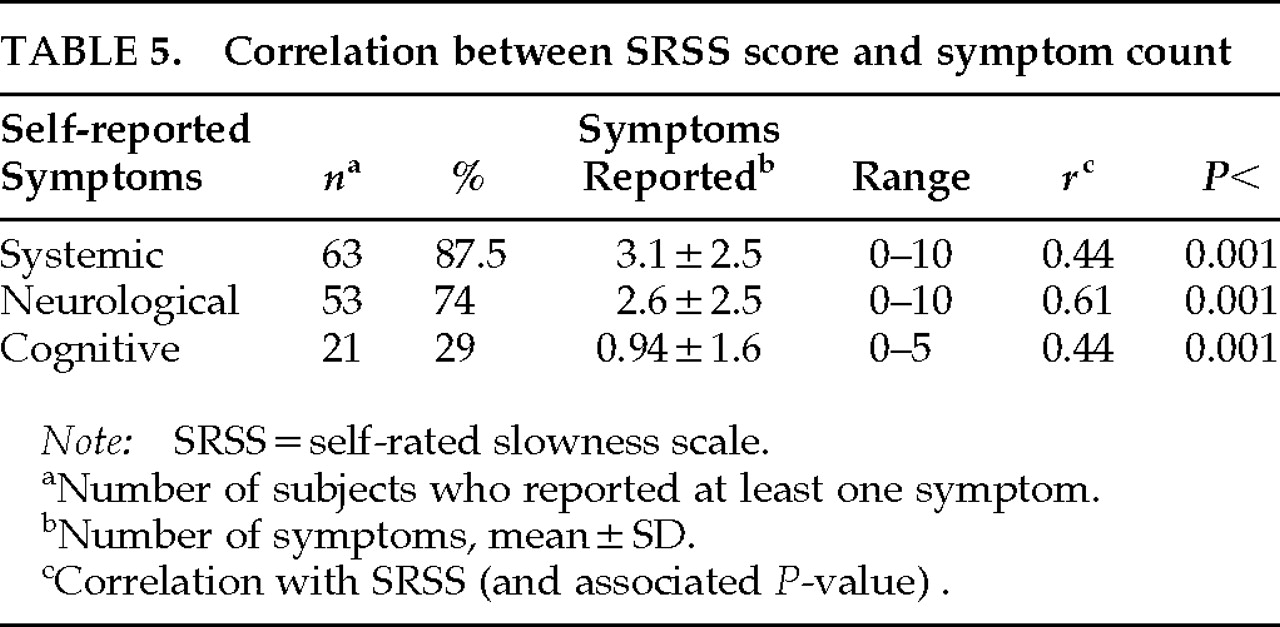
Self-reported symptoms, which were elicited by the examiner as part of the review of symptoms, included 1) medical symptoms: episodes of fever, night sweats, loss of weight, fatigue, oral/genital herpes, oral/esophageal candidiasis, diarrhea, frequent bruises, shortness of breath, and persistent coughing; 2) cognitive symptoms: memory deficits, word-finding difficulty, difficulty writing, reading, speaking, and doing mental calculations, episodes of disorientation, and impaired judgment; 3) neurological symptoms: episodes of syncope, hyper/hyposomnia, loss of libido, impotence, tinnitus, vertigo, dysphagia, dysarthria, dysphonia, disequilibrium, inability to walk/run, frequent falls, seizures, head trauma, blurred vision, diplopia, abnormal movements, and focal motor and sensory deficits. We calculated a total score indicating the total number of symptoms in each area.
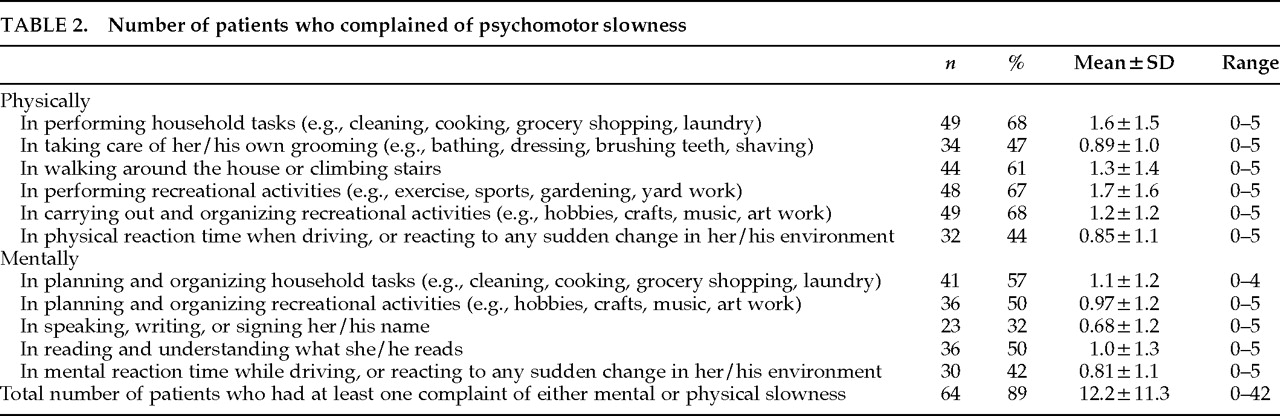
The subjects completed a self-rating slowness scale (SRSS) that included the most frequent activities of daily living.
37 The subjects were asked to rate the slowness of their own performance during the 6-month period prior to the study visit. The SRSS lists 11 common behaviors, 5 of which are focused on motor slowness and 6 on mental slowness. Each question was rated from 0 (normal) to 5 (extremely slow). The maximum possible score was 55, corresponding to the maximum severity of subjective slowness, and results are presented as an overall score. Content validity was evaluated with a principal component factor analysis in which two factors were extracted. The eigenvalues were 6.83 (62.1% variance) for the first factor and 1.06 (9.6% variance) for the second factor; a single-factor solution was thought to best account for the data. Details of the SRSS have been described elsewhere.
37DISCUSSION
In this study, we simultaneously examined the relationship of subjects' perceptions of their mental and motor slowness and the presence of HIV-related neurological and medical syndromes, mood-related disorders, neuropsychological features, and medication as well as complaints of neurological, cognitive, and systemic problems. By contrast, previous studies tended to focus on individual correlations between complaints of symptoms and either neurological, psychiatric, or cognitive manifestations of the HIV infection.
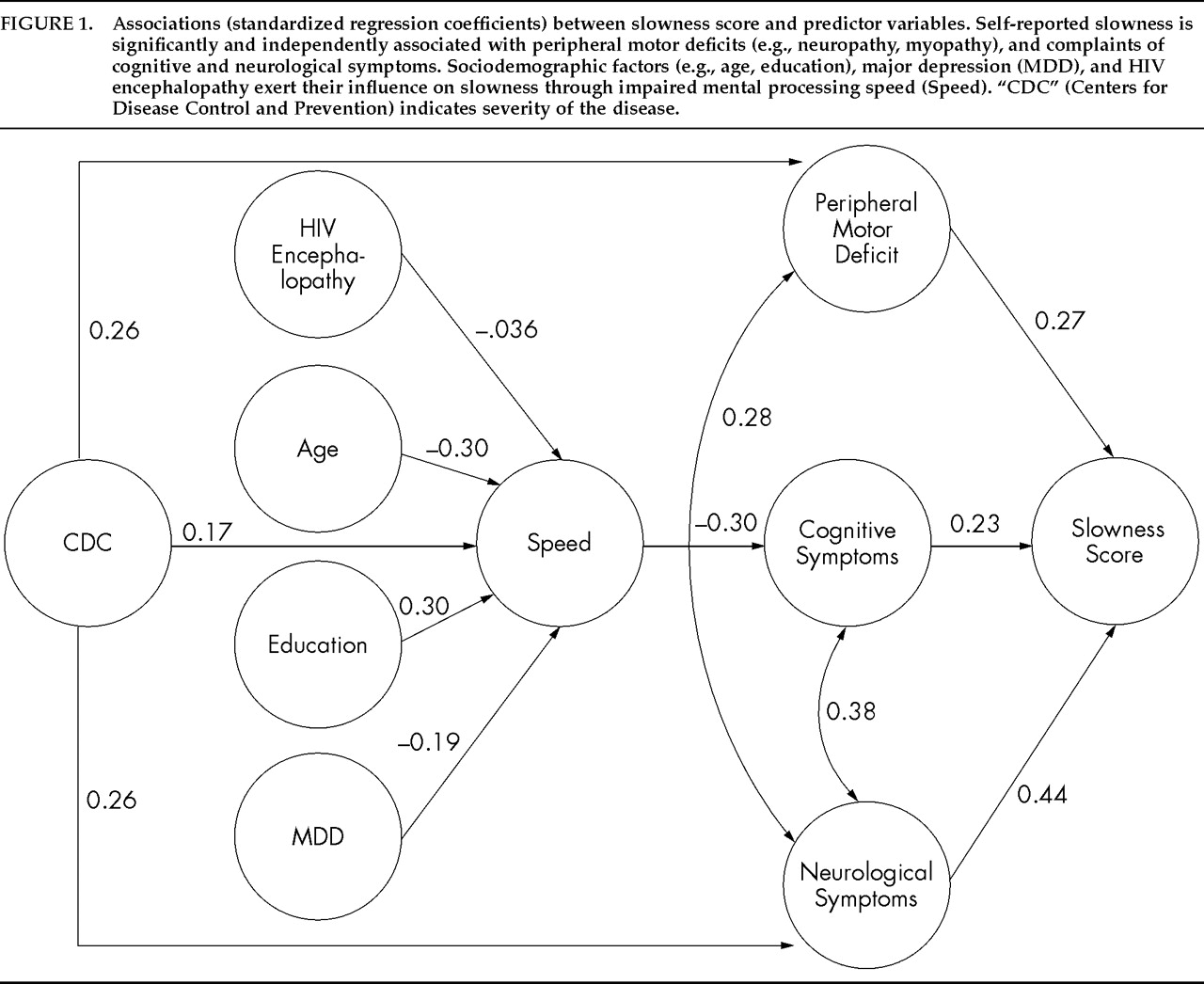
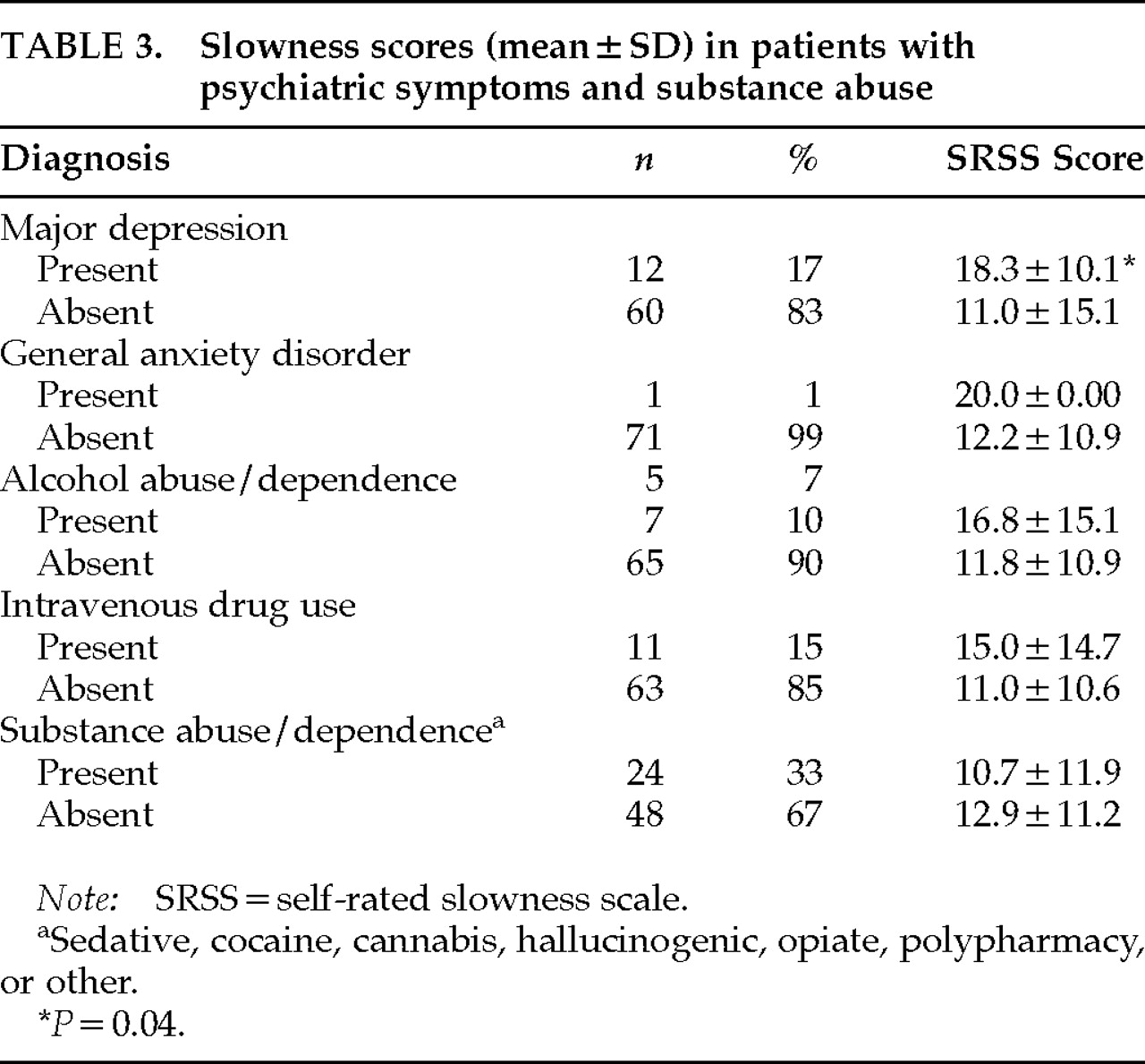
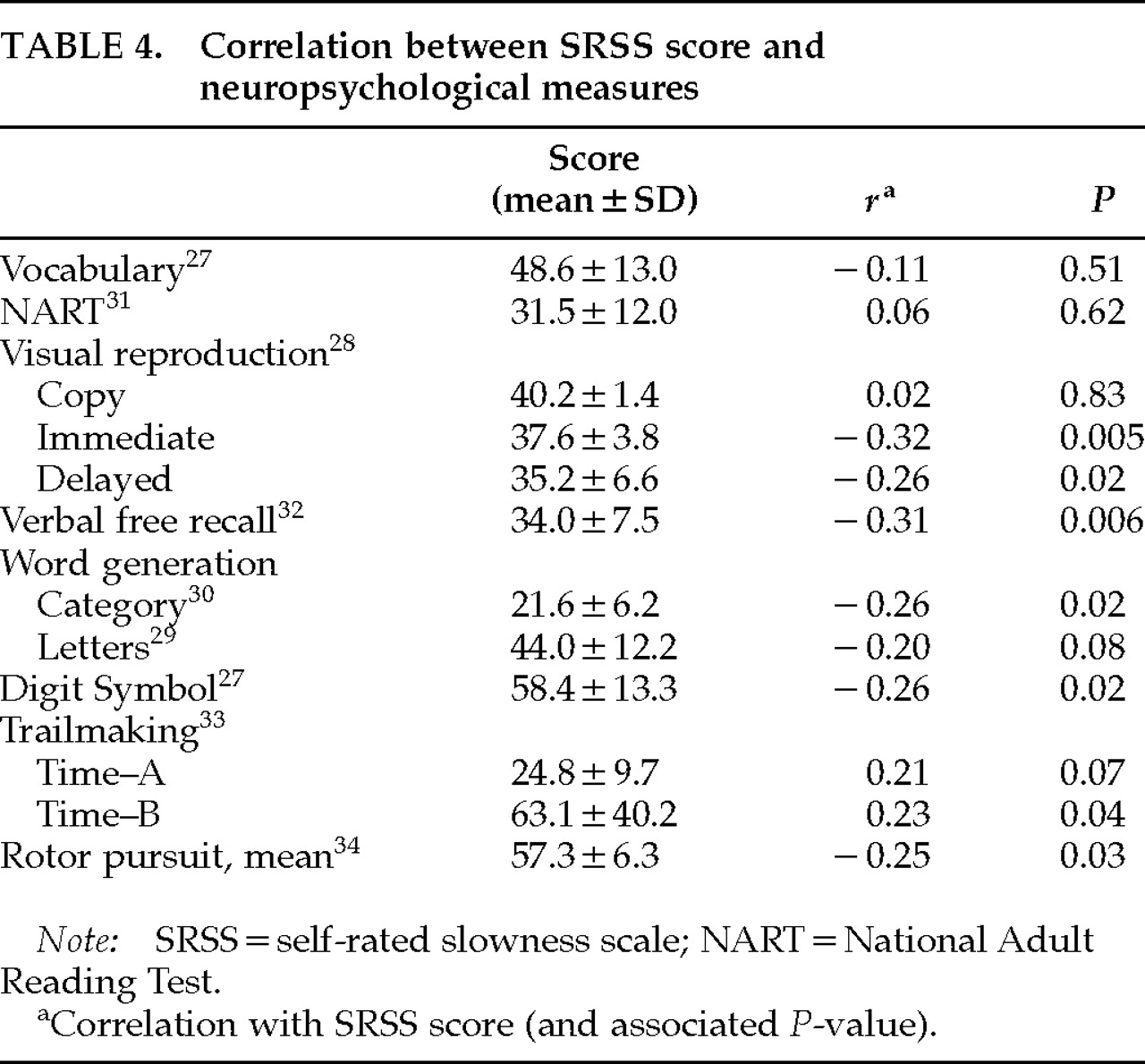
17–23 We found that SRSS scores correlated with severity of HIV infection, major depression, cognitive and neurological complaints, and measures of memory and information-processing speed. In addition, the SRSS score also correlated with neurological syndromes (myopathy, neuropathy, encephalopathy) and systemic syndromes (KS, wasting syndrome). Using this information, we examined the predictors of perceived slowness with a multiple regression analysis. Moreover, we developed an exploratory model to help us understand how these variables and the interrelationship among them may affect the subjects' complaints—specifically, complaints of perceived mental and motor slowness.
Two interrelated dimensions appear to affect SRSS scores. The first includes complaints of cognitive and neurological disturbances and peripheral neurological syndromes, where a close relationship exists between psychological symptoms and actual neurological symptomatology. The second includes variables that independently exert influence on the first dimension, such as age, education, severity of the disease, depression, and encephalopathy acting through mental processing speed. These findings suggest a close relationship between CNS involvement, disease severity, mood-related disorders, sociodemographic factors, and complaints in general, especially those of psychomotor retardation.
When HIV+ patients report specific cognitive deficits, this may more accurately reflect overall slowed processing speed. Mapou et al.
20 reported that HIV+ patients who complained of language difficulties actually manifested deficits in simple reaction time tasks rather than in language functions. Moreover, in a separate study, we found that impaired mental processing speed was an independent predictor of frontal, memory, verbal fluency, and spatial performance scores.
24 It thus appears that reports of mental slowness reflect slowed psychomotor speed and that this in turn has its effect on other aspects of cognition.
The neuropsychological assessment had two limitations. First, in order to present a homogeneous cognitive battery, we limited the number of tests, although they covered the most relevant HIV cognitive manifestations. Second, a group of patients had the SRSS and cognitive testing at follow-up examination; therefore, a learning effect of neuropsychological information may have influenced these patients' performance. However, the SRSS scores correlated with wordlist learning and nonverbal memory and with measures that had large information processing speed components (word generation, Digit Symbol, and Trail Making Test). This pattern is consistent with the idea that frontal-subcortical system dysfunction is a core phenomenology of psychomotor slowness in HIV.
6–10 A similar pattern of memory and slow mentation has been reported in PD patients with bradyphrenia, who are more impaired on memory, reaction time, and continuous performance tests than are PD patients without bradyphrenia.
14The presence of peripheral neurological deficits was a significant predictor of self-reported psychomotor retardation. Motor complaints correlate with measures of fine motor control, and HIV+ patients with motor complaints are neuropsychologically worse than those without complaints.
18 Psychomotor retardation, as measured by complaints of symptoms or by actual neuropsychological testing, appears to be involved in the whole spectrum of the neuropsychiatric manifestation of the disease, especially as the infection becomes more severe.
The relationship between slowness and depression appears to be attenuated when other cognitive, neurological, and medical signs and symptoms are taken into account in HIV+ individuals. As noted in our model, although depression can contribute to the feelings of slowness, it appears to exert its major influence through the effect that mood-related disorders have on cognitive function. Indeed, Perkins et al.
21 found that complaints of fatigue and motor slowing, as symptoms of major depression in asymptomatic HIV+ patients, were independent of dysphoric mood and other symptoms of major depression.
Our findings indicate the importance of complaints of psychomotor slowness in HIV and the need to further examine their presence in larger HIV cohorts. They are associated with severity of the disease, and they occur in the context of specific HIV-related neuropsychiatric symptomatology, including major depression, peripheral neurological deficits, and cognitive impairment.