Several reports suggest that testosterone engenders aggression in males. Studies in prisoners have found evidence of a positive correlation between testosterone and aggression.
1,2 Violent male offenders show substantially higher plasma testosterone levels than less violent individuals.
1,2 Similar results were obtained from a volunteer male sample divided according to the presence or absence of aggression when drinking alcohol
3 or while playing a competitive sport.
4The relationship between testosterone and aggression in elderly men with dementia has not been systematically investigated. Case studies have reported the efficacy of estrogen treatment on aggressive behavior in 2 men with dementia and in 1 with traumatic brain injury.
5,6 A randomized, double-blind placebo-controlled trial found that estrogen therapy was associated with lower aggression in 7 women and 1 man with dementia in a long-term care facility.
7 Other studies, totaling fewer than 10 patients, have reported that the administration of medroxyprogesterone acetate, estrogen, and leuprolide acetate decreases aggression and sexually aberrant behavior in men with and without dementia.
8–11 We have reported a significant correlation between testosterone levels and physical aggression in 13 men with dementia.
12In this study, we hypothesized that testosterone levels are related specifically to aggression (as distinguished from agitation) and that aggression is specifically and inversely related to estrogen levels.
RESULTS
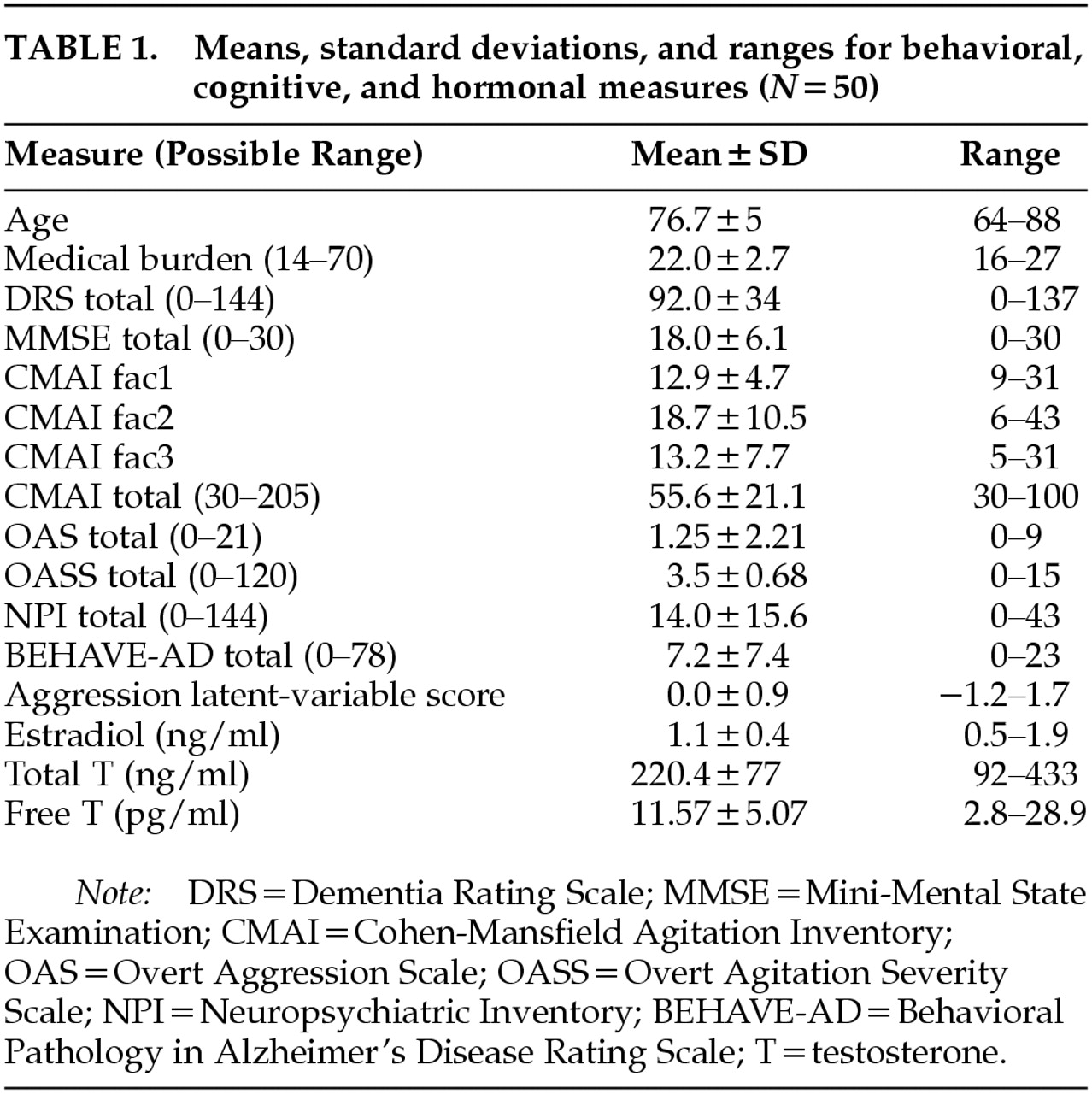
A total of 50 patients met criteria and agreed to participate in the study. Ten patients met criteria but refused to participate. The average age was 76.7±5 years (means and standard deviations are reported). Fifty-eight percent were Caucasian, 30% African American, and 12% Hispanic. Seventy-six percent were living at home, 12% in personal care homes, and 12% in nursing homes. Sixty percent (31 patients) had a diagnosis of Alzheimer's dementia, 28% (14 patients) had a diagnosis of vascular dementia, 6% (3 patients) had a diagnosis of mixed dementia, and the remaining 4% (2 patients) had alcohol-induced persisting dementia. The average MMSE score was 18±6, and the average DRS score was 92.2±34.
Table 1 shows the means, standard deviations, and ranges for the behavioral, cognitive, and hormone measures. The total CMAI score for the subject population is similar to that reported in other studies investigating behavioral dyscontrol in community-dwelling individuals with dementia.
23,27Fit of the data to the latent-variable model measuring aggression was good and demonstrated that the model adequately represented the data, as evidenced by the chi-square test of goodness of fit (χ
2=8.0, df=7,
P=0.33) and the root mean square error of approximation (0.06).
24,25 The reliability of the latent variable was 0.90, and the proportion of variance captured by the latent variable relative to the amount of variance due to measurement error, or the average variance extracted, was 0.69.
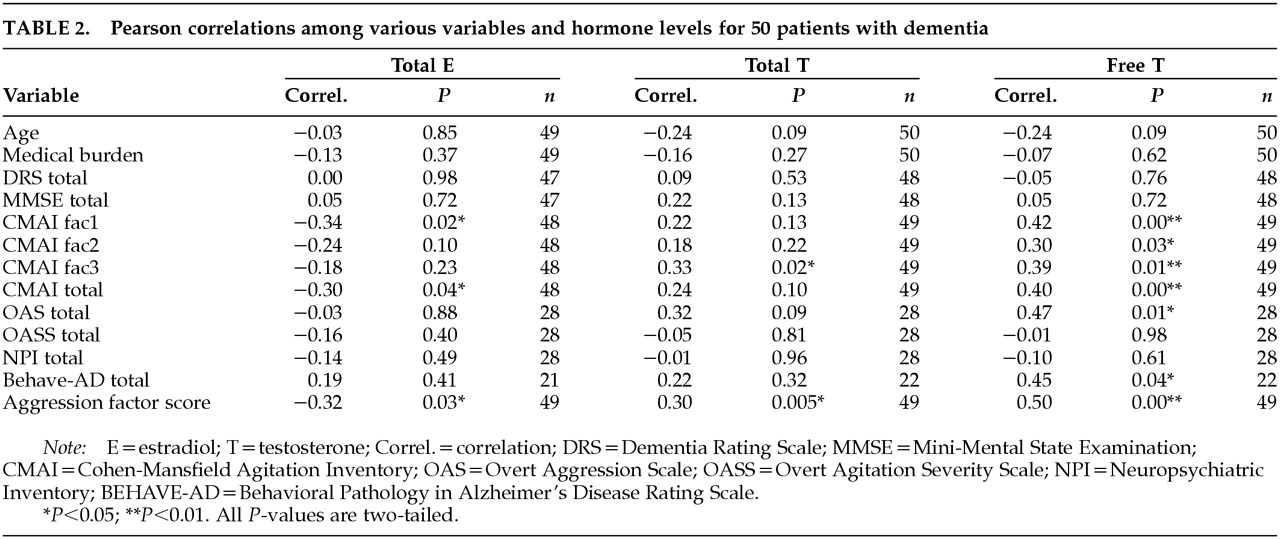
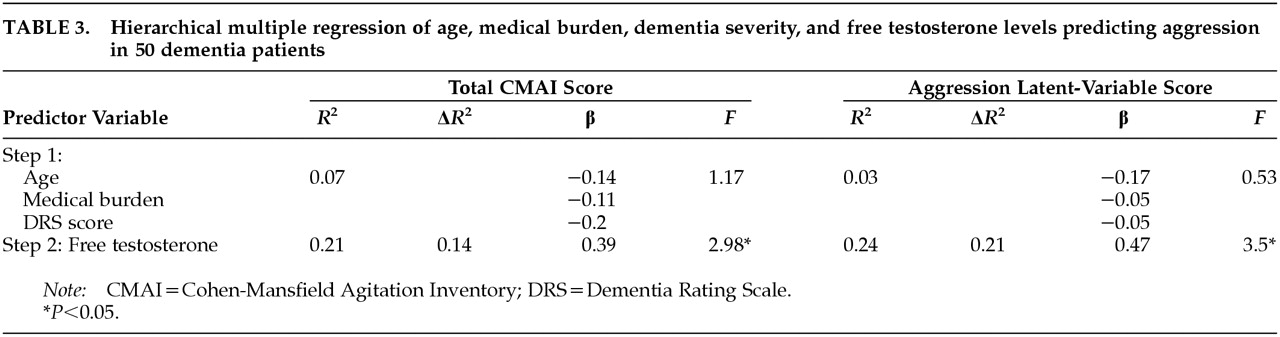
28Table 2 shows the correlation coefficient for hormone levels and measures of cognition and behavior. Significant positive correlations were found between free T levels and CMAI fac1, CMAI fac2, CMAI fac3, CMAI total, OAS, and aggression latent-variable scores. Estrogen levels show a negative significant correlation with CMAI fac1 and total CMAI. Multiple regression equations were computed for total CMAI score and for the aggression latent-variable scores. Age, medical burden (CIRS), and dementia severity (DRS score) were entered on the first step, and free testosterone was entered on the second step.
Table 3 lists the results from the regression analysis. Free testosterone alone accounts for 14% of the variance in total CMAI score and 21% of the variance in aggression latent-variable score.
DISCUSSION
We found levels of testosterone to be positively correlated and levels of estrogen to be negatively correlated with the specific behavior of physical aggression in elderly men with dementia, regardless of the type of dementia. Free testosterone accounts for 21% of the variance in the aggression latent-variable score when controlling for age, dementia severity, and medical illness. The biologic plausibility of the inverse relationship between estrogen and testosterone, together with the finding of specificity that neither testosterone nor estrogen level was associated with other behavior disturbances such as psychomotor agitation (OASS), psychosis (paranoia-hallucination subscale of NPI or delusion-hallucination subscales of BEHAVE-AD), depression, or mania (affect subscale of NPI or depression-euphoria subscale of BEHAVE-AD) adds strength to the finding. When these findings are evaluated in conjunction with the double-blind study by Kyomen et al.
7 showing a temporal relationship between estrogen treatment and decreased aggression, an argument can be made for an important role of testosterone and estrogen in aggression in elderly male patients with dementia.
Often physicians and other healthcare professionals group together many diverse behavioral disturbances as “agitation.” Such a vague, global concept hinders clinical quantification, obscures underlying disorders, and can result in inappropriate use of pharmacotherapy or physical restraints. Aggression is defined as recurrent violent events, either verbal or physical in nature, that are out of proportion to the precipitating stress or provocation and that stem from organic etiologies. Agitation is excessive and/or inappropriate verbal, vocal, or motor activity, which may or may not be voluntary. In this study we show that free testosterone levels are correlated specifically with aggression and not with agitation.
This study measured plasma free testosterone rather than cerebrospinal fluid (CSF) testosterone. Because of its lipophilic nature, testosterone easily passes through the blood–brain barrier in free form (not bound to protein). At the cerebral level, steroid hormones originating from the periphery influence the function of nerve cells dispersed throughout the body. The best example of this influence is the neurons that secrete hypophysiotrophic factors stimulating the production of pituitary hormones such as ACTH and gonadotropins. These hormones are subjected to regulation by the corresponding steroid hormones by a feedback mechanism.
Testosterone and estrogen receptors are primarily located in the limbic areas of the brain. Many studies in animals and humans have found that rage reactions occur with stimulation of limbic structures but not as the result of stimulation of the neocortex.
29,30 Phylogenetically and histologically, the limbic gray matter is clearly more primitive than the other cortical areas. Individuals with dementia have diminished higher cortical function that may lead to a decrease in the psychosocial or environmental influences on behavior. Therefore, a demented individual may be more influenced by primitive or limbic impulses and may lack the inhibitions of learned psychosocial behaviors. This explanation is consistent with the hypothesis that deeper limbic structures contain the template for aggressive behavior but that higher centers, when intact, maintain control of aggression.
Testosterone and estrogen levels appear to be important determinants of the complex behavior termed aggression. However, 79% of the variance of aggression is unaccounted for in our regression model. Clearly other biologic or psychosocial determinants exist and need to be explored. The role of other neurotransmitters such as serotonin, dopamine, norepinephrine, and arginine vasopressin should also be explored. Aggression is an end product of brain function, and although modified, enhanced, or diminished by environmental factors, it has as its nucleus a complex interaction of anatomic, chemical, and physiologic determinants.
Future studies should include larger sample sizes of individuals specifically selected for physically aggressive behavior problems (unrelated to psychosis) to assess adequately the aggression–testosterone relationship with subgroups of aggressive patients with different types of dementia. Future investigations could also measure testosterone levels in CSF to determine if a relationship exists between CSF concentrations of testosterone and aggression.
The results of this study offer new data to aid in the understanding of aggression in elderly men with dementia. We believe that all agitation/aggression in dementia is not the same, and suggest that different behaviors warrant specific treatments. For example, agitated patients with psychotic features require antipsychotics, whereas those with agitated depression do best with antidepressant treatment and those with physical aggression may need androgen-lowering agents. Further research on specific treatments for specific agitated behaviors in elderly patients with dementia is greatly needed. In addition, other factors associated with aggression in patients with dementia should be investigated, including premorbid personality, environmental triggers, aggressor–victim relationship, frontal lobe pathology, and acute medical conditions causing delirium.
The limitations of this study include an all-male sample of veterans in an outpatient geropsychiatric clinic. Nonetheless, our data indicate a specific association between aggressive behavior and testosterone and suggest that trials to test novel treatment approaches for physically aggressive patients (e.g., lowering testosterone levels) should be undertaken. Our nation's population is aging, the incidence of dementia is increasing, and the need to find safe and effective treatments for the behavioral disturbances associated with dementia is growing.