While patients with cerebellar disease have exhibited a variety of cognitive and affective impairments,
10 their disordered executive functioning is particularly notable.
12 This broad category of cognition includes planning and anticipating; initiating, sustaining, and inhibiting activity, as situationally appropriate; generating ideas; inferring and deducing; judging and weighing options; acquiring and shifting mental sets; and related processes. These functions are often attributed to the prefrontal cortex, but they are perhaps more appropriately viewed as emerging from the integrated activity of a corticostriatothalamic “loop” and a cerebrocerebellar output channel.
13,14 Other cognitive impairments frequently reported among patients with cerebellar pathology include working memory and effortful recall of newly learned information.
15–17 A functional disconnection of the cerebellum from the cerebrum, especially from the prefrontal association cortex, is typically implicated in these impairments.
18Cerebellar dysfunction can result from stroke, tumor, trauma, or other pathophysiologic mechanisms. Of primary interest in this report are disorders causing primary cerebellar degeneration (CD). As used in this study, cerebellar degeneration encompasses conditions diagnosed clinically as olivopontocerebellar atrophy (OPCA; a subtype of multiple system atrophy) and familial spinocerebellar ataxia (SCA). These disorders are themselves quite heterogeneous.
19 For example, as many as 17 phenotypically similar, yet genetically distinct, autosomal dominant types of SCA have been identified to date.
20 However, in all of these conditions, the most striking neuropathological feature is extensive atrophy of the cerebellar hemispheres and vermis, along with varying degrees of degeneration of brainstem nuclei (especially the inferior olives, which project to both the cerebellar cortex and deep nuclei). In some of these disorders, mild to moderate atrophy of cerebral cortex and basal ganglia may be seen as well.
One limitation of the existing literature on cognitive impairments in patients with cerebellar disorders is that the patients studied have been compared typically to healthy, neurologically normal adults. Thus, it remains unclear whether the observed deficits are specific to patients with cerebellar lesions or whether they are also found in patients with other movement disorders having different underlying neuropathology. In the present study, the neuropsychological test performance of patients with CD is compared to that of patients with Huntington’s disease (HD). It is widely acknowledged that HD patients also suffer from a subcortical dementia and perform poorly on tasks requiring sustained attention, multiple simultaneous operations, planning, other aspects of executive functioning, and free recall.
21–23 Like CD, HD is characterized by an adult-onset movement disorder and, like several types of SCA, is caused by an expanded repeat mutation of the CAG triplet coding for glutamine. However, the cerebellum is usually unaffected in adult-onset HD.
24 In early- to mid-stage HD, neuropathology is restricted to the neostriatum. In late stage illness, there is widespread neuronal loss throughout the basal ganglia, thalamus, and cerebral cortex, but the cerebellum is typically spared.
25,26 Thus, a comparison of CD and HD patients, equivalent in age and severity and chronicity of movement disorder, may elucidate the unique contribution of cerebellar dysfunction to cognitive impairment.
METHODS
Subjects
Thirty-one patients with CD, 21 patients with HD, and 29 neurologically normal adults participated in this research. All subjects gave informed consent for their participation in the study, which was reviewed and approved by the Johns Hopkins Joint Committee on Clinical Investigation.
The CD patients were diagnosed and referred by faculty neurologists. A board-certified neurologist specializing in movement disorders (E.O.) verified all diagnoses based on clinical examination, brain imaging studies, and DNA analysis. Fifteen of the 31 CD patients had familial disorders, with the specific genetic etiology known in nine cases: two patients had SCA, type 1 (SCA1); two had SCA3; two had SCA6; and one patient each had SCA2, SCA7, and SCA8. In six familial cases, the genetic mutation was unknown. While the neuropathology of some of the SCAs extends beyond the cerebellum, the patients selected for the present study all had markedly prominent cerebellar signs and minimal evidence of extracerebellar disease. Among the 16 sporadic CD cases, five carried the diagnosis of cerebellar-predominant multisystem atrophy, and the remaining 11 had cerebellar degeneration of unknown etiology.
The HD patients were recruited from the Baltimore Huntington’s Disease Center at Johns Hopkins Hospital. They were diagnosed by experienced neuropsychiatrists (A.R. and R.L.M.) based on family history and clinical examination and confirmed by DNA testing for a triplet repeat mutation in the huntingtin gene. All HD patients had onset in adulthood and were symptomatic for at least 5 years.
For the CD and HD patients, the age at first signs of unambiguous motor impairment reported by knowledgeable family members (typically spouses) was considered the age of disease onset. Unaffected family members of CD and HD patients served as normal control subjects. None of these people had any history of neurological disorder.
Procedures
All patients and control subjects were evaluated neurologically, psychiatrically, and neuropsychologically, using standardized instruments and methods. The neurological evaluation included the Quantified Neurological Exam (QNE),
27 developed specifically for HD, and the International Cooperative Ataxia Rating Scale (ICARS).
28 In addition to a history and mental status exam, the psychiatric evaluation included administration of the Structured Clinical Interview for DSM-IV Axis I Disorders (nonpatient version)
29 and the Neuropsychiatric Inventory
30 and the completion of a number of symptom rating scales. (The psychiatric characteristics of the patients described in this report are described more fully elsewhere.
31)
The neuropsychological evaluation included administration of the North American Adult Reading Test (NAART),
32 Grooved Pegboard Test,
33 Brief Test of Attention,
34 Verbal Fluency (word-list generation guided by initial letter and semantic category),
35–37 Developmental Test of Visual-Motor Integration,
38 and Hopkins Verbal Learning Test—Revised (HVLT-R).
39,40 In addition, three experimental tasks were administered. The first of these was the Hopkins Board.
41 This is a brief, relatively culture-free test of learning and memory that yields measures of picture naming, learning efficiency, and delayed recall of both verbal and spatial information. The second experimental task was motivated by the finding that performing a difficult pegboard puzzle, the “Insanity Task,“ activates a major cerebellar output nucleus bilaterally.
4 We developed a somewhat simpler task, a modification of the Grooved Pegboard Test that added an executive, mental tracking component. After placing each peg, the patient had to alternate skipping one, two, or three holes before placing the next peg. We averaged the time to complete the 30-hole pegboard with the dominant hand and time to complete it with the nondominant hand. The final experimental task was Word Class Fluency. Motivated by the finding that the right lateral cerebellum is involved in rule-governed word (especially verb) production,
7,11,42 we asked patients to say as many verbs as possible in 1 minute, and as many adjectives as possible in 1 minute.
Statistical Methods
The demographic and clinical characteristics of the three groups were compared with one-way analysis of variance (ANOVA), with planned contrasts between the CD and HD groups. The neuropsychological tests yield a minimum of 15 conceptually important scores, and group means on these variables were subjected to one-way ANOVA, with post hoc Scheffé tests. For test variables where the assumption of homogeneity of variance was not met, the data were subjected to square-root transformation before the ANOVA was performed, and Tamhane’s T2 post hoc test was used. To reduce the probability of type I statistical error due to multiple comparisons, α for all comparisons was set at 0.01. (While the Bonferroni correction for multiple comparisons is often considered
de rigueur in clinical research, its uncritical use is based on the faulty notion that type II statistical errors [failing to detect a real difference between groups or conditions] are less problematic than type I errors. This is often not the case. A conservative α level is an easily justified compromise. See Rothman
43 for a fuller discussion of this issue.)
The ratio of subjects to variables did not allow a principal components or other formal latent structure analysis of the neuropsychological data. Therefore, the 15 neuropsychological variables were reduced a priori to five underlying domains (motor, verbal, spatial, memory, and executive). Prior to examining any of the collected data, a board-certified clinical neuropsychologist (J.B.) assigned each test variable to one or two of these domains based on his assessment of the importance of the underlying cognitive/behavioral function to test performance. To test the reliability of this assignment of test variables to domains, two other academic neuropsychologists independently performed the same assignment. Of the 150 decisions (15 variables × 5 domains × 2 raters), there was agreement with the author on 136 (91% agreement). The variables “loading“ on each domain are as follows: Motor: Grooved Pegboard, mean of dominant and nondominant hands; Grooved Pegboard, Skipping Version, mean of dominant and nondominant hands; Developmental Test of Visual-Motor Integration, number correct. Verbal: Hopkins Board, number correctly named; Hopkins Board, delayed recall of items; Initial Letter Fluency, sum of three trials; Category Fluency, sum of three trials; Word Class Fluency, verbs; Word Class Fluency, adjectives; HVLT-R, sum of three learning trials; HVLT-R, percent retained on delayed recall; HVLT-R, recognition discrimination index. Spatial: Hopkins Board, trials to criterion; Hopkins Board, delayed recall of locations; Developmental Test of Visual-Motor Integration, number correct. Memory: Hopkins Board, trials to criterion; Hopkins Board, delayed recall of items; Hopkins Board, delayed recall of locations; HVLT-R, sum of three learning trials; HVLT-R, percent retained on delayed recall; HVLT-R, recognition discrimination index. Executive: Grooved Pegboard, Skipping Version, mean of dominant and nondominant hands; Brief Test of Attention, number correct; Initial Letter Fluency, sum of three trials; Category Fluency, sum of three trials; Word Class Fluency, verbs; Word Class Fluency, adjectives.
For the patient groups, the deficit in each domain was quantified by averaging the estimated effect sizes for the test variables comprising the domain. The effect size statistic used was the partial η
2, derived from one-way ANOVAs comparing the means of the patient group to the normal control group.
44 Partial η
2 is the ratio of the sum-of-squares for the group effect to the group sum-of-squares plus the error sum-of-squares.
45 This statistic is interpreted as a squared correlation coefficient: the estimated percent of variance in the dependent variable (neurocognitive domain score) that can be accounted for by the independent variable (group). The analysis of effect sizes allows us to examine the
magnitude of cognitive deficits in the CD and HD groups, not simply their presence (as indicated by the significance tests).
46,47RESULTS
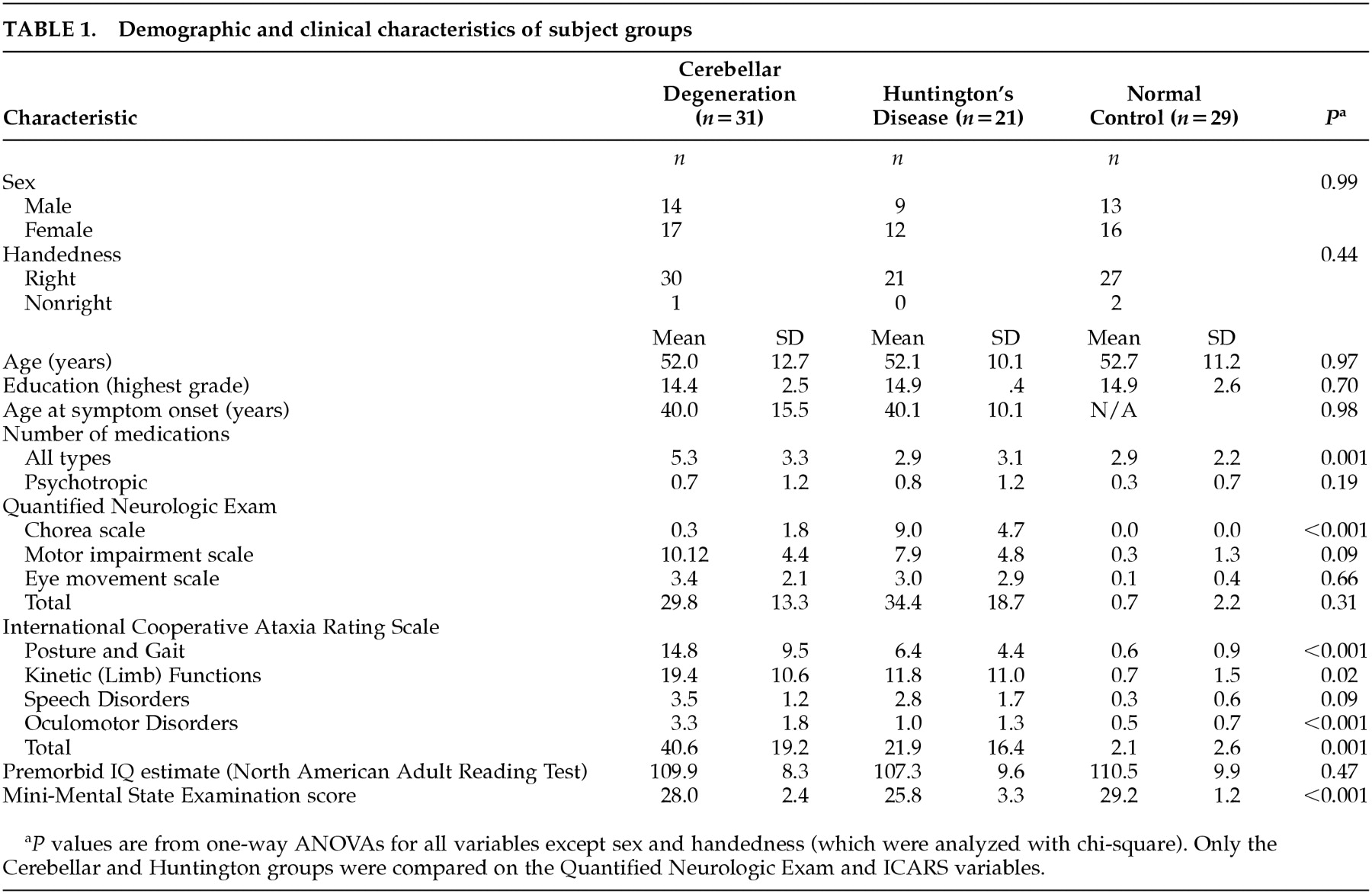
The three groups were comparable in age, sex distribution, and educational level (
Table 1). Age at disease onset was very similar for the two patient groups.
The CD and HD groups had equivalent scores on the QNE. The only component of the QNE on which the two patient groups differed was the chorea scale, which was significantly higher in the HD group. There were significant differences between the CD and HD groups on the ICARS. The CD patients had greater ataxia on all the ICARS components except the speech subscale. As a group, the CD patients were taking more medications than the HD patients or normal control subjects, but this was not the case for psychotropic medications.
The three subject groups performed very similarly on the NAART (
Table 1). This finding, combined with the equivalence in education among the groups, suggests that they were of comparable premorbid intellect. On the Mini-Mental State Examination (MMSE), the groups differed markedly, with the HD group impaired relative to both the CD group (
p= 0.006) and the normal control group (
p<0.001). The MMSE scores of the CD and normal control group were not appreciably different.
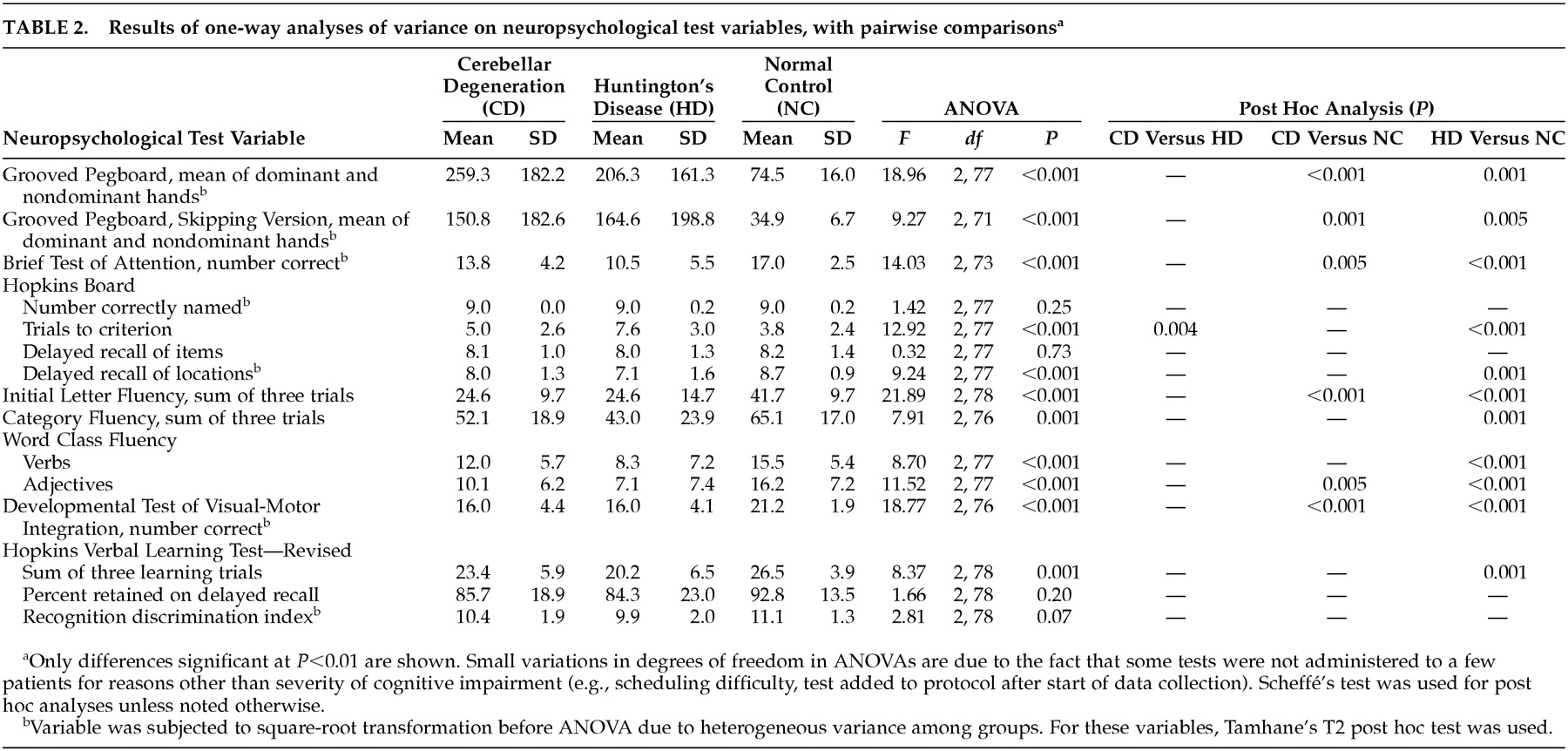
There were significant differences among the three groups (
p<0.01) on 11 of the 15 neuropsychological test variables (
Table 2). Post hoc tests revealed that the group effect was due, in most cases, to the HD patients performing worse than the normal control subjects. The CD patients performed more poorly than normal subjects only on the Grooved Pegboard Test (both versions), Brief Test of Attention, Verbal Fluency (initial letter), Word Class Fluency (adjectives), and the Developmental Test of Visual-Motor Integration. The two patient groups differed significantly only on the number of trials to learning criterion on the Hopkins Board. On this measure of spatial learning, HD patients were clearly impaired (
p<0.001), while CD patients performed as well as normal subjects.
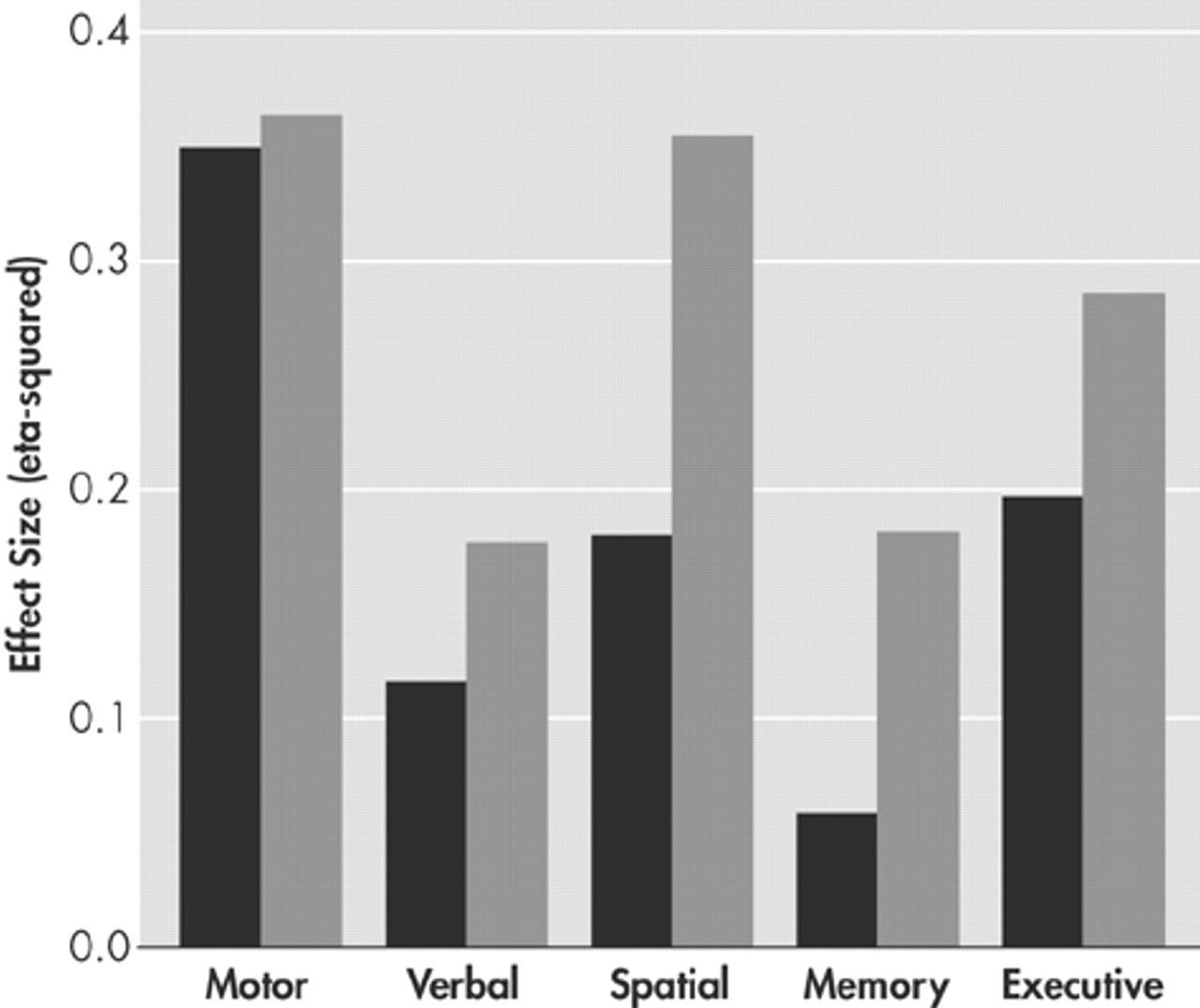
The magnitude of impairment in each of the five neurocognitive domains was estimated for each patient group by averaging the effect sizes for the test variables comprising those domains. As seen in the
Figure, the two patient groups were equally impaired, vis-à-vis the normal subjects, on the tests comprising the motor domain. In the other four domains, the CD patients displayed only mild deficits, with effect sizes ranging from a low of 0.057 in the memory domain to a high of 0.195 in the executive domain. The HD patients displayed more substantial impairments, with effect sizes ranging from a low of 0.177 in the verbal domain to 0.352 in the spatial domain.
DISCUSSION
The first major finding of this study is that groups of CD and HD patients with equivalent durations of illness have comparable degrees of overall motor impairment. Whereas ataxia was rated as more severe in the CD patients, and chorea was more severe in the HD patients. The total QNE scores of the groups did not differ. In addition, both groups were severely but equivalently impaired in the motor component of the neuropsychological tests employed in this study.
The second finding is that the cognitive impairment of CD patients, ill for an average of 12 years, is relatively mild. Whereas demographically matched HD patients obtained lower than normal scores on 11 of 15 neuropsychological test variables, CD patients with equivalent lengths of illness and overall motor impairment were impaired on only six. In addition, group membership accounted for, at most, 20% of the variance in performance among CD patients and control subjects (in the executive domain). In contrast, group membership accounted for up to 35% of the variance in performance among HD patients and control subjects (in the spatial domain).
Several previous studies have also reported minimal cognitive impairment in CD. In one, OPCA patients, who were ill for an average of 6 years, performed cognitive tests as well as education-matched normal subjects.
48 In another study, 43 mildly ataxic SCA patients, ill for an average of 11 years, performed almost normally on a battery of neuropsychological tests.
17The third major finding is that the
pattern of impairment in CD is different from that in HD. In the present study, CD patients had their most substantial impairment in executive function, but negligible impairment in new learning and memory. This contrasts with the profile of HD patients, who had marked spatial deficits in addition to executive impairment and much more prominent memory deficits.
49–51Severe executive dysfunction in patients with cerebellar pathology has been observed using the Tower of Hanoi task
12 and the Tower of Toronto task.
11 These tasks, and variations of them, have become favorite measures of problem-solving among cognitive neuroscientists.
52,53 Efficient solution requires the subject to develop a strategy for reaching a goal and to carry out that plan of action through a series of moves. Many of the critical moves are counterintuitive and require the subject to inhibit what may be a prepotent response. Although each problem has a different initial state, and hence a different “path” to its correct solution, optimal performance is achieved by discerning successive subgoals and carrying out a recursive sequence of moves. Patients with pure cerebellar atrophy have been found to solve fewer Tower of Hanoi puzzles and make more rule violations than normal subjects.
12 An individually reported case of right cerebellar stroke had an intelligence quotient (IQ) of 131 and a Wechsler Memory Scale (WMS) Memory Quotient of 124, but scored four standard deviations below normal on the Tower of Toronto task.
11 Although this patient’s performance improved across blocks of trials, his errors at critical choice points belied the fact that he was not consistently following a recursive rule. Other evidence of marked executive dysfunction in cerebellar patients has been provided by both bedside mental status testing and formal neuropsychological assessment.
10Our finding of minimal memory impairment in CD patients is consistent with some previous studies, but not others. When 11 OPCA patients from a single pedigree were studied using standardized cognitive tests, they were found to be most impaired on the recall of stories read to them. The mean score of these patients on the WMS Logical Memory subtest was 46% that of normal control subjects.
16 This same research team later reported mild memory deficits (low scores on WMS Mental Control and Logical Memory subtests, and WMS Memory Quotient) among SCA patients with moderate ataxia and more pervasive memory and cognitive deficits (though no aphasia) among those with severe ataxia.
17In one of the most comprehensive studies of cognition in cerebellar patients to date, a large number of clinical and experimental tests of explicit memory were administered to 11 patients with isolated cerebellar degeneration.
15 The patients performed more poorly than normal control subjects on the Dementia Rating Scale
54, word-list generation tasks, and effort-demanding tests of memory: free recall of word lists and paired-associate learning using both word and picture stimuli. Importantly, the patients were not impaired on tasks requiring less effort: cued recall and yes/no recognition.
55 Similarly, the cerebellar patients were unimpaired in their incidental monitoring of frequency of occurrence or modality of stimulus presentation, two measures of automatic cognitive processing.
56 These same investigators also studied implicit memory and found that cerebellar patients and normal control subjects displayed equivalent improvement over trials on both a word fragment completion test and an identification of incomplete pictures test. The conclusions drawn from these results were that 1) only attention-demanding cognitive processes are impaired by cerebellar pathology; and 2) this variety of executive dysfunction is responsible for the apparent memory impairment of these patients.
The severity and pattern of impairments seen in our CD and HD patients may be appreciated in light of the circuitry linking of the cerebellum and basal ganglia to the cerebral cortex.
13,14,57 The dentate nucleus, the deep output nucleus of the cerebellar hemispheres, sends projections via the thalamus primarily to frontal cortex, including primary motor and premotor areas (areas 4 and 6), the frontal eye fields (area 8), and dorsolateral prefrontal cortex (areas 9 and 46). These latter regions of association cortex are critically involved in directed attention, working memory, planning, and other executive functions. Thus, motor and executive functions might be expected to be most impaired in CD patients. The basal ganglia, on the other hand, have somewhat more widespread cortical linkages. These include reciprocal connections with orbital frontal cortex (area 12), an area important in risk-taking and decision-making;
58,59 inferotemporal cortex (area TE), an area critical for visual object recognition and associative memory;
60,61 and posterior parietal cortex (area 7), an area important in spatial operations.
57,62,63 Disruption of the cortical-striatal circuits involving parietal and temporal neocortex may underlie our finding that spatial cognition and memory are more significantly impaired in HD than in CD.
Of course, it is possible that using more or different tests of these cognitive functions might reveal more striking impairments in CD patients. While a different assignment of tests to cognitive domains may also result in a different pattern of impaired and spared functioning, we consider our assignment relatively conservative and noncontentious. Finally, since the CD patients were taking more medications than the HD patients, yet had milder cognitive impairments, it is unlikely that medication effects are a significant contributor to our findings.
The heterogeneity of our CD group, composed of patients with several phenotypically similar but genotypically distinct disorders, limits our ability to make strong neuropathological inferences from our neuropsychological data. Future research with larger, more homogeneous samples, who are studied with quantitative neuroimaging as well as neurocognitive procedures, will allow more definitive conclusions to be drawn about the role of specific cerebellar and extracerebellar mechanisms in the mental functioning of CD patients. In the meantime, clinicians and caregivers of patients with cerebellar disease are advised to appreciate that mild impairment of executive functioning is common in these patients and any apparent forgetfulness or memory impairment is probably secondary to impaired executive control.
ACKNOWLEDGMENTS
The authors thank Stephen Grill, M.D., Ph.D., Hyder Jinnah, M.D., Ph.D., Stephen Reich, M.D., and Christopher Ross, M.D., Ph.D., for evaluating, diagnosing, and referring patients; Cynthia Munro, Ph.D., and David Schretlen, Ph.D., for help establishing the reliability of the neuropsychological domain assignments; Ms. J. Kathleen Tracy for testing the participants; and Mss. Caroline Blau and Christine Liszewski for program coordination and data management. This research was supported by NIH grants NS-16375 and RR-00052 and a grant from the National Association for Research on Schizophrenia and Affective Disorders.