The following case report describes the natural history, clinical evolution, and possible functional cortical involvement of a subcortical abnormality.
Case Report
A 16-year-old right-handed girl presented with typical early schizophrenic symptomatology of 12 months' duration. Her main symptoms consisted of
athymhormia, a syndrome recognized in France that is characterized by a loss of drive and affective responsiveness. She was treated with individual psychoanalytical psychodrama for a year before she had to be admitted to an adult psychiatric ward. The diagnosis of schizophrenia was confirmed, and she was treated with neuroleptics. This reduced her high levels of anxiety and controlled her hallucinatory symptomatology. The results of initial structural
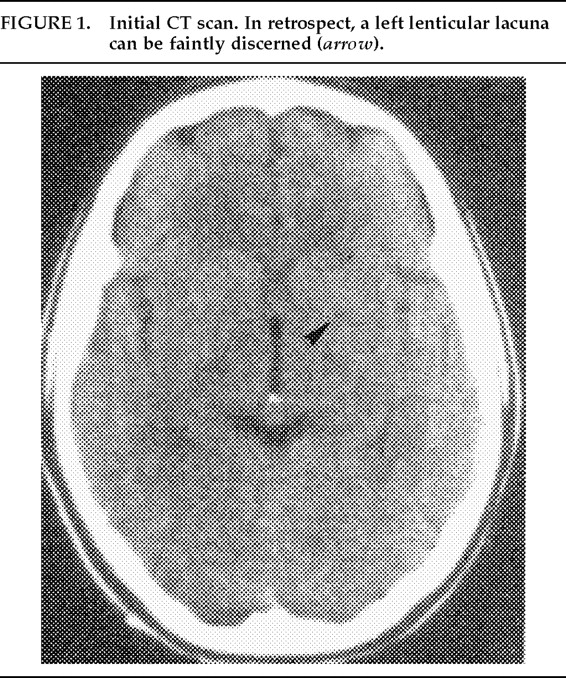
(Figure 1) and functional imaging studies were reported as normal.
Between the ages of 17 and 23 the patient attended a day hospital. At the age of 24 she was rehospitalized because of a progressive deterioration of her condition, manifested in violent behavior toward her parents, dramatic reduction of speech, prominent auditory hallucinations, incongruous laughter, and autistic withdrawal.
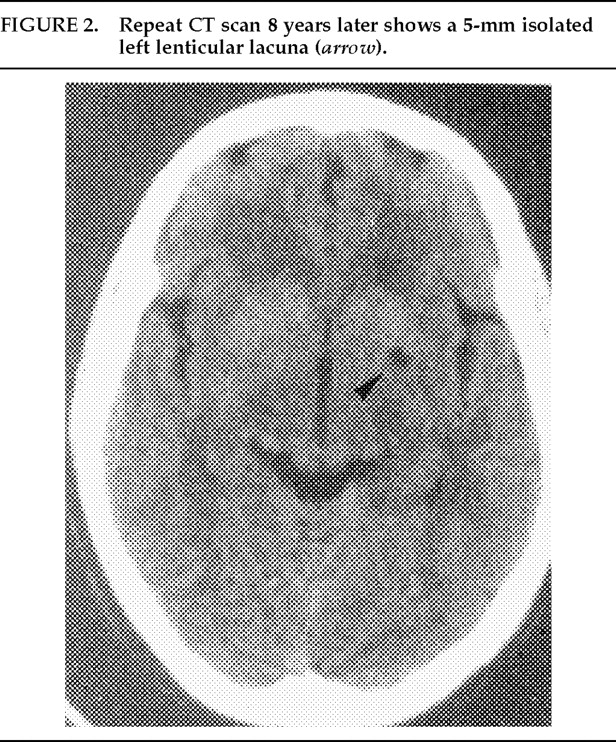
A repeat of the previous imaging studies revealed, on CT scan
(Figure 2), a 5-mm isolated left lenticular lacuna, which on MRI scan was located at the inferoposterior putamen. Isodense relative to the CFS in a young patient without vascular risk factors or a history of cardiac embolism, it was deemed a type III lacuna resulting from a dilatation of the perivascular (Virchow-Robin) space.
1 In retrospect, it could be faintly discerned on the first CT scan and therefore appeared to be evolving. We hypothesize that the major cortical hypoperfusion demonstrated on the second SPECT scan was the result of diaschisis or deafferentation, a depressive metabolic effect exerted on an intact brain region by a distant primary lesion.
2,3 This seems particularly plausible in view of the predominantly left ipsilateral cortical hypoperfusion.
However, the question remains whether the lacuna is of pathological significance. Such isolated lesions are sometimes discovered accidentally and without any clinical manifestations in elderly subjects, and the cortical hypoperfusion could represent a correlate of the patient's psychotic state.
Alternatively, a case could be made for an etiological link between the parallel evolution of the imaged lesion and the patient's clinical condition. The lacuna is situated in a region that has previously been implicated in the pathogenesis of schizophrenia.
4 In addition, athymhormia has been observed after acquired basal ganglia lesions.
5To conclude, early and repeated structural and functional cerebral imaging studies identified an isolated and evolving lacuna of the left putamen in a case of severe, progressive schizophrenia. Although its origin remains unknown, its pathological significance seems probable. Similar findings may confirm the etiological importance of certain strategically located microlesions in the origin of some psychotic disorders.
We thank Professors Derouesné and Poirier for their expert opinions on this case.