The Spectrum of Organic Depersonalization: A Review Plus Four New Cases
Abstract
METHODS
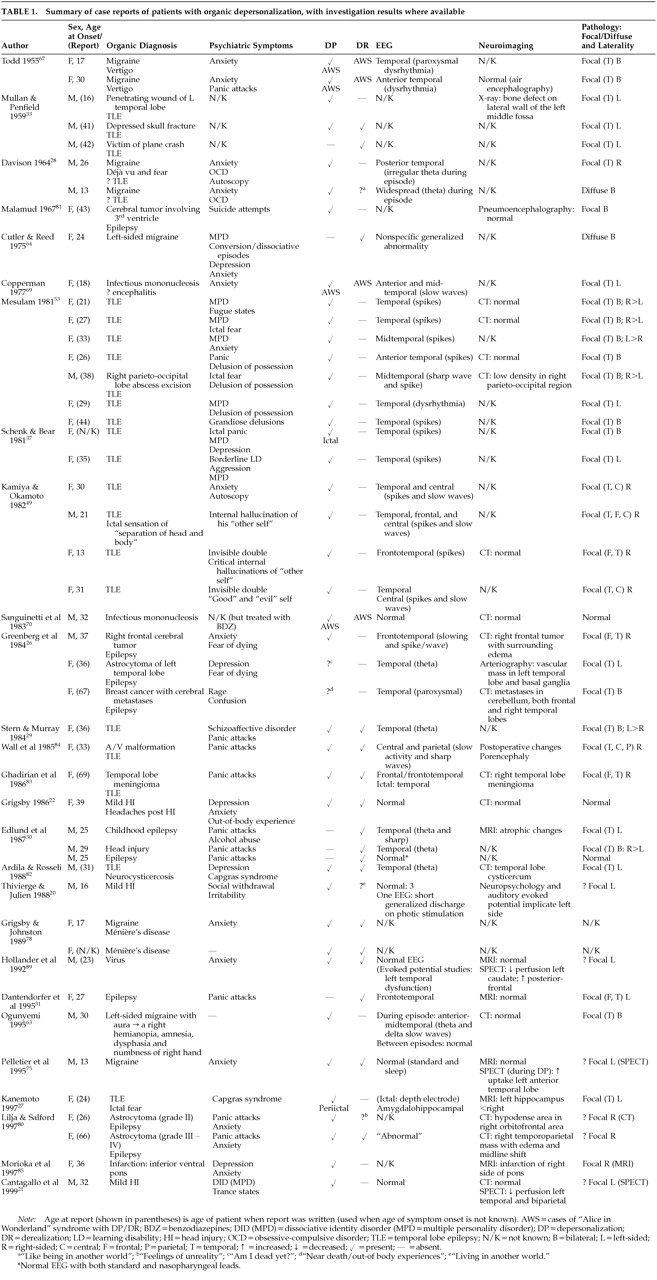
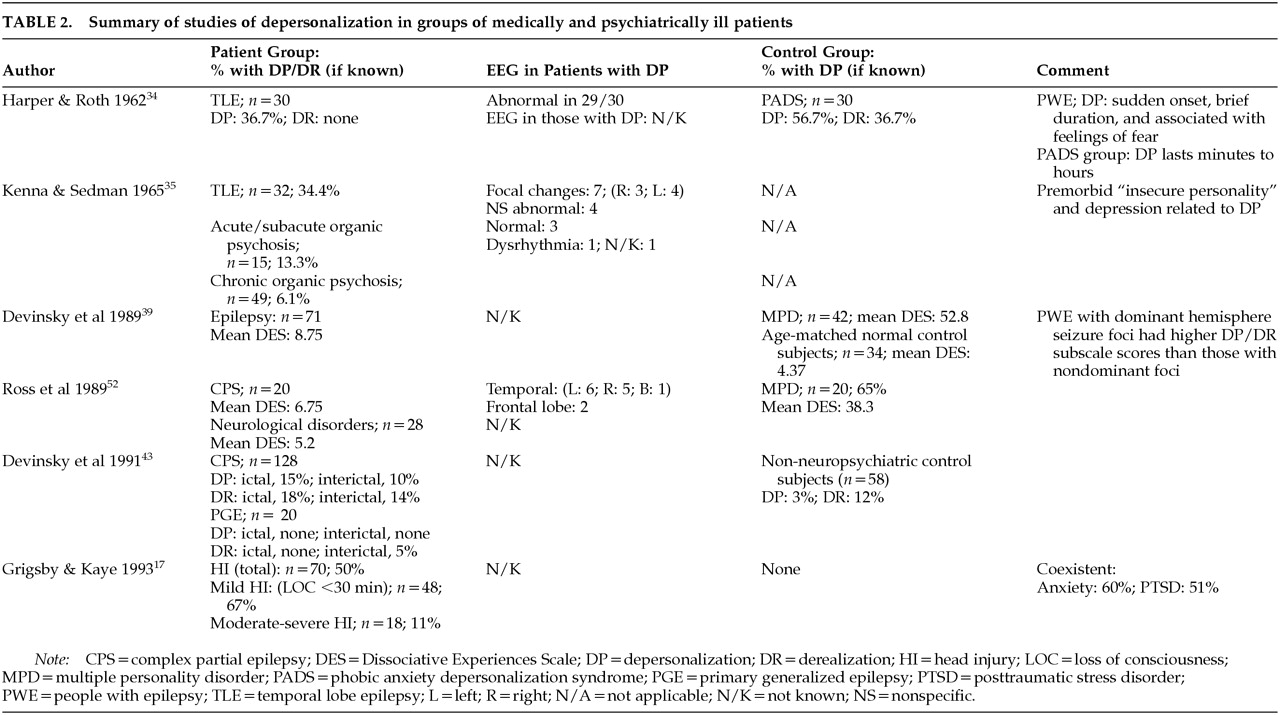
LITERATURE REVIEW
RESULTS
Traumatic Brain Injury (TBI)
Epilepsy
Case Reports:
Case Series:
Stimulation Studies:
Migraine
Vertigo
Cerebral Tumors and Cerebrovascular Disease
NEW CASE HISTORIES
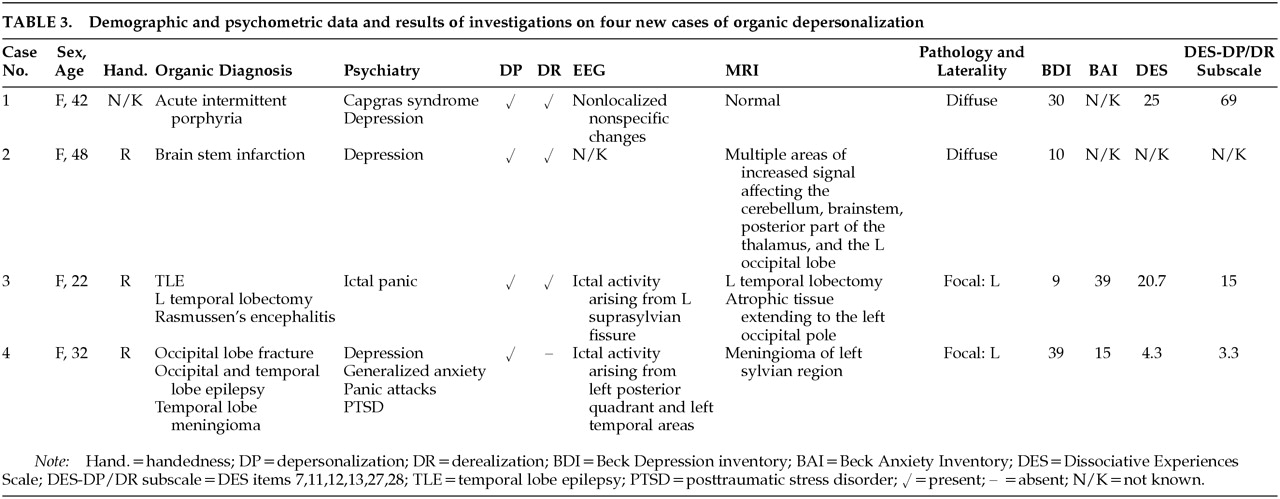
Case 1. A 42-year-old woman with no personal or family history of any neuropsychiatric disorder was diagnosed with acute intermittent porphyria at the age of 39. Her attacks tended to occur monthly, generally premenstrually, and consisted of intense abdominal pain radiating to both legs, accompanied by headache, nausea, and occasionally vomiting. During severe attacks she would become mute, later stating that she tried to talk but “the words would not come out.” Following a severe episode, she became comatose for 2 weeks and on regaining consciousness, was found to be delirious. After 1 month, the delirium cleared, revealing a Capgras syndrome with reduplicative paramnesia. Although she could recognize her husband, her children, and her house, she believed that there was “something different about them.” She thought that either everything had been duplicated or that she had been “taken by aliens to another planet where things were similar.” She also experienced intense symptoms of depersonalization. She stated that her body felt strange, as though it did not belong to her, and that she did not know whether she existed or not. She also felt that she was not in control of her behavior. She believed that either she had changed and everything else had remained the same or that she was real and everything else had changed. On noticing a familiar birthmark, she decided on the latter explanation. Neuropsychological assessment revealed sensory aphasia, color blindness, visual agnosia, and both episodic and semantic memory impairment. MRI and SPECT were unremarkable, and her EEG revealed nonlocalized nonspecific changes. Her overall DES score was 25; however, she scored 69 on the DP/DR subscale. The Capgras syndrome and the symptoms of DP and DR lasted 6 months, gradually resolving.
Case 2. A 48-year-old right-handed woman with no personal or family neuropsychiatric history suffered a brainstem infarct. MRI revealed multiple areas of increased signal affecting the cerebellum, brainstem, posterior part of the thalamus bilaterally, and the left occipital lobe, consistent with ischemic lesions in the vertebrobasilar territory. Six months following the infarct, she developed low mood accompanied by both DP and DR. She referred to herself as the “old” and “new” selves. She described the “new self” as if “part of me is not me” and “something's missing.” She was anxious that the “new self” might take over. She experienced a reality distortion of objects and unfamiliar people in the outside world, which she described as “I know that it's there…but it's not the same,” and “I know that you're there…but you're not.” She also found that she had to concentrate much harder to understand details of conversation and to register details of other objects and people. Paroxetine relieved the depressive ideation but not the DP and DR, which persisted for several months.
Case 3. A 22-year-old right-handed woman with a family history of depression developed partial epilepsy at the age of 17. The seizures were medically intractable, and thus she underwent a left-sided temporal lobectomy at the age of 18. Pathological examination of the resected temporal lobe revealed Rasmussen's encephalitis. Neuroimaging confirmed the complete removal of all the medial temporal structures. Eighteen months later, her seizures recurred, consisting of a “thumping” sensation in her head, along with fear and the feeling of someone being behind her. They were accompanied by symptoms typical of a panic attack, with palpitations, overbreathing, a dry mouth, a sense of the world closing in on her, and a fear of dying. She also experienced marked symptoms of depersonalization and derealization. She felt that she “wasn't there,” that she was not real, and that she was in a dream. She also felt that the surroundings and other people were not real, as though she were watching television. A video-EEG revealed frequent runs of epileptiform activity originating in the left suprasylvian region and rapidly becoming generalized. The EEG changes were accompanied by her symptoms of panic and depersonalization, confirming the ictal nature of the episodes. She scored highly on measures of anxiety and dissociation while having these frequent seizures (Table 3). The episodes ceased on increasing her anticonvulsant medication.
Case 4. A 32-year-old right-handed woman with no personal or family psychiatric history developed medically intractable posttraumatic epilepsy of occipital lobe origin at the age of 25, 9 months after suffering an assault. The seizures consisted of flashing lights in the right hemifield, which at times would generalize into a tonic-clonic seizure. In addition, she experienced complex partial seizures consisting of a feeling of depersonalization during which she lost the “sense of herself” and episodes in which she felt she went “outside herself” and during which she “observed herself.” During these episodes she was unaware of her surroundings, and they were accompanied by automatisms consisting of plucking actions involving her right hand, along with chewing movements. These seizures also had a tendency to generalize. Neuroimaging revealed a meningioma arising from the left temporal lobe. Following the assault she suffered from PTSD and developed a depressive illness, which was treated with cognitive-behavioral therapy. The seizures, and thus the ictal depersonalization, developed several months after the depression had shown some improvement with therapy. Interictally, her overall score on the DES was 4.3, with a DP/DR subscale rating of 3.3. A left temporal lobectomy relieved the episodes of ictal depersonalization and temporal lobe automatisms, but the occipital seizures remained.
DISCUSSION
ACKNOWLEDGMENTS
References
Information & Authors
Information
Published In

History
Authors
Metrics & Citations
Metrics
Citations
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
There are no citations for this item
View Options
View options
PDF/ePub
View PDF/ePubGet Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
Personal login Institutional Login Open Athens loginNot a subscriber?
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).