The functional anatomy of the brain, especially of the subcortical structures, is one of the least understood areas in medical science. Although there has been much debate over the years regarding the need for clinical imaging of patients with psychiatric symptoms, much of our understanding of functional anatomy is derived from study of patients whose brains have been damaged by injury or illness. This approach has been more fruitful in illuminating the functions of cortical areas rather than subcortical. The limited functional information regarding subcortical nuclei is due to the relatively small size of most subcortical nuclei and the density of adjacent tracts. Most injuries affect more than one subcortical structure. The exceptions to this are the disease and injury processes that target very specific brain areas.
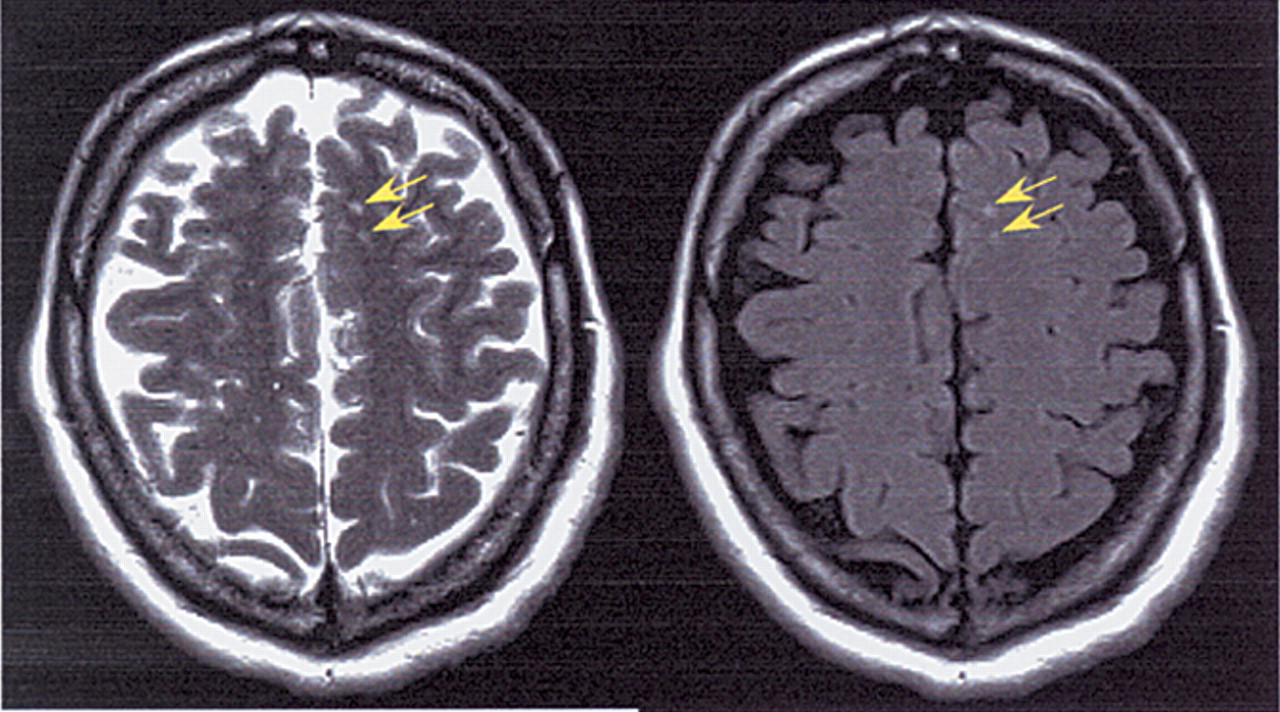
Carbon monoxide (CO) poisoning, with its traditional symptom clusters and classic predilection for the basal ganglia and subcortical white matter, provides insight into the functional anatomy of this complex area. Patients who survive the initial CO poisoning provide a population in which imaging findings can be studied in relation to clinical symptoms. This is particularly valuable in view of the continuing controversy over the significance of small areas of abnormality on images, particularly areas of hyperintense signal on T
2-weighted magnetic resonance (MR) images (see
Figure 1).
Carbon monoxide is a colorless, odorless gas produced as a byproduct of combustion. Poisoning usually occurs from exposure to automobile engine exhaust, cigarette smoking, furnaces, or other unvented gas exhausts. Carbon monoxide is the major cause of poisoning deaths (accidental and deliberate) in the United States and Europe, with more cases occurring during the winter months.
1,2 Although estimates vary, in the United States 2,000 to 6,000 deaths and 40,000 emergency room visits occur each year from CO poisoning.
1As with most types of poisoning, outcome depends on the length and intensity of exposure. Commonly, initial symptoms include severe headache, nausea, weakness, confusion, arrhythmias, metabolic acidosis, coma, or death.
3,4 If the patient survives the initial insult, 2% to 40% will develop a delayed or interval CO encephalopathy 2 to 40 days later. The most commonly reported sequelae include parkinsonism; dystonias or other motor impairments; cognitive or executive function deficits; akinetic mutism; mood disorders (including depression, anxiety, and emotional lability); memory deficits; and personality changes.
5–8Recovery varies; most patients achieve at least partial recovery within 6 months to one year. However, studies examining neuropsychological functioning have been limited.
1,7,8 Recent studies using more detailed neuropsychological assessment indicate that subtle but significant decrements in cognitive performance may be common even years after recovery from the major symptoms.
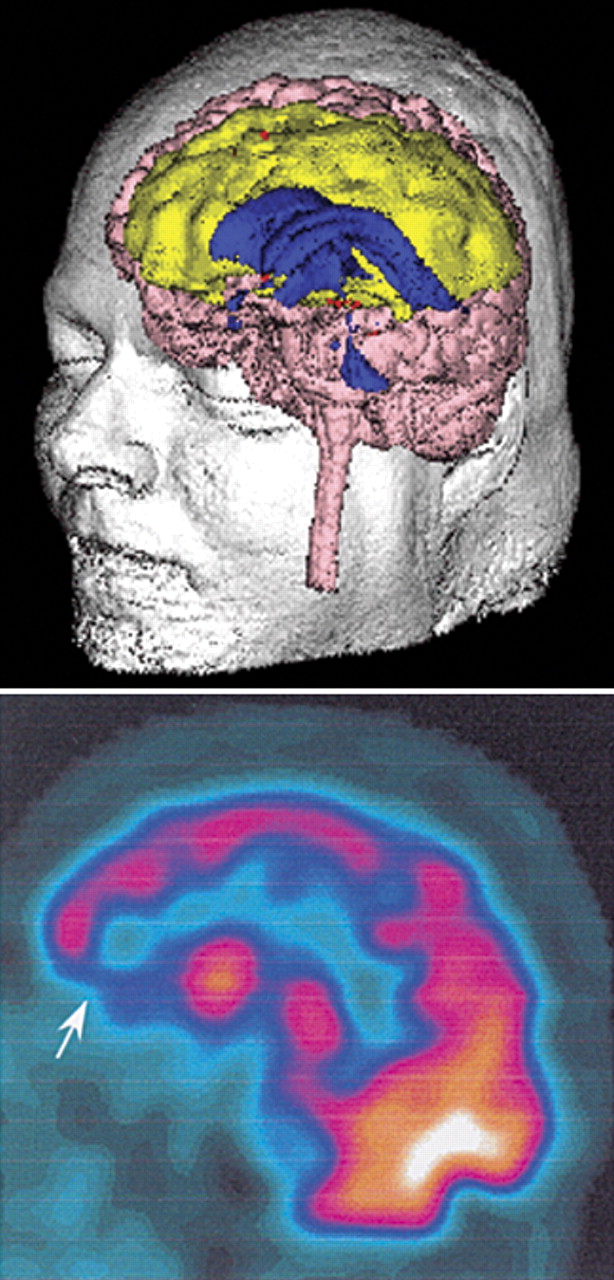
1,7 Thus, while these individuals may appear normal and may have returned to independent living, some are functioning at a clearly diminished level. One study reported a significant correlation between neuropsychological impairments and abnormalities in cerebral perfusion, clinical MR, and/or brain volumetric measures (see Cover and
Figure 2).
1 Prospective studies from the same group suggest that specific atrophic changes in white matter structures may correlate with some cognitive impairments at 6 months post CO exposure.
9,10Clinicians generally have examined carboxyhemoglobin (COHb) levels for guidance on acute treatment and for prediction of long-term deficits. Recent work has shown that COHb levels do not correlate with clinical symptoms but can be helpful in guiding initial emergent care (i.e., the need for hyperbaric oxygen versus 100% oxygen at ambient pressure).
2,4For a fuller appreciation of the imaging findings in CO poisoning, a brief review of pathophysiology is helpful.
11 Carbon monoxide poisoning causes profound tissue hypoxia by both direct and indirect mechanisms. It competitively binds to hemoglobin, replacing oxygen, forming COHb. Although CO binds more slowly than oxygen, the binding is estimated to be more than 200 times stronger. As CO replaces oxygen on hemoglobin, less oxygen is available for transport to tissue. The bound CO also increases the stability of the oxyhemoglobin complex (shifts the oxygen dissociation curve to the left), allowing the hemoglobin to release less of the bound oxygen it carries to tissues. In addition, the stability of the COHb complex results in CO remaining bound to hemoglobin, reducing the amount of hemoglobin that is free to pick up carbon dioxide (CO
2) from tissue. As a result, the CO
2 concentration of the blood is lowered. The low blood CO
2 decreases the direct stimulation of the respiratory centers and thus lowers the respiratory rate. Although delivery of oxygen to tissue is low, the carotid sinus is not stimulated, since the oxygen partial pressure in the blood is normal. Carbon monoxide also combines with cytochromes and myoglobin. It inhibits cellular actions such as mitochondrial metabolism and promotes production of free radicals.
4 It may be the combination of these mechanisms that leads to the brain injury from CO poisoning.
12The brain and heart are particularly vulnerable to the destructive forces of this poison. The myocardium binds CO more strongly than skeletal muscle, leading to noticeable oxygen deprivation and symptoms of angina, arrhythmias, and markers of cellular death. If the patient survives the initial insult, demyelination of subcortical white matter and necrosis of the basal ganglia are common. In part, this may be because these areas have limited vascularity and a “watershed” blood supply. Cortical, hippocampal, and cerebellar insult occur with more extensive exposures.
For many years, MR and computed tomographic (CT) imaging have been performed in patients with CO poisoning. The findings generally have been reported in limited numbers or as single case reports, owing to the small number of poisoning cases that will come into a single emergency room or academic institution. Recently, the focus has shifted from simply reporting findings to examining their use as predictors of outcome, an important advance in understanding the functional role(s) of the basal ganglia. Imaging studies have been done both acutely and during later stages, when delayed parkinsonian and other symptoms are expected. The recent addition of methods more sensitive to brain function (i.e., imaging of cerebral blood flow and cerebral metabolism) may also provide valuable prognostic information.
Two recent studies present sufficient cases to assess the frequency of visualizing different types of brain injury during the first week after CO poisoning.
2,13 Although the imaging techniques used (MR, CT) provide quite different levels of anatomic detail, the results were rather similar. In both reports, slightly more than one-third of patients had normal imaging studies. The globus pallidus was the most frequently injured area (39%–63%), followed by the deep subcortical white matter (28%–32%). Cortical, mesial temporal lobe, and other subcortical lesions were occasionally seen.
Patients without imaging abnormalities had a favorable prognosis in both of these studies. In contrast, Lee and Marsden
14 did not find a better prognosis in patients with normal initial CT scans who were symptomatic in the first week. In general, the literature indicates that patients with more areas of injury have a poorer clinical course and are more likely to have significant neuropsychiatric abnormalities later. However, like the level of COHb in the blood and the initial duration of impaired consciousness, the results of imaging in the acute stage are not presently reliable predictors of outcome. This situation may change as MR techniques that are more sensitive to white matter damage come into clinical use. Murata et al.
15 reported a case in which standard clinical MR images (i.e., T
1- and T
2-weighted images) appeared normal at the same time that abnormalities were clearly present in the white matter on fluid-attenuated inversion recovery (FLAIR) images (see
Figure 1). In the future, correlations between initial imaging abnormalities and outcome may improve.
Measures of cerebral blood flow, using positron emission tomography (PET), single-photon emission computed tomography (SPECT), or xenon-enhanced CT (Xe-CT), may be more immediately useful in estimating prognosis during the acute stage. Several recent studies, using modern scanners that allow visualization of subcortical as well as cortical blood flow, have shown that regional cerebral blood flow abnormalities may be present in the absence of abnormality on CT or MR.
16–18 In one study, cerebral blood flow abnormalities related to CO poisoning were present in 2 patients who had bad outcomes (death, long-term memory impairment), but not in 1 patient who recovered fully.
12 Two of these patients were studied the day of admission, the other patient 4 days after admission. Kao et al.,
17 who measured cerebral blood flow within a few hours of admission, also found that their 2 patients with normal cerebral blood flow had a good recovery. In contrast, Sesay et al.
16 did not find cerebral blood flow measurements taken 3 to 5 days after insult to be predictive of outcome.
One study indicates that there may be a good correlation between the areas that are hypoperfused during the acute stage and the neuropsychiatric symptoms that develop later.
17 Parkinsonian symptoms developed only in the patients with decreased perfusion of the basal ganglia. Cognitive deficits (confusion, disorientation, memory deficits) developed in patients with decreased cerebral blood flow in cortical areas.
As noted earlier, there can be delayed development of symptoms after a period of apparent recovery (the interval or delayed form). The most common locations of imaging abnormality may be different in this later stage. Some studies have found more lesions in the white matter (58%–64%) than in the globus pallidus (9%–26%), whereas others have found an equal incidence.
5,8,14Magnetic resonance and CT studies done when these delayed symptoms appear indicate that there is not a clear correlation between symptoms and imaging abnormalities. Pavese et al.
5 found that at 1 month post CO poisoning, 50% of patients (11/22) had abnormalities on MR, but only 27% were symptomatic. All patients with normal MR were asymptomatic at 1 month, although 1 patient with a normal and 1 with an abnormal MR study became symptomatic later. Other authors have reported that many patients with delayed symptoms (30%–42%) have normal imaging examinations.
8,14As in the acute stage, measures of cerebral blood flow may be more sensitive to CO poisoning–related delayed changes than is standard diagnostic imaging (see
Figure 2). A recent SPECT study found patchy hypoperfusion in all patients (13/ 13) examined after appearance of delayed symptoms.
8 Four of these patients had normal CT scans. Follow-up studies were obtained in one-half of the group. Cerebral blood flow improved in the 6 patients showing clinical improvement and was unchanged in the 1 patient who did not recover. Similarly, another study (using SPECT and Xe-CT) reported 3 patients in whom delayed clinical deterioration correlated with decreased cerebral blood flow.
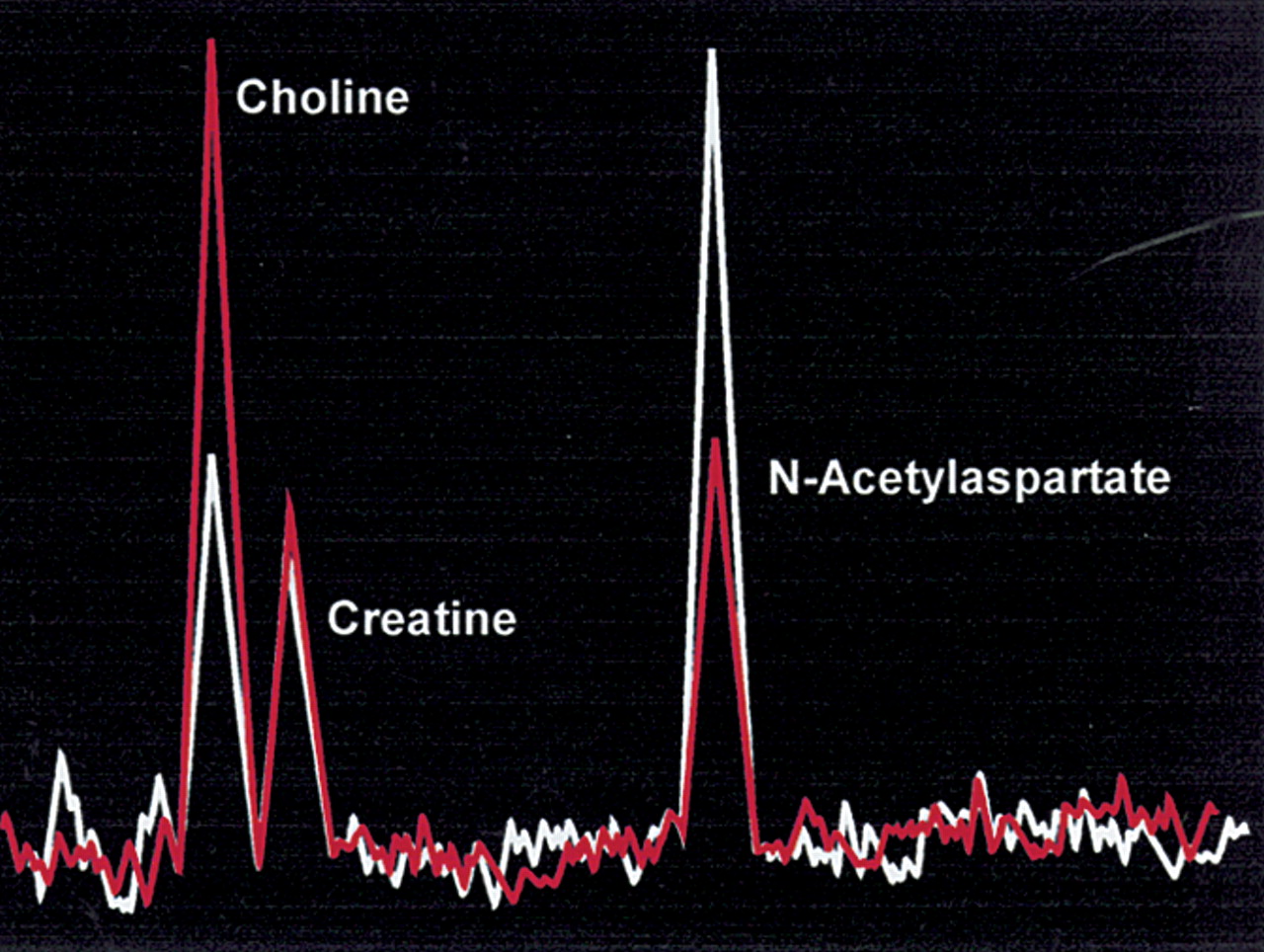
16Another method that may be quite sensitive to the pathophysiology underlying the development of delayed symptoms is magnetic resonance spectroscopy (MRS). In MRS, signal is obtained from metabolites that are present in very low concentrations (as opposed to MR imaging, in which most of the signal comes from water). The low amount of signal available demands acquisition from a relatively large volume (voxel). The signal is usually displayed as the spectrum of the amount of signal produced by each metabolite. In proton MRS of brain, signal is present from N-acetylaspartate (NAA, located primarily in neurons, a marker for neurons and axons), choline (Cho, principally phosphatidyl choline, a membrane constituent), and creatine (Cr, used as an internal standard because its level is usually stable). If an area is severely injured, there may also be a lactate peak. The absolute amount of signal in each spectral peak is highly dependent on the acquisition parameters, so for comparison purposes the signals of interest (NAA, Cho) are expressed relative to Cr. The Cho/Cr peak reflects membrane metabolism and has been found to be elevated both during degradation (demyelination) and rapid synthesis. The NAA/Cr peak reflects neuronal and axonal density.
Several small studies have found proton MRS to be quite sensitive to CO poisoning–related changes in white matter (see
Figure 3).
19–21 In one patient, for example, NAA/Cr was below normal and Cho/Cr was elevated at the time of delayed onset of symptoms (which included bizarre behavior, urinary and fecal incontinence, and gait apraxia), yet both MR and cerebral blood flow measures were normal.
19 Abnormalities were visualized later on MR, while the patient was still fully symptomatic. Cerebral blood flow measures were always normal. The MRS changes persisted for some time, returning toward normal in parallel with clinical recovery. In another study, spectral changes at delayed symptom onset were more severe in the patient who developed the more profound clinical symptoms. The two patients had similar levels of abnormality on MR imaging. Clinical recovery correlated with normalization of the spectra in both patients.
21 Thus, proton MRS may provide a much-needed measure of injury severity following CO exposure.
Although the common wisdom has been that most people who survive the initial insult will recover from CO poisoning within a year, recent studies have suggested long-lasting, perhaps permanent, more subtle impairments may occur rather frequently. Careful study of patients with only white matter lesions or only basal ganglia injury could shed valuable light on the functional significance of these areas as well as identify the best imaging techniques to discern injury both in the acute and delayed settings. Additionally, identification of neuropsychological deficits that may benefit from therapy or explain a downdrift in cerebral functioning can be invaluable.