The purpose of this study was to characterize the cerebral electrical activity by qEEG in Chernobyl accident survivors who were diagnosed with ARS (with distinction of confirmed versus nonconfirmed ARS) in order to reveal whether qEEG-abnormalities were related to the absorbed dose in the remote period of exposure to a short-term whole-body relatively uniform ionizing radiation.
METHODS
Background
During the beginning of 2002, there were 188 survivors who were diagnosed in 1986 with ARS, among them, 92 had confirmed ARS (14 patients died from August 1, 1986–2002), and 96 had nonconfirmed ARS (7 patients died from August 1, 1986–2002). At present, the 80 confirmed and 91 nonconfirmed ARS patients live in the Ukraine.
Both confirmed and nonconfirmed ARS patients were exposed to ionizing radiation at the most dramatic period of the Chernobyl disaster: the night of the accident. They had equal medical history after the accident and similar socio-demographical, occupational, economical, and educational levels, namely firemen and personnel of the power station. Social privilege and insurance and the availability and regularity of free, high-quality medical care are the same for all people who were with ARS. The ARS patients are blind to the results of the procedure of ARS verification—all of them have in their medical records the diagnosis of ARS of different degrees of severity, whereas nonconfirmed ARS registered as mild ARS or ARS of the first severity degree. Thus, the main difference between confirmed and nonconfirmed ARS patients was the value of absorbed dose, and this comparison gives a possibility to study the radio-cerebral effects by qEEG.
Patient Selection
During 1996–2001 (10 to 15 years after irradiation), a cross-sectional qEEG study of the patients who were diagnosed with ARS (divided according to confirmed and nonconfirmed ARS) was carried out. In order to control the influences of traditional risk factors that could affect the qEEG pattern, we selected the patients who met the following inclusion criteria: 1) age at the moment of examination <60 years; 2) male; 3) absence of any neuropsychiatric and physical disease or head trauma before the accident; 4) absence of head trauma, stroke, neuroinfections, and dependence on any psychoactive substances (other than tobacco) after the accident; 5) righthandedness; 6) the same qEEG equipment and the regimen of qEEG registration. We enrolled 63 patients into the study (26 with nonconfirmed ARS and 37 with confirmed ARS).
Patients with nonconfirmed ARS and confirmed ARS had no differences in age (M ± SD: 43.1 ± 6.8 and 46.3 ± 7.9 years correspondingly, t = −1.6; df = 61; P = 0.1), but these groups significantly differed in terms of absorbed doses. Dosimetric maintenance of both groups was based on biological dosimetry by cytogenetic studies of lymphocytes carried out by experts from the Institute of Biophysics (Moscow, Russian Federation).
Nonconfirmed ARS patients were exposed in 1986 to acute ionizing irradiation in the dose range 0.2–0.6 Gy (M = 0.32; SD = 0.16; Median = 0.3 Gy).
Confirmed ARS patients were exposed in 1986 to acute ionizing irradiation in the dose range 0.7–5.7 Gy (M = 2.81; SD = 1.61; Median = 2.35 Gy). Among them were 12 patients who had mild ARS or ARS of the first severity degree (dose absorbed (M ± SD) 1.11 ± 0.48 Gy); 18 had moderate ARS or ARS of the second severity degree (2.67 ± 1.1 Gy); and 7 had severe ARS or ARS of the third severity degree (4.89 ± 1.2 Gy).
Nonconfirmed and confirmed ARS patients were in-patients of the Department of Radiation Pathology (Department of Radioinduced and General Occupational Pathology) of the Institute for Clinical Radiology (ICR) of the Scientific Center for Radiation Medicine (SCRM) of Academy of Medical Sciences (AMS) of Ukraine, Kiev, which is the major referral center for Chernobyl accident survivors in the country. All of these patients are under clinical monitoring on the base of regular in-patient medical examinations and rehabilitation in RCRM.
All examined, nonconfirmed and confirmed ARS patients had neuropsychiatric disorders. Organic asthenic (emotional labile) disorder {ICD-10: F06.6 [DSM-IV has no such category and this seems to be rather somatoform disorders (300.81) than labile type of personality change due to general medical condition (310.1)]} was diagnosed in 20 (77%) nonconfirmed ARS patients and 16 (43%) confirmed patients (χ2 = 7.07, df = 1, P < 0.008). Other patients were diagnosed with organic personality disorder (ICD-10: F07.0 or DSM-IV-R: 310.1):6 (23%) nonconfirmed ARS patients and 21 (57%) confirmed ARS patients (χ2 = 7.07, df = 1, P < 0.008). The most characteristic, apathetic, type of organic personality disorder was diagnosed in 3 (11.5%) nonconfirmed ARS patients and 18 (49%) confirmed ARS patients (χ2 = 9.46, df = 1, P < 0.002).
Procedures
Neurophysiological investigations were carried out in the screened neurophysiological laboratory of the Department of Neurology (Department of Radiation Psychoneurology) of ICR of RCRM of AMS of Ukraine in the first half of the day during the passive awake state of a patient. The patients were nonmedicated for 3 or more days.
Quantitative EEG was performed with a 19-channel brain biopotentials analyzer (Brain Surveyor, SAICO, Italy). The brain spontaneous electric activity was monopolarly registered with linked ears reference. Nineteen scalp electrodes were placed according to the 10–20 International System. Quantitative EEG registration was made using silver-silver chloride bridge electrodes (Ag-AgCl) attached by gel. Quantitative EEG was registered at passive awake, when patients' eyes were closed. Visual and spectral analyses of EEG were carried out. Epochs used in the analysis were 60 seconds. The obtained frequency band was 1–32 Hz. All of the EEG records were visually edited for artifacts; prior to analysis artifacts due to eye or muscle movements or respiration were removed blind to subject group. Spectral analysis was carried out using classical Fast Fourier Transformation methods. Absolute total spectral power (μV2Hz−1) for 1–32 Hz band, dominant frequency (Hz) for 1–32 Hz band, absolute (μV2Hz−1) and relative (% to the whole spectrum) spectral power in the main frequency bands: δ (1–4 Hz), θ (>4–7 Hz), α (>7–12 Hz), and β (>12–32 Hz) were obtained automatically. Summarized total absolute power and summarized relative/absolute power of certain frequency band (δ, θ, α and β) was assumed as the average value of corresponding spectral power in all leads. There were analyzed numerical indices and brain maps of qEEG-parameters.
Laterality (interhemispheric asymmetry) was assessed by equation as follows:
Lat = (L—R) / (L + R)100%,
where Lat—laterality coefficient;
L—qEEG-parameter of symmetrical area of the left hemisphere;
R—qEEG-parameter of symmetrical area of the right hemisphere.
Laterality was considered to be significant at Lat > 5%.
Statistical analysis was performed using STATISTICA 5.0 and MS EXCEL software. Statistical processing included descriptive statistic, ANOVA, Student's t test, the Chi-square test (criterion χ2), Pearson product-moment correlation and regression analysis. t-criterion of differences between patients with nonconfirmed ARS and confirmed ARS, as well as linear correlation coefficients between qEEG-parameters and absorbed dose of ionizing radiation were also presented as brain maps.
RESULTS
Taking into account a uniqueness of the sample of patients who were diagnosed with ARS as a result of the Chernobyl accident, we present the comparative descriptive characteristic of patients with confirmed ARS and nonconfirmed ARS in spite of the differences between them on the base of the conservative control for Type I error (p < 0.001) would be recognized as a tendencies only.
There is the tendency toward a diffusive decrease of total absolute spectral power of cerebral electrical activity (band 1–32 Hz) in confirmed ARS patients in comparison with nonconfirmed ARS patients (summarized total absolute power 65 ± 49 and 71.1 ± 50.9 μV
2Hz
−1 correspondingly,
t = −0.5;
df = 61;
P > 0.05) that reflects increased number of low-voltage/flat EEG-patterns
7 according to visual analysis of EEG among confirmed ARS patients in comparison with nonconfirmed ARS patients (25 (68%) and 11 (42%) correspondingly, χ
2 = 3.98;
df = 1;
P < 0.046).
Generalized slowing of EEG-pattern is characteristic for confirmed ARS patients that testify to organic EEG abnormalities.
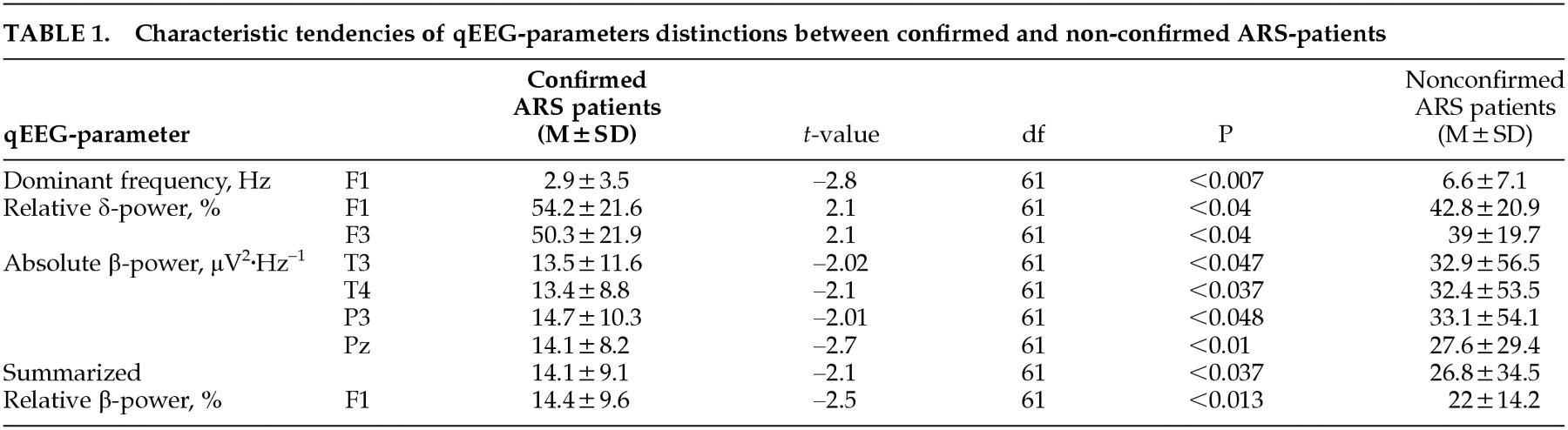
18 There is the tendency toward a diffusive decrease of dominant frequency (band 1–32 Hz) in confirmed ARS patients in comparison with nonconfirmed ARS patients (summarized dominant frequency 5.4 ± 5.2 and 6.9 ± 6.1 Hz correspondingly,
t = −1;
df = 61;
P > 0.05), which is more prominent (
F = 7.8; df
Effect = 1;
P < 0.007) in the left frontal area (
Table 1,
Figure 1). Generalized slowing of EEG with a decrease of cerebral electrical activity frequency below 8 Hz at the posterior brain area is considered to be the clear marker of encephalopathic EEG-pattern.
18 In both groups 30 (48%) patients with dominant frequency in the parieto-occipital area <8 Hz are revealed. In confirmed ARS patients there are somewhat more such patients in comparison with nonconfirmed ARS patients: 19 (51%) and 11 (42%) correspondingly (χ
2 = 0.5;
df = 1;
P = 0.48).
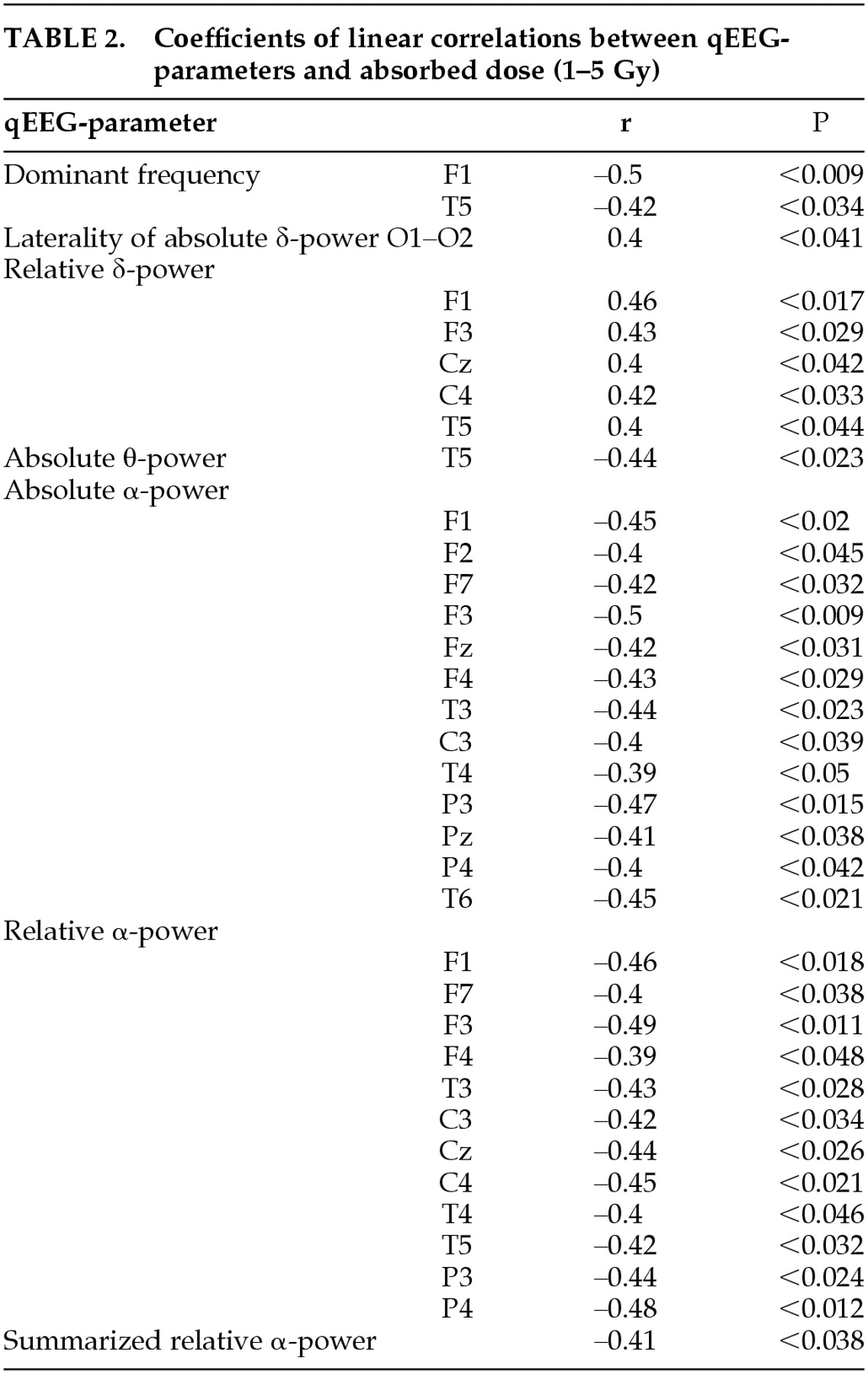
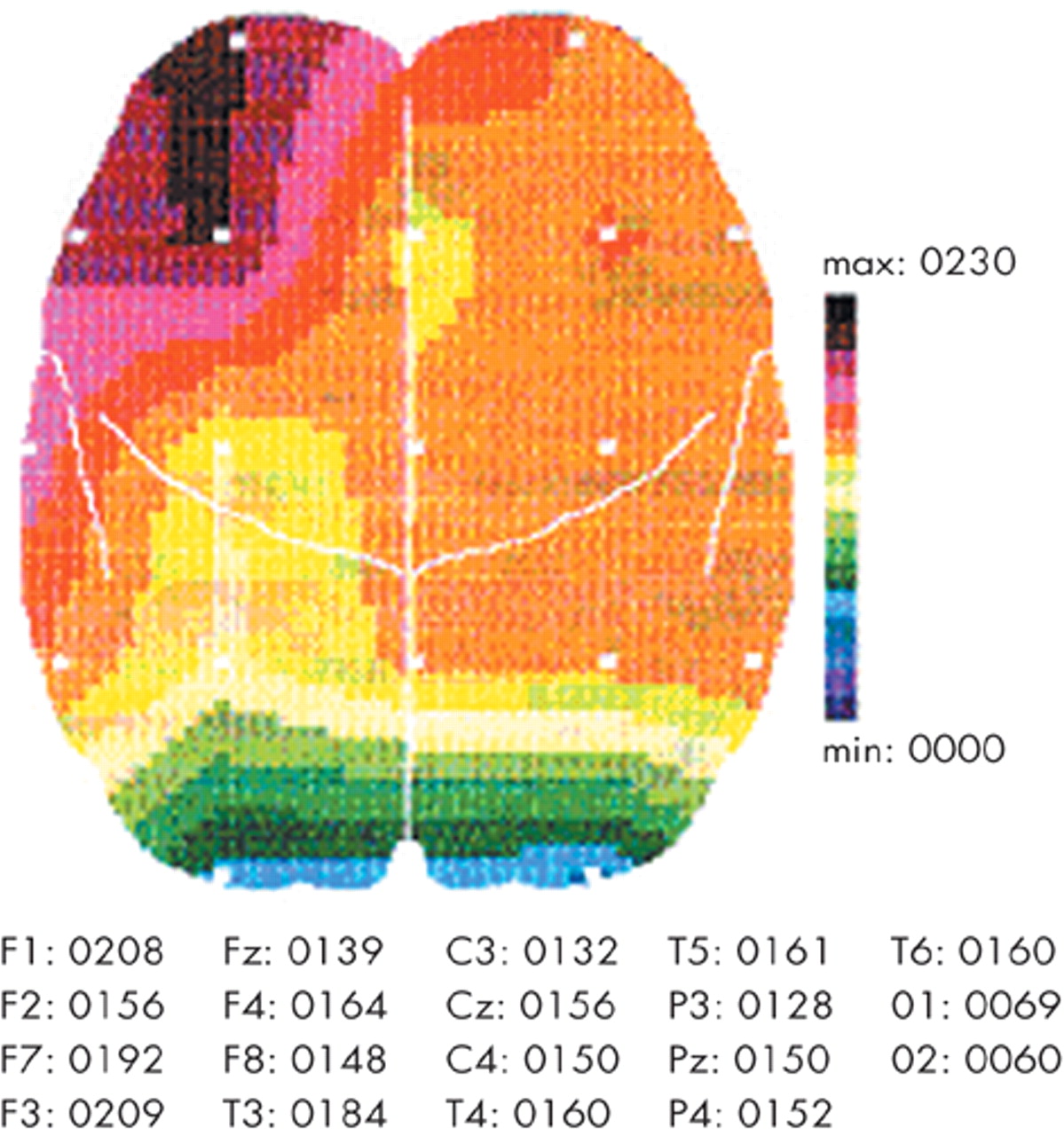
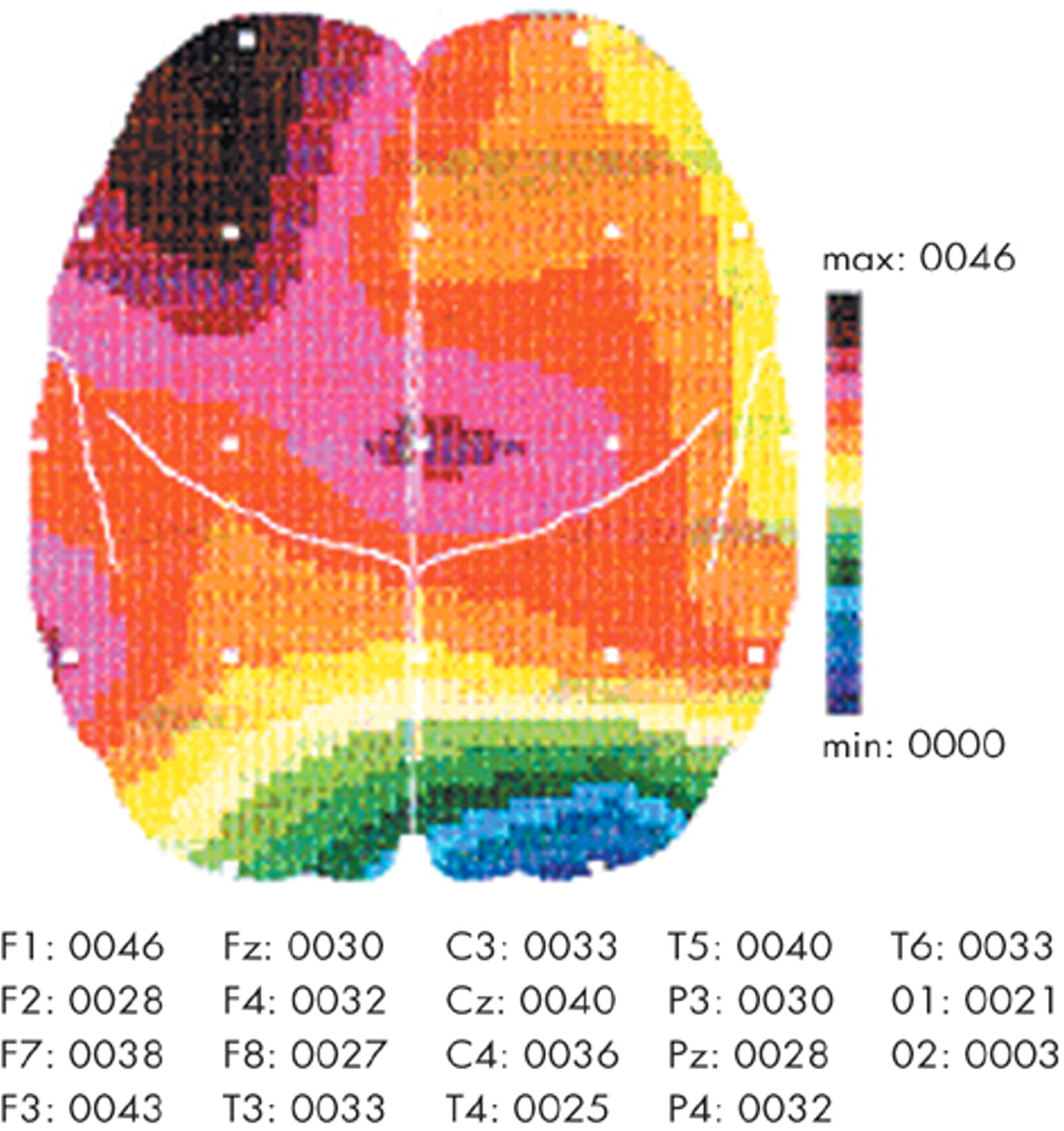
In spite of the tendency toward a decrease of total absolute spectral power in confirmed ARS patients in comparison with nonconfirmed ARS patients, confirmed ARS patients have the opposite tendency toward an increase of absolute δ-power in comparison with nonconfirmed ARS patients (
Figure 2): summarized absolute δ-power 37 ± 34 and 27.8 ± 23.4 μV
2Hz
−1 correspondingly,
t = 1.2;
df = 61;
P > 0.05). Although these differences do not reach to statistical significance, they are more prominent in the left frontal region. Confirmed ARS patients have somewhat more absolute δ-power in the left frontal and right central areas (
Figure 2), as well as the absolute δ-power laterality coefficient in frontal region (F3–F4) is 6.7% while in nonconfirmed ARS patients this is opposite: −1.19% that could reflect a greater involvement of the left, dominant, hemisphere following exposure to ionizing radiation.
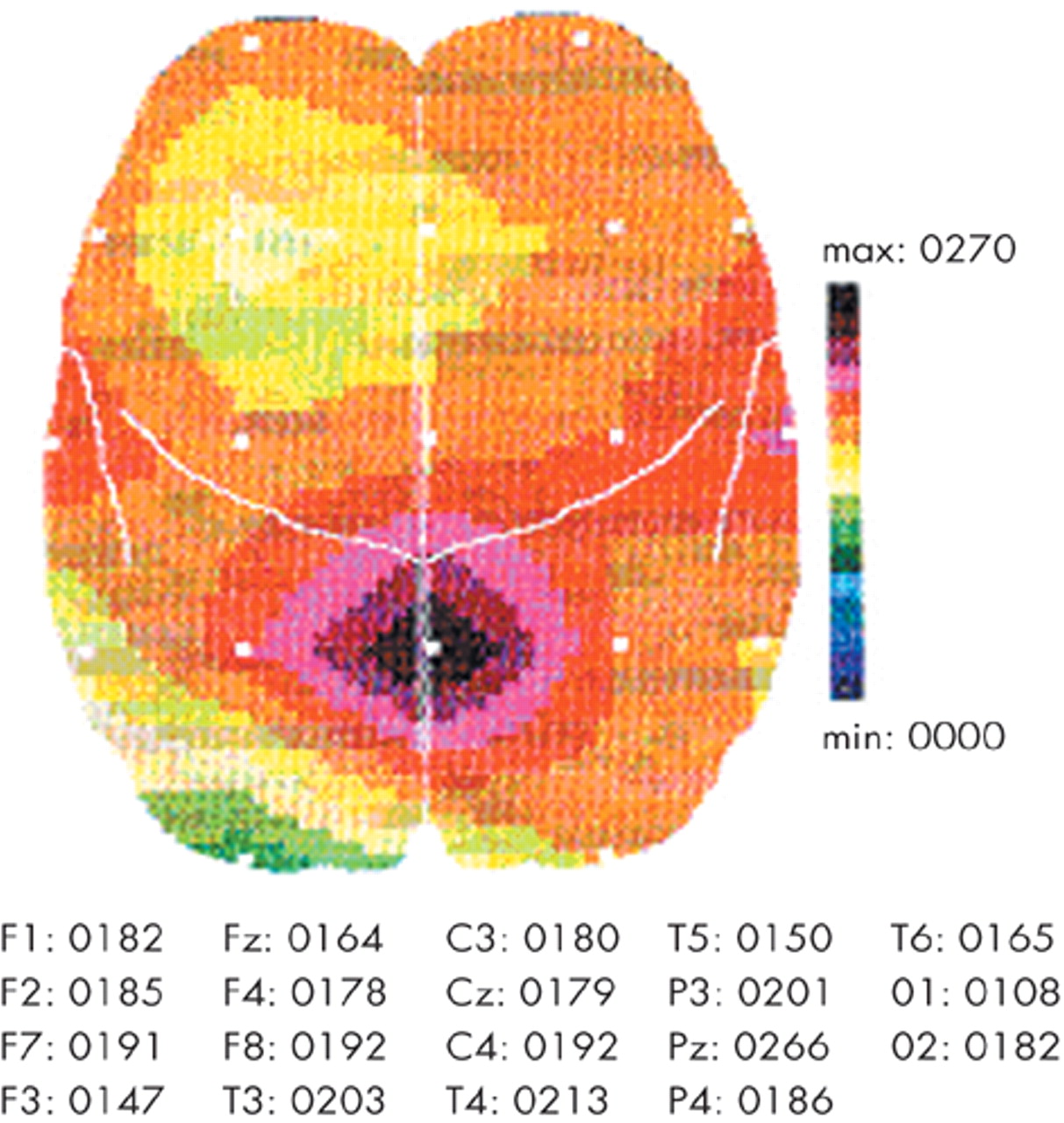
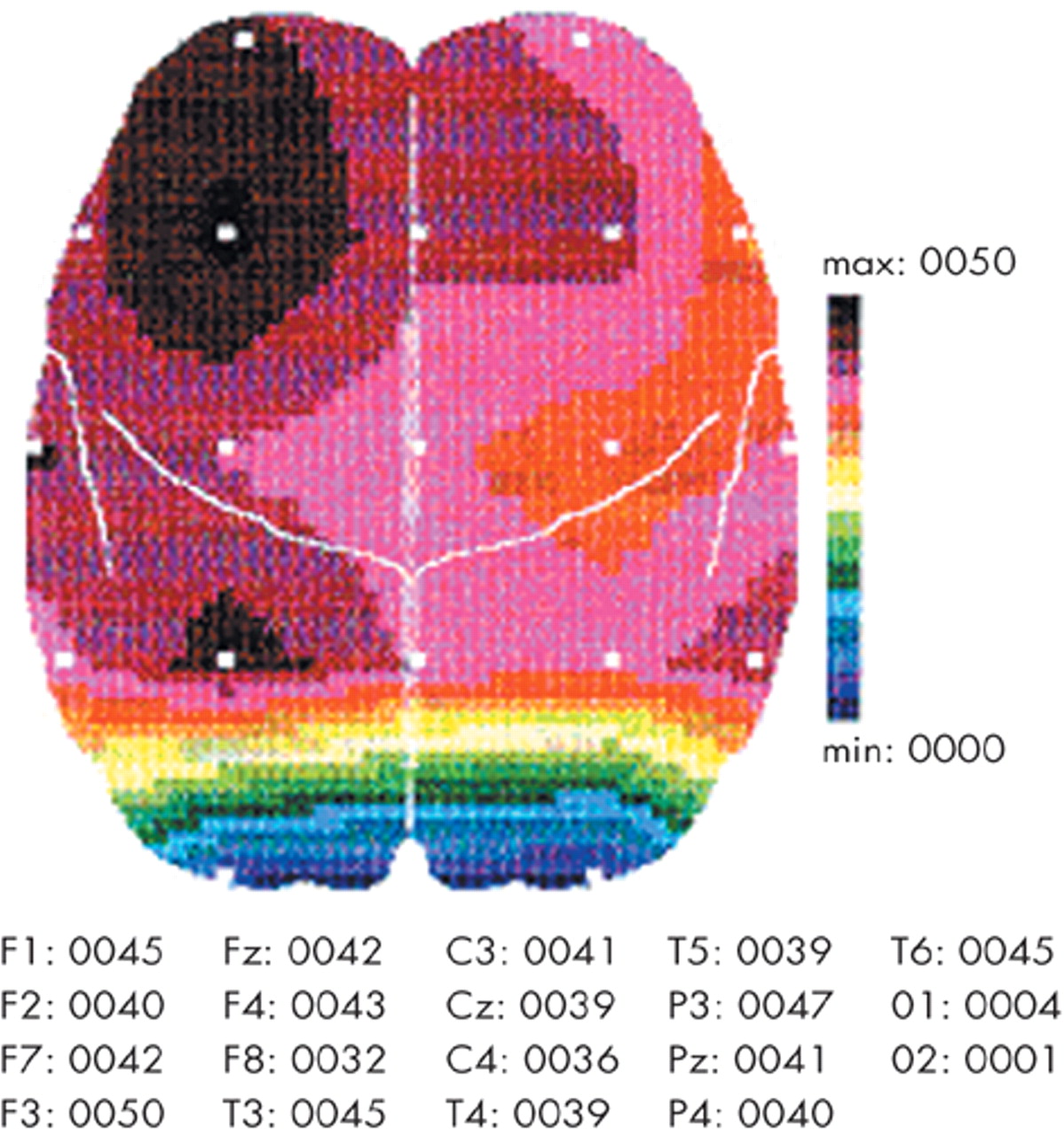
In confirmed ARS patients there is the tendency toward a diffusive increase of relative δ-power in comparison with nonconfirmed ARS patients (
Figure 3): summarized relative δ-power 44.8 ± 20.4 and 36.3 ± 17.1% correspondingly,
t = 1.72;
df = 61;
P = 0.09), which is more prominent (
F = 4.3; df
Effect = 1;
P < 0.04) in the left frontal area (see
Table 1,
Figure 3) that supports a greater involvement of the left, dominant, hemisphere following irradiation.
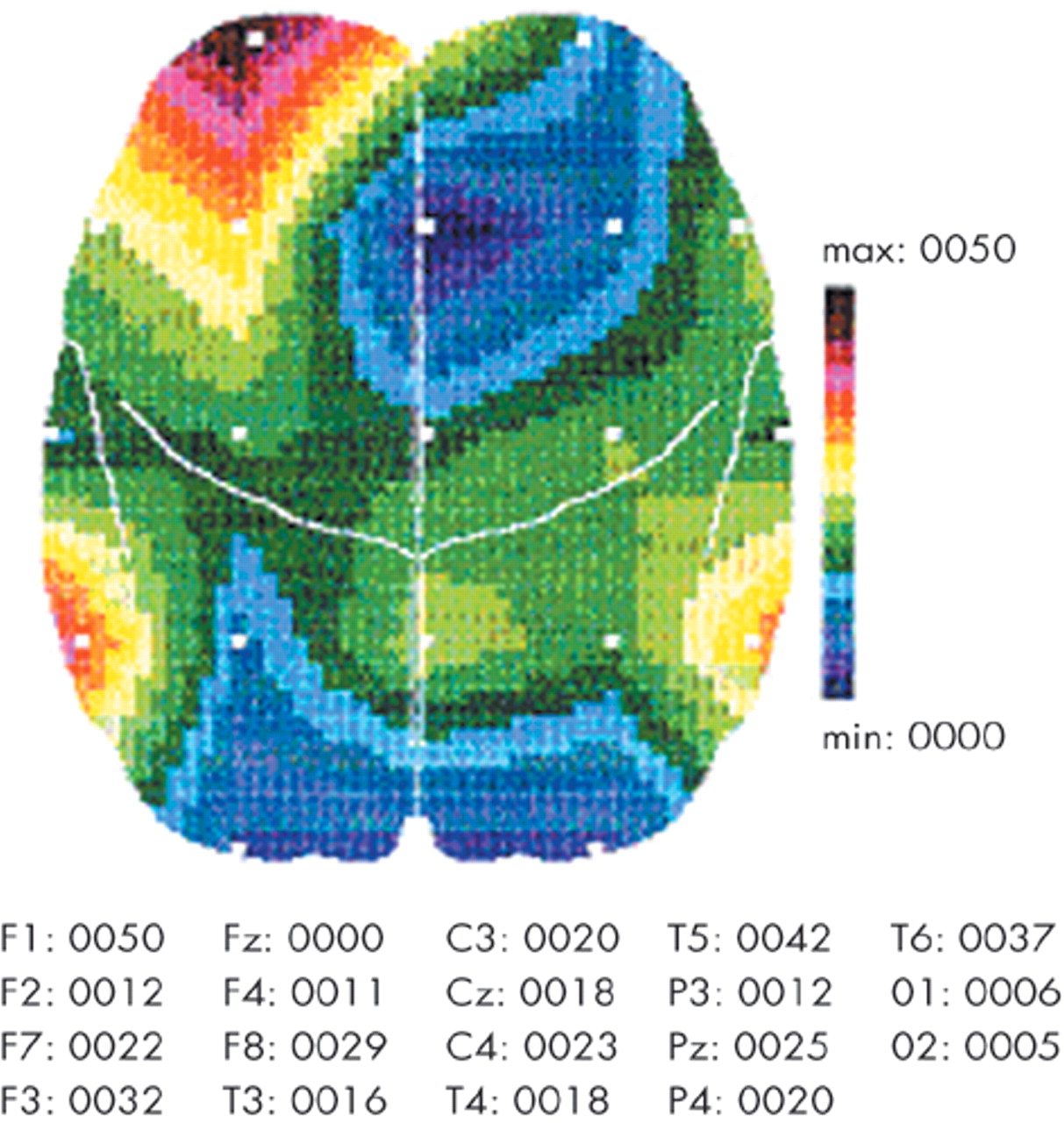
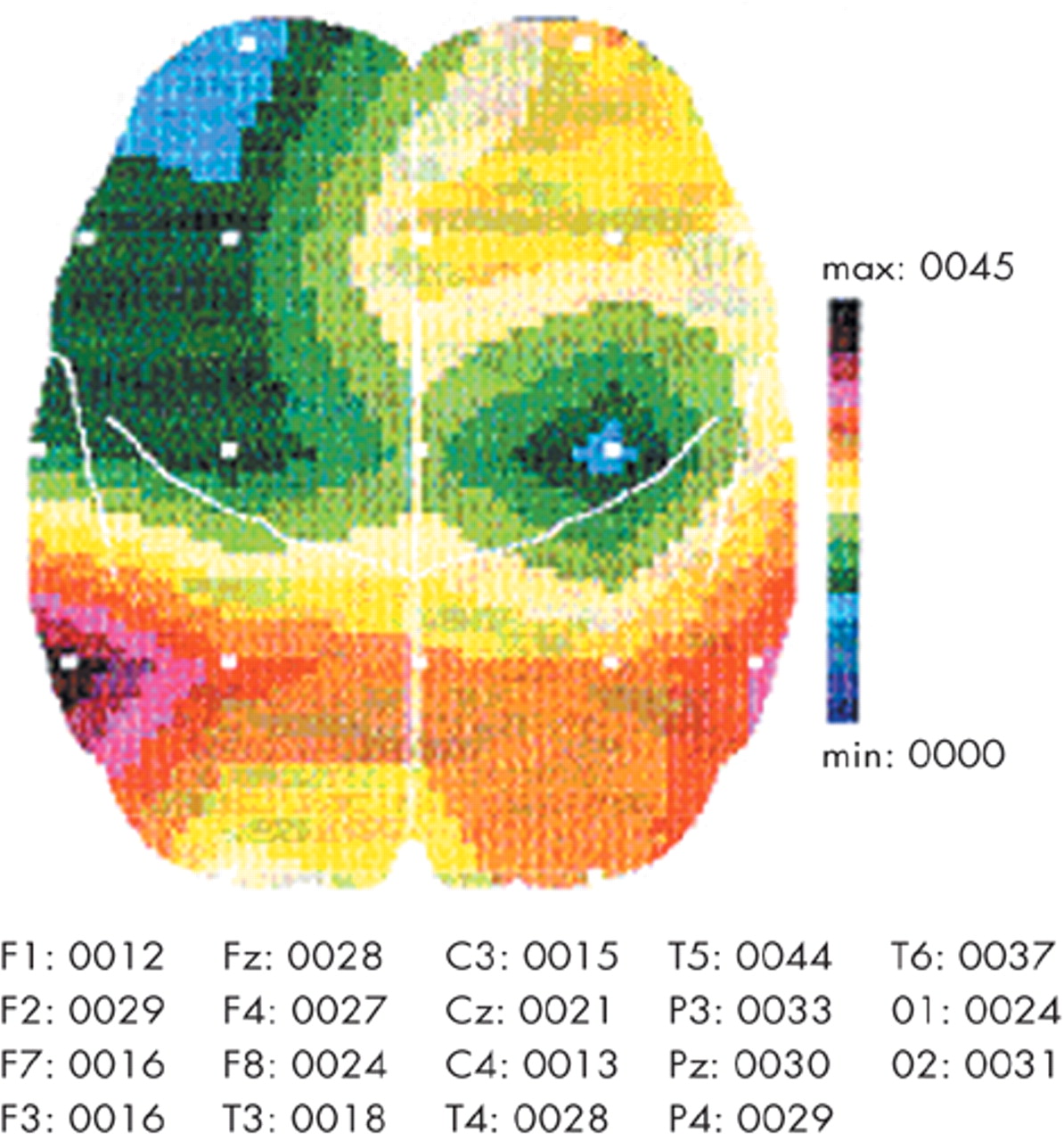
Absolute and relative θ-power are the lowest among all frequency bands of qEEG in the all irradiated patients: summarized absolute θ-power is 6.5 ± 4.4 μV2Hz−1 and summarized relative θ-power is 6.6 ± 3.3% only. When compared with nonconfirmed ARS patients, confirmed ARS patients patients showed tendency toward decrease in the left temporal region of absolute θ-power (6.5 ± 4 and 7.2 ± 6.2 μV2Hz−1 correspondingly, t = −0.5; df = 61; P > 0.05) and relative θ-power (9.1 ± 4 and 10.1 ± 8.5% correspondingly, t = −0.6; df = 61; P > 0.05).
There was the tendency toward a diffusive decrease of absolute and relative α-power in confirmed ARS patients in comparison with nonconfirmed ARS patients—summarized absolute α-power 25.8 ± 19 and 31 ± 23.9 μV2Hz−1 correspondingly (t = −0.95; df = 61; P > 0.05) and summarized relative α-power 29.1 ± 15.6 and 32 ± 19.1 μV2Hz−1 correspondingly (t = −0.66; df = 61; P > 0.05).
In confirmed ARS patients, as compared with nonconfirmed ARS patients, there were decreased indices (
Table 1,
Figure 4) as follows: summarized absolute β-power (
F = 4.5; df
Effect = 1;
P < 0.037), absolute β-power in the left temporal (
F = 4.1; df
Effect = 1;
P < 0.047), the right temporal (
F = 4.5; df
Effect = 1;
P < 0.037), the left parietal (
F = 4; df
Effect = 1;
P < 0.048), and the central parietal (
F = 7.1; df
Effect = 1;
P < 0.01) areas, as well as relative β-power in the left frontal region (
F = 6.5; df
Effect = 1;
P < 0.01) against the background of the tendency toward a diffusive decrease of relative β-power (20.9 ± 12.2 and 25.6 ± 13.5% correspondingly,
t = −1.43;
df = 61;
P > 0.05).
In the entire group of patients diagnosed with ARS and in nonconfirmed ARS patients, significant dose-effect relationship between qEEG parameters and absorbed dose was not revealed. Dose-effect relationship was revealed in the confirmed ARS patients exposed to ionizing radiation in the dose range 1–5 Gy (
n = 26). That could be explained by an existence of the dose threshold of 1 Gy of acute whole-body irradiation for brain abnormalities development persisting 10 to 15 years after exposure as a result of the Chernobyl accident. Factors such as individual radiosensitivity/radiovulnerability, uncertainties of the assessment of the values the individual absorbed dose, etc. should also be considered. This relationship corresponds to the qEEG differences between confirmed and nonconfirmed ARS patients (
Table 2).
Slowing of qEEG-pattern is in proportion to absorbed dose (
Figure 5,
Table 2). A decrease of dominant frequency has a statistical significance in the left fronto-temporal area only.
Lateralization of absolute δ-power to the left occipital area significantly increased with growth of absorbed dose (
Table 2).
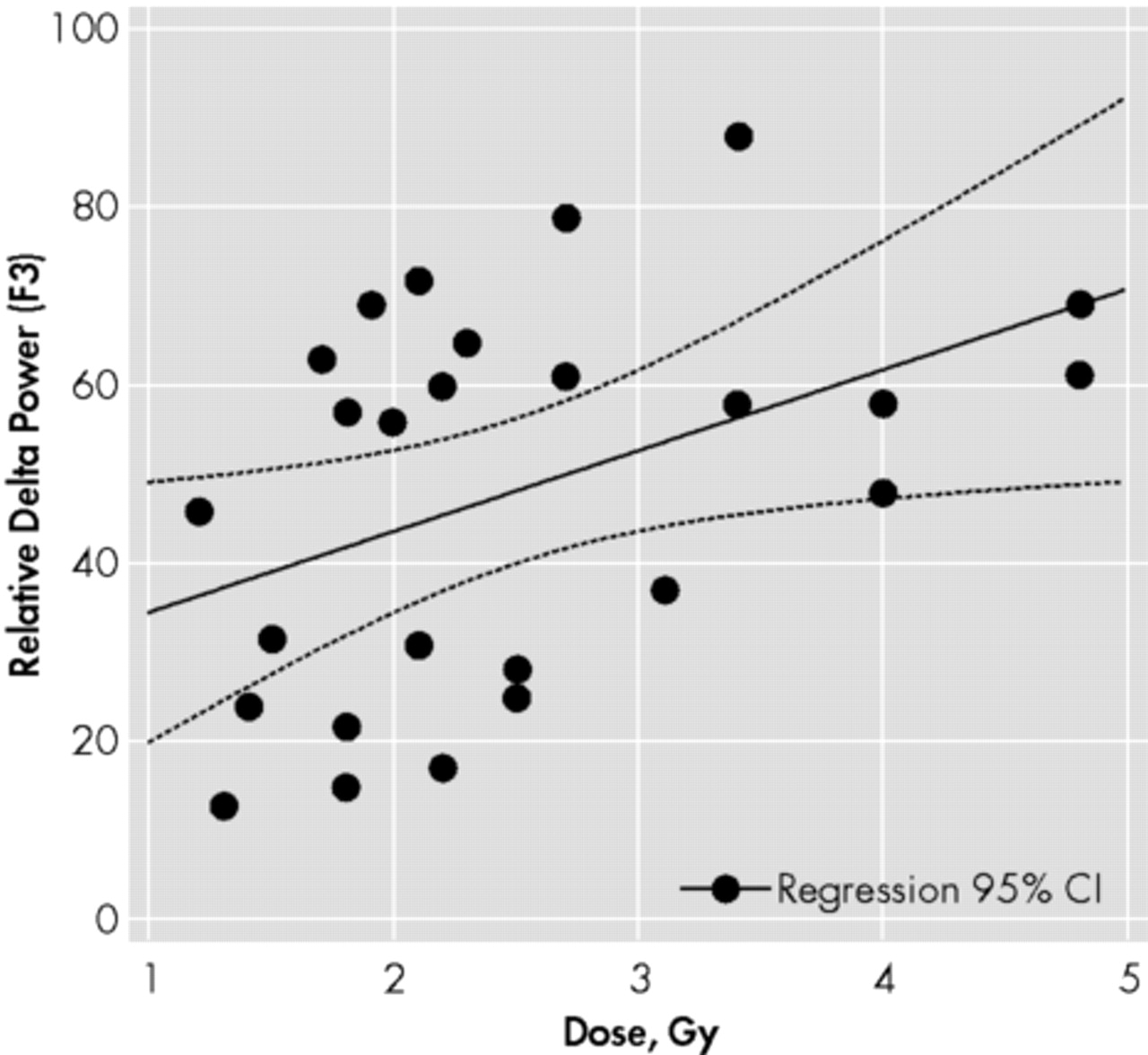
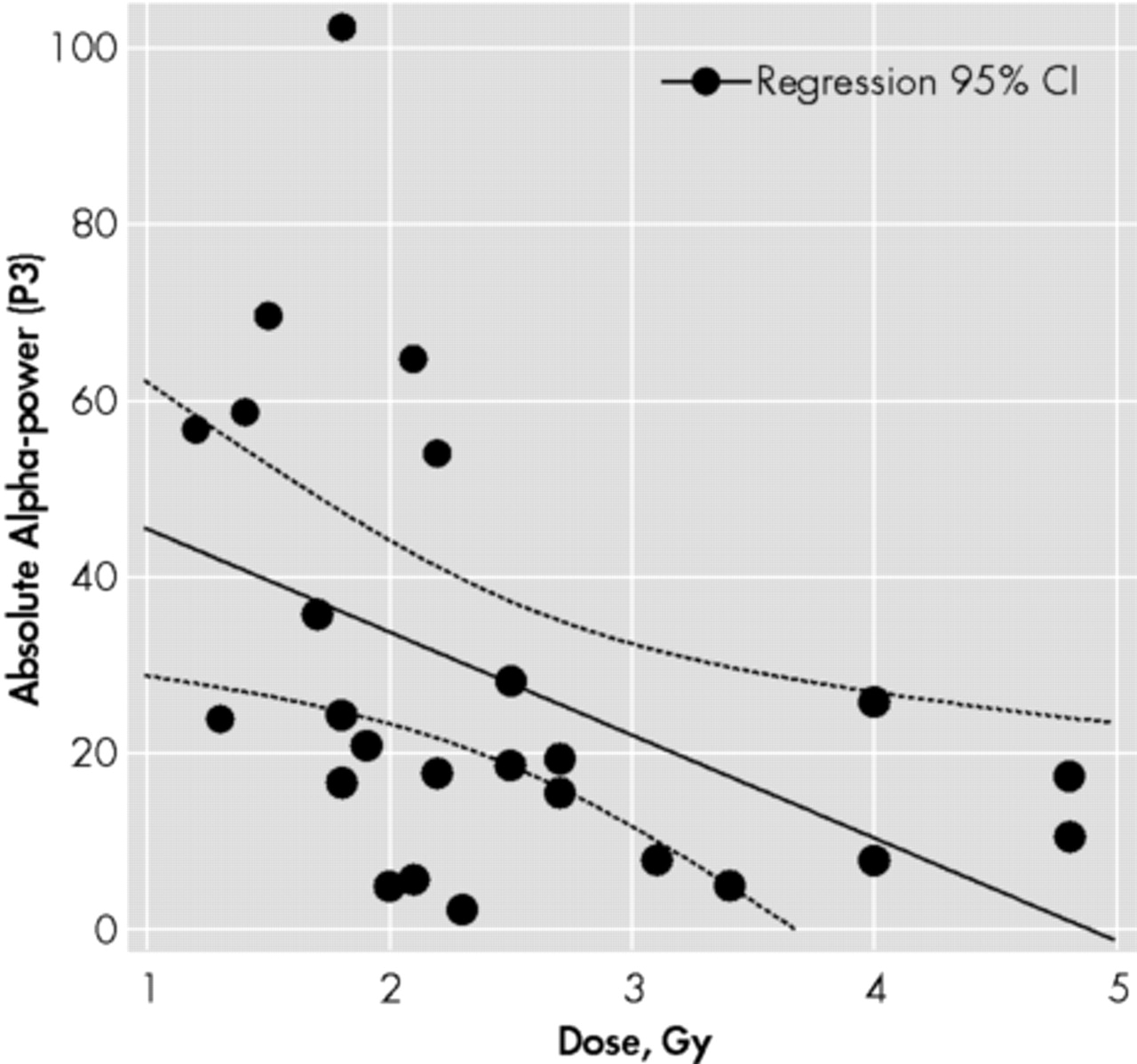
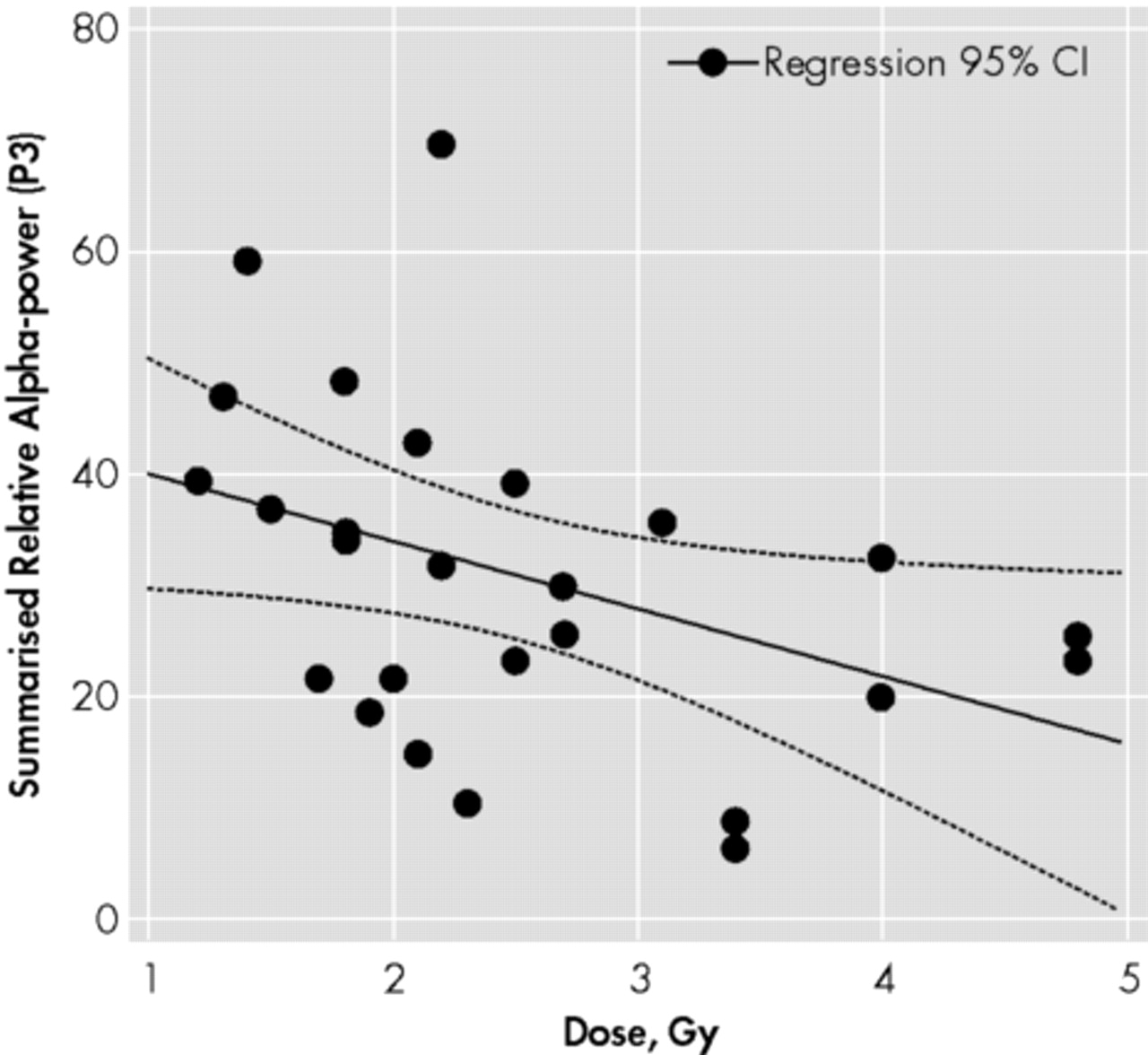
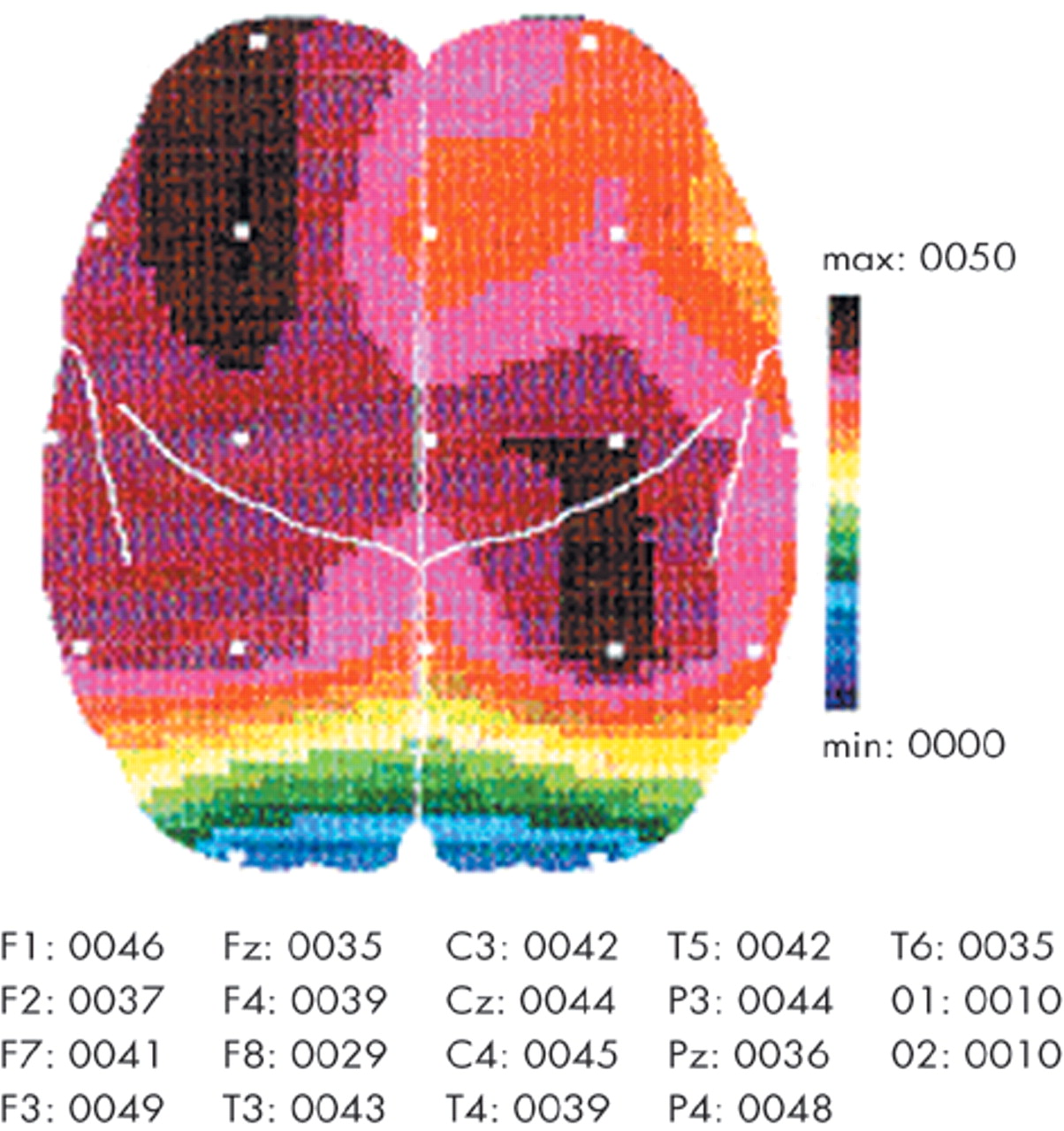
Relative δ-power significantly increased in proportion to absorbed dose, especially in the left fronto-temporal area (
Figure 6,
Figure 7,
Table 2).
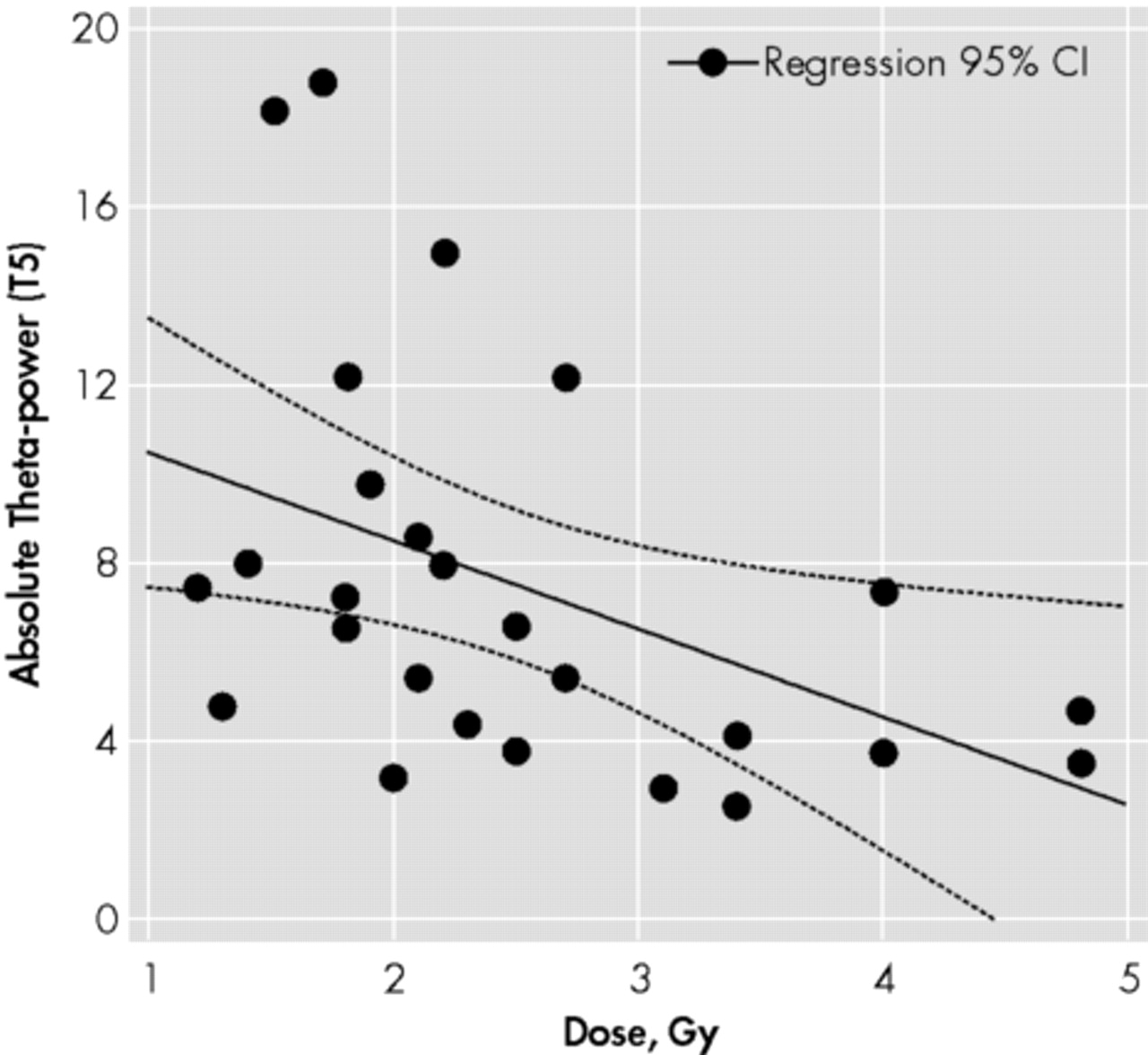
Absolute θ-power significantly decreased proportionally to absorbed dose in the left temporal area (
Figure 8,
Figure 9,
Table 2).
Thus, in confirmed ARS patients exposed to ionizing radiation of 1–5 Gy the most characteristic qEEG abnormalities related to the absorbed dose (that could be recognized as neurophysiological markers of ionizing radiation) are as follows: a reduction of dominant frequency in the left fronto-temporal area; lateralization of absolute δ-power to the dominant, left, hemisphere; an increase of relative δ-power in the fronto-temporal areas also lateralized to the dominant, left, hemisphere; a decrease of absolute θ-power in the left temporal region; diffusive decrease of absolute and relative α-power with their depression lateralization to the left hemisphere.
DISCUSSION
The following interpretation of the data obtained is highly speculative, aiming to integrate the current knowledge in neuropsychiatry and radiobiology.
Generalized slowing of EEG pattern in ARS patients testifies to organic EEG abnormalities.
18 Dose-effect relationship for slowing in the left fronto-temporal region could reflect radiation-induced brain damage mainly in this area.
Dose-related increased δ-power could be interpreted as disinhibition of neurons in deep cortical layers and in the thalamus, normally inhibited by input from the ascending reticular activating system in the midbrain,
19 due to inhibition of reticular formation and posterior hypothalamus.
20Rhythmic θ-activity might originate from direct cortical activation, or from the cortical activation driven by the neuronal impulses from the limbic system.
21 Hippocampal θ-activity results from activation in the ascending synchronizing system.
22 Consequently, dose-related reduction of θ-activity in the left temporal region could be explained as cortical and limbic, particularly, hippocampal damage.
23–27Dose-related diffusive depression of α-power in the frame of current neurophysiological theories could be outlined as 1) thalamic, 2) thalamocortical, 3) cortical, 4) hippocampal and/or 5) diffusive brain damage.
28Diffusive reduction of β-power in confirmed ARS patients could be explained as dysfunction (inhibition) of corticocortical and thalamocortical transactions
19 and decreased thalamic and nucleus caudate input on cortex.
20We propose to classify as dominant-cortical syndrome the revealed characteristic qEEG-pattern of the remote period of ARS following exposure to ionizing radiation in doses of 1–5 Gy. Abnormalities, mainly in the cortex of the dominant (left) hemisphere, may be recognized as the cerebral basis of this syndrome. This does not mean that pathology is localized in the cortex only and in the dominant hemisphere only. However, involvement of other cerebral structures and systems seems to be secondary and subordinated. Dominant-cortical syndrome may be caused by abnormalities, mainly in the limbic, associative frontal and temporal cortex, as well as in the secondary cortical receptor fields and the tertiary associative area. These disorders during the postaccidental years have no topographic changes, but irritation (overactivation) at the first years after exposure transformed toward inhibition and brain organic damage in the remote period.
7,9–17An EEG pattern of dominant-cortical syndrome in the remote period of ARS is low-voltage (<30 μV) or flat polymorphous EEG with prevalence of δ-activity, lateralized to the dominant hemisphere, together with depression of α- and θ-activity. In contrary to low-voltage polymorphous EEG-pattern in irradiated by lower dose persons, described by us before,
7,14,29–33 in the confirmed ARS patients (doses > 1 Gy) β-power is diffusively decreased. Accordingly, neurophysiological mechanisms of dominant-cortical syndrome in the remote period of confirmed ARS could be described as a damage of the cortex and hippocampus of the dominant hemisphere, decreased thalamic and nucleus caudate input in the cortex together with inhibition of the posterior hypothalamus and brain-stem reticular formation.
Personality changes, negative psychopathological symptoms, schizotypical symptoms, cognitive disturbances, as well as paroxysmal states (similar to temporal and/or mediobasal limbic epileptic syndromes) described in ARS patients
7,9–17,31 could be satisfactorily explained in the frame of dominant-cortical syndrome, where limbic, associative frontal and temporal cortex is mainly involved.
34–36 Pathology of the secondary cortical receptor fields and, especially, the tertiary associative region of the dominant hemisphere is the cerebral basis of disorders of afferent synthesis and the central mechanisms of afferentation.
37 This could explain abnormal somatosensoric and somatovisceral sensations, psychosensoric and hypochondriac disorders in the remote period of ARS.
14,38Disturbances of frontal associative cortex of the dominant hemisphere are the cerebral basis of negative psychopathological symptoms
35,36 in the remote period after irradiation. Moreover, depression, increased in 10–15 years after the Chernobyl accident among ARS patients,
9–17,31 could also be explained with damage of the left frontal region. Due to injury of the dominant hemisphere, its transcallosal inhibition control of the nondominant hemisphere is significantly reduced. Consequently, the right hemisphere, associated with depression, becomes disinhibited. This neurophysiological model has been clearly demonstrated for poststroke depression that frequency is significantly higher after left-hemispheric stroke than after right-hemispheric stroke.
35,36Involvement of the dominant hemisphere, particularly left fronto-temporal region in persons exposed to ionizing radiation was reported in studies of other authors.
39–43 In remote period of irradiation there were revealed pathology of both diencephalo-brain-stem and mediobasal cortical structures. Moreover, they proposed corpus callosum to be involved in postradiation brain damage.
44Earlier, we proposed that the left (dominant) hemisphere is more vulnerable in right-handed men, to the whole-body irradiation than the right.
7,16,17 Now we propose that the neocortex seems to be more radiosensitive than subcortical structures and brain stem. The well-known fact that the weight of the cerebral cortex consists of 78% of the whole brain weight
45 should be taken into account. Consequently, following exposure to external uniform ionizing radiation the neocortex is irradiated in 3.5 times much more than all another brain structures. Moreover, the frontal cortex includes 23.5% of the all cortex and has the most sophisticated cytoarchitecture. The temporal cortex consists of 23.5% of the entire cortex, the insular, and limbic cortex, 1.8% and 4% correspondingly.
45 So, the cortical part of the cortico-limbic system includes the major part (52.8%) of all brain cortex or 41.1% of the whole brain weight that resulted in its involvement in the majority of neuropsychiatric disorders, including those following exposure to ionizing radiation.
A unique blood supply of the neocortex is another important factor of higher cortical radiosensitivity due to modification of radiation effects as a result of the well-known in radiobiology oxygen effect—an increasing radiation effects in proportion to oxygen level in organ or tissue that leads toward an intensification of peroxidation of cellular structures and furthers their damage.
46–48 The brain consumes above 50 ml of O
2 per minute that is above 20% of general oxygen consumption by human in rest. Blood supply of the brain (that has 2.5% only of the whole body weight) consists of 15% of heart output. Blood supply of different brain regions is not similar:
491) blood circulation in the cortex is significantly higher than in white matter;
2) blood circulation in the frontal regions is significantly higher than in other cortical parts; and
3) blood circulation and metabolism in the dominant (left) hemisphere is significantly higher than in the nondominant (right) hemisphere.
49Thereby, more intensive blood circulation and metabolism in the cortex, particularly in the frontal regions of the left (dominant) hemisphere could be the basis of their increased vulnerability to exposure to ionizing radiation.
Interhemispheric differences (laterality) of radio-cerebral effects should be discussed on the base of neuroanatomical peculiarities of brain hemispheres in right-handed men. According to neuroimaging data the dominant (left) hemisphere distinguished with as follows:
higher percent of gray matter;
50higher metabolical activity;
49higher blood circulation;
49 and
higher volume of
planum temporale in Wernicke's area
37On the basis of the oxygen effect, we could explain higher vulnerability to irradiation of the dominant hemisphere in comparison with the nondominant. The neurobiological basis of increased radiosensitivity of the dominant hemisphere seems to be higher intensity of metabolism and blood supply resulting in increased concentration of oxygen in tissue of this hemisphere followed with increased formation of free radicals with the development of peroxidative damage of neurons.
The classical radiobiology is based on the foundation by French radiotherapeutics Bergonie and Tribondeau (1906) for the cancer radiotherapy, where the sensitivity of cells to irradiation is in direct proportion to their reproductive activity and inversely proportional to their degree of differentiation. Accordingly, adult brain is recognized as an excellent example of a closed static population and, because of its fixed postmitotic state, this population was considered as extremely radioresistant.
48 Consequently, white matter, together with cerebral vessels (glial-vascular union), was recognized to be more radiosensitive than gray matter because of an absence of neuronal mytotical activity.
51 However, this approach refers to nuclear deoxyribonucleic acid (DNA) only.
Recently, increased attention has been given to mitochondrial DNA damage in the pathogenesis of neuropsychiatric disorders.
52 In contrast to nuclear DNA,
53 the mitochondrial genome has greater instability due to an absence of effective reparative systems. Mitochondrial DNA, especially in neurons, is dramatically more vulnerable to exposure to ionizing radiation than nuclear DNA.
54 Mitochondrial DNA was proposed by Beregovskaya et al. (1989) as a possible target of ionizing radiation exposure.
55,56Radiation-induced damage of mitochondrial DNA in postmitotic tissues with low proliferation activity was proposed to be a part of the basis of the effects of low doses concerning an increase of noncancer morbidity and mortality in the Chernobyl accident survivors.
57 A high radiosensitivity of the brain, along with deterministic neuropsychiatric radiation effects, could be explained by radiation-induced damage of neuronal mitochondrial DNA, which caused a progressive decrease of energetic supply of neurons and synthesis of neuromediators due to an absence of reparation. This leads toward well-known polyneurotransmitter radiation effect.
58,59Revealed neurophysiological abnormalities in persons who had ARS and were irradiated in doses of 1–5 Gy could testify to the damage of the cortical-limbic system, mainly in the dominant (left) hemisphere. A frequency and intensity of these effects increased on proportion to the absorbed dose (1–5 Gy) that allows considering them as deterministic radiation effects. Quantitative electroencephaologram (qEEG) could be proposed as a powerful and beneficial tool for differentiation of radiation and nonradiation brain damages, as well as for the development of a promising new method for biological dosymetry, with reconstruction of absorbed dose on the basis of qEEG-parameters.
60 Utilizing more sophisticated EEG technologies (coherence analysis, source localization, cognitive evoked potentials etc.), along with neuroimaging, particularly, positron emission tomography (PET), is the most challenging approach for the radio-cerebral effects investigation.