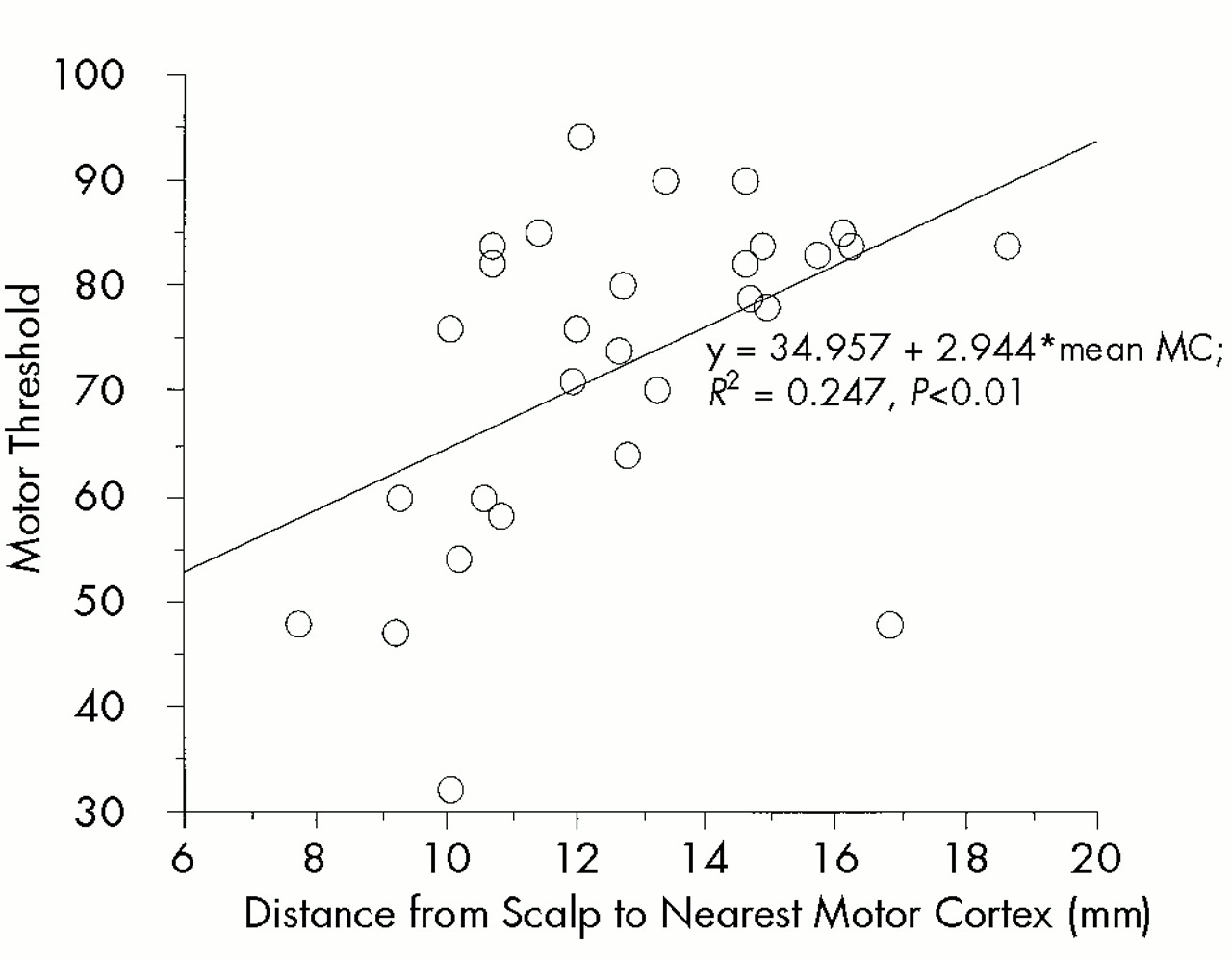
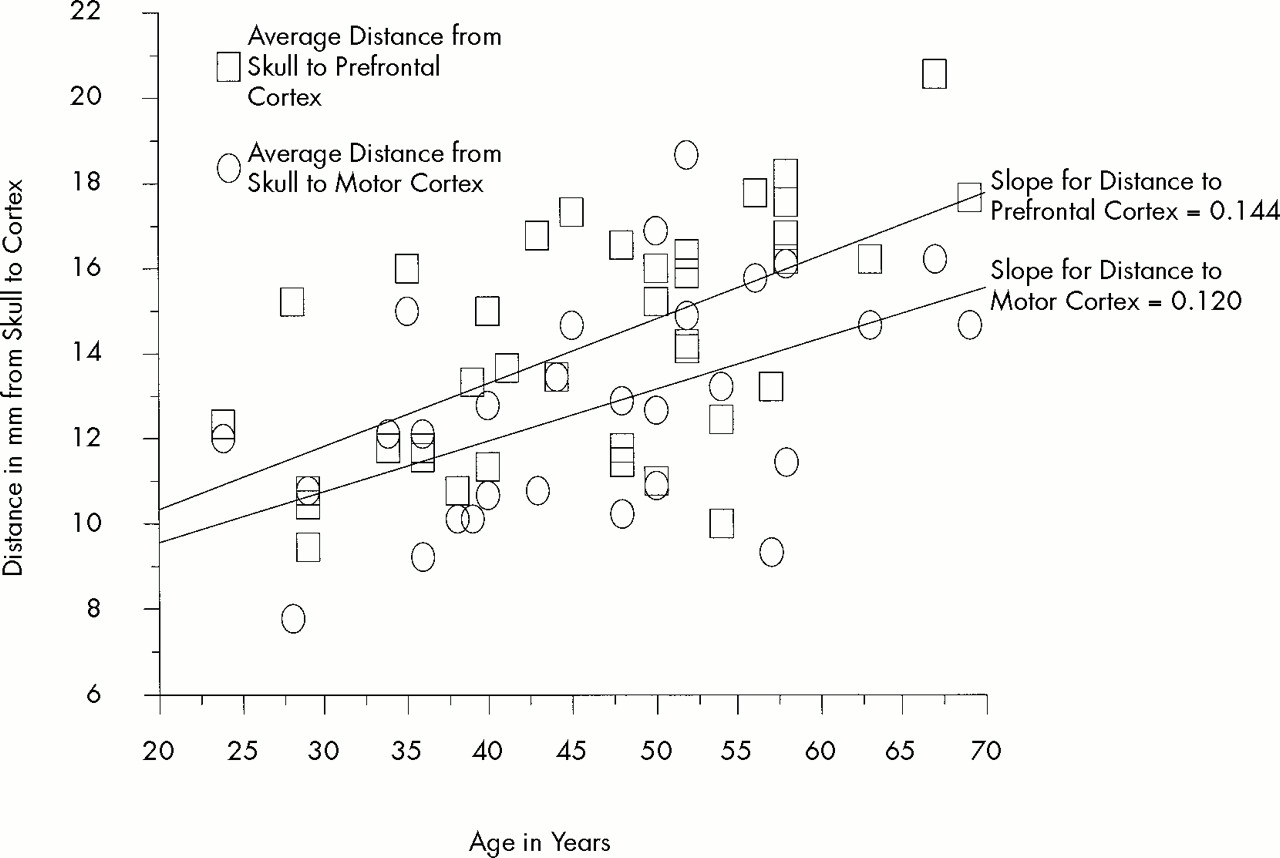
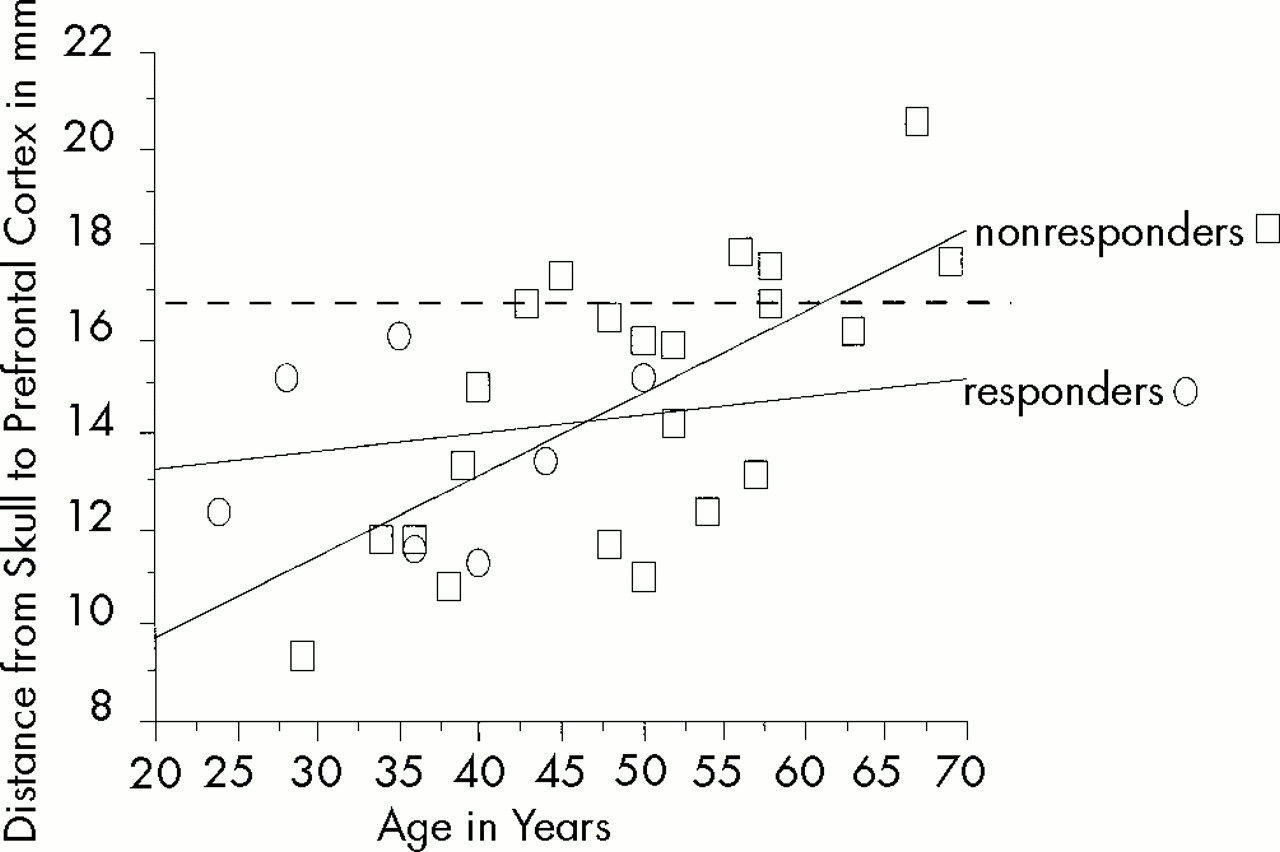
This is the first study addressing the complicated area of whether and to what degree the distance from coil to motor or prefrontal cortex interacts with motor threshold. This study also examines the relationships between age, prefrontal cortex distance, and clinical antidepressant response. As the first study exploring these questions, it suffers from several methodological shortcomings outlined below. Nevertheless, there were several important findings. The estimated distance from TMS coil to prefrontal cortex (D-PFC) was greater than the distance from coil to motor cortex (D-MC). The motor threshold (MT) significantly correlated with D-MC, whereas it did not correlate with D-PFC. Both motor and prefrontal cortex distances increased with age in this depressed cohort, with D-PFC showing a trend to increase at a faster rate than D-MC. Finally, there was not a linear correlation between D-PFC and clinical antidepressant response. All subjects however, who responded were below a critical threshold of age and prefrontal cortex distance.
Limitations of the Study
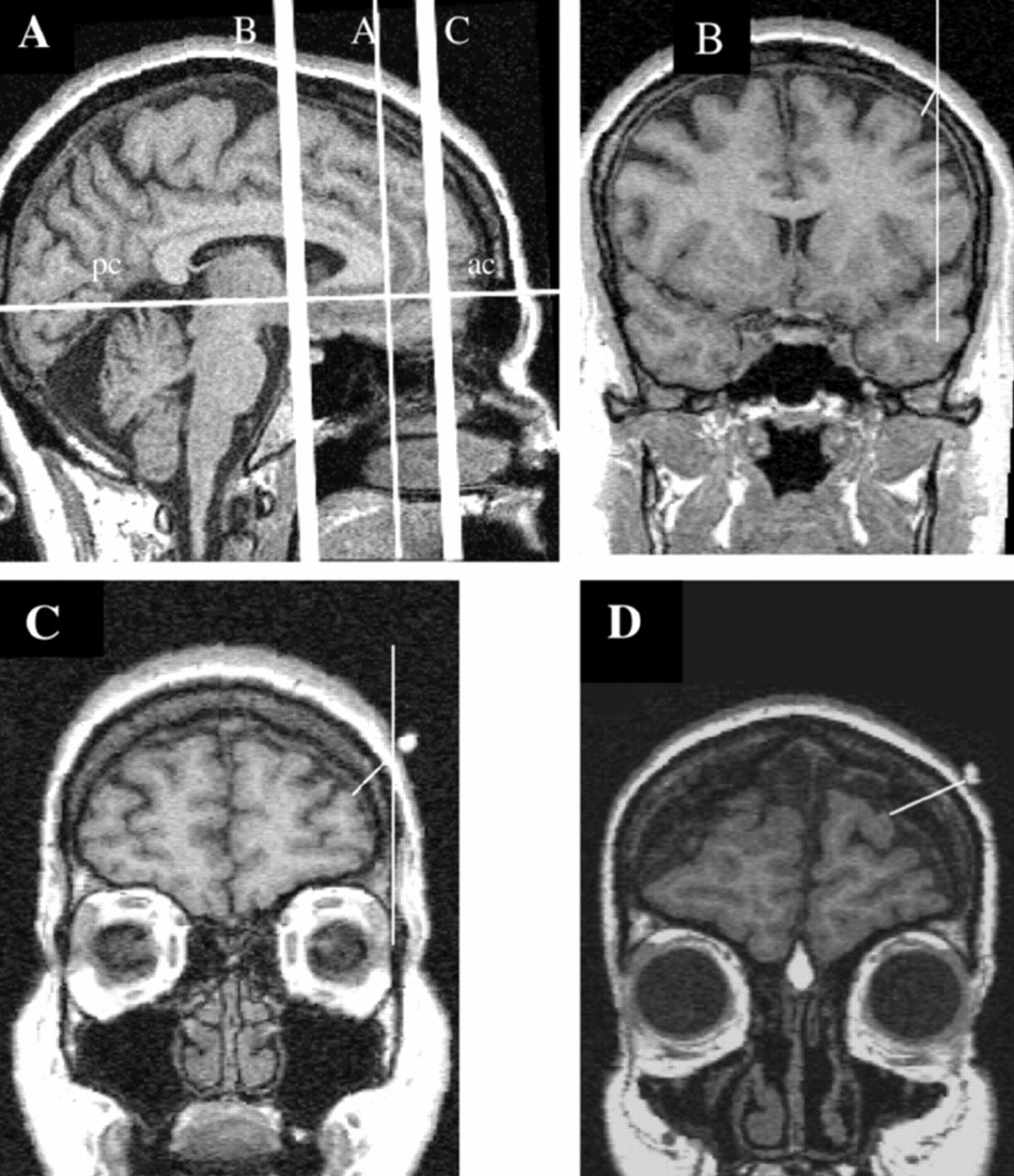
There are several limitations of this study that bear on proper interpretation. The most important of these was difficulty in determining the TMS sites on the MRI scans. One method used was to place a fiducial at the site of the rTMS. When designing the study, we reasoned that this fiducial would enable a relatively precise localization of the actual site of stimulation. Using this method alone, however, would have limited an already small sample size, because only about three-fifths of the subjects studied and scanned had fiducials that could be seen on the MRI scan. Complicating things further, during scanning several of the fiducials appeared to have moved off of the scalp, resulting in a placement that no longer represented the true site of rTMS. Because of these confounding factors, we felt that using the actual fiducial to measure the distance to nearest cortex in this study was not an accurate method.
While trying to develop a more accurate method, we noticed that the prefrontal fiducial was often directly in line with a vertical (–90 degree) line from the lateral center point of the left eye. We found that the fiducial was commonly 20 slices anterior from the corpus callosum and therefore adopted this as the “virtual” location of the rTMS coil to start measuring the eight scans. By performing the measurement 4 mm in front of and behind this chosen intersection, we averaged the scalp to cortex distance over the likely prefrontal spot. Thus, even if we did not measure directly under the actual TMS spot, we were able to obtain a distance measurement that likely represented the average distance of skull to cortex in this region. Further, this averaging system of a virtual spot enabled us to utilize all of the scans available for analysis, and the technique often correlated well with the position of the fiducial. The limitation was that we could not be sure how close to the actual coil stimulation the measurements were performed. Despite these difficulties, the standardized method of measuring eight scans and averaging the result does appear to give a rough approximation of the distance to the nearest cortex in the area stimulated. This corresponds to either the left medial frontal gyrus or the left superior frontal gyrus (Talairach coordinates:
x plane from –25 to –40,
y from 50 to 58,
z from 20 to 40). Future studies with more precise fiducial placement, or even MRI phase maps of the actual magnetic field
3 in all subjects, would improve on the current study.
Similarly, there was no fiducial over the motor cortex APB area where MT was actually determined. Thus, we were forced to empirically determine this spot as well by measuring backward from the prefrontal site. We again measured the motor cortex distance over a relatively large area (8 mm) in order to compensate for the imprecision of our location. Because we measured motor cortex distance on 8 slices, the number used as a dependent variable is thus more likely a rough measure of motor cortex atrophy, rather than the exact distance from coil to motor cortex.
Despite all these factors, the robust correlation of motor threshold with distance to motor cortex is surprising, especially given these limitations in spatial location. Future studies with fiducials directly over the true site of optimum APB stimulation are needed.
The motor threshold was determined in this study by using visible movement, which is not standard practice but which our group has shown on a different machine to correspond to MT determined by motor evoked potentials.
13 Future studies exploring these issues might use electrophysiologically determined MT. Similarly, our choice of the percentage change in Ham-D as the dependent variable for clinical response is relatively imprecise, but a standard practice. Future studies using other behavioral, neuroendocrine, or even brain metabolism measures might better address the correlation between distance and clinical response. Finally, the small sample size could have reduced the power of the study such that the relationship between distance to the cortex and percentage response was not statistically significant. Our sample was especially small at the extremes of age (5 subjects>55 years old) and distance to the prefrontal cortex (3 subjects>17 mm). On a more theoretical note, the magnetic field declines logarithmically with distance, and we tested for correlations that assumed linear relationships. Future studies with larger samples might explore whether nonlinear relationships exist between the distance variables and the other factors examined in this study. Despite these important limitations, these data provide intriguing results that will require further investigation combining rTMS and imaging.