H yperactive and hypoactive motor presentations of delirium were described as far back as in Ancient Greece where these patterns were termed “phrenitis” and “lethargicus,” respectively.
1 In more contemporary literature, three patterns—hyperactive, hypoactive, and mixed according to a wide variety of psychomotor symptoms—are recognized, though quantification, severity, and specificity of these symptoms in delirium have not been adequately studied. Psychomotor subtypes are often assessed using checklists of psychomotor symptoms without clear cutoffs for symptom severity or specificity. There are three often-cited delirium psychomotor checklists,
2 –
4 while other studies used pure motor items from a standardized delirium rating scale such as the Memorial Delirium Assessment Scale, the Delirium Rating Scale, or a visual analogue scale to identify motor subtypes.
5 Studies using these various methods have identified widely varying subtype category frequencies and indicate that hyperactive, hypoactive, and mixed delirium subgroups may differ regarding their relationships to nonmotor symptoms,
6 –
8 etiology,
6,
9,
10 pathophysiology,
11,
12 detection rates,
13 delirium treatment experience,
14 –
16 episode duration, and outcome.
3,
4,
17 –
19 However, findings have been inconsistent due to differing delirious patient populations, a lack of validated rating instruments with no clear cutoff values for symptom presence or severity, and further obfuscation of phenomenology by inclusion of many nonmotor symptoms that have uncertain value in motor subtyping (e.g., irritability, aggressive behaviors, and screaming).
20 Many psychomotor symptoms are easily observable clinically and may pose considerable management problems, but whether they denote a physiologically or clinically meaningful subtype of delirium is not well substantiated. While EEG diffuse slowing and severity of cognitive impairment were comparable in hyperactive and hypoactive patients when levels of motor activity were measured on a visual analogue scale,
9 other work suggests pathophysiological differences according to motor profile.
11,
12 Little work has been done in delirium using objective motor activity monitoring and none which correlated subjective to objective ratings.
To better understand the differences among subjective approaches, Meagher et al.
21 compared delirium subtypes categorized using three subtyping schema
2,
3,
4 and the motor items of the Delirium Rating Scale-Revised-98. When simultaneously applied in a single delirious population, the study found only 34% concordance. Further, when nonredundant items from these three psychomotor schema were combined to form the 30-item Delirium Motoric Checklist, only 6 of 22 nonmotor symptoms differed (after Bonferroni correction) between delirium patients and comparison subjects, suggesting nonspecificity for delirium.
6 Importantly, when just “pure” motor checklist items were analyzed, delirious patients showed significantly more impairment than nondelirious comparison subjects in the same clinical setting, suggesting that motor symptoms may carry specific phenomenologic significance in delirium, in addition to core cognitive symptoms, and therefore deserve further study. This is consistent with other work showing that motor activity impairments are almost invariably present in delirium.
22,
23In this report we extended our analyses of a recently studied population in order to obtain a more in-depth phenomenological understanding of psychomotor symptoms. We applied principal components analysis to the Delirium Motoric Checklist data to determine phenomenological domains and examined the frequency and correlation of the 30 items from the checklist in relation to an independent rating of motor activity levels and specificity for delirium as compared to nondelirious comparison subjects. Finally, we developed a new subtype scale from suitable items and back-applied it to identify subtype frequency and clinical characteristics in a population with DSM-IV delirium.
METHOD
Design and Subjects
We conducted a prospective cross-sectional descriptive study of psychomotor phenomenology in 100 consecutive cancer patients with DSM-IV diagnosed delirium admitted to a palliative care center in Limerick, Ireland. Patient identification and assessment methods are described in a previous report.
23 Patients with DSM-IV delirium were assessed for delirium symptoms over the preceding 24 hours using the Delirium Rating Scale-Revised-98
22 and for cognitive performance with the Cognitive Test for Delirium.
24 Staff nurses completed the Delirium Motoric Checklist independent of the research psychiatrist assessment for the same 24-hour period. Demographics, psychotropic drug exposure at the time of assessment, and the possibility of underlying dementia (noted in case history or suggested by investigation) were also collected.
A group of nondelirious comparison subjects (N=52) matched for approximate age, medical diagnosis, and medication use, who were receiving treatment in the same setting as the delirious cohort, were assessed using the Delirium Motoric Checklist to determine the frequency of motor symptoms for a 24-hour period.
Delirium phenomenology and severity were assessed using the Delirium Rating Scale-Revised-98 (DRS-R98); which was designed for phenomenological assessment using anchored descriptive item ratings on Likert scales (13 that comprise the severity scale plus three diagnostic items).
22 It has high interrater reliability, validity, sensitivity, and specificity for distinguishing delirium in mixed neuropsychiatric populations including dementia, depression, and schizophrenia.
22 DRS-R98 severity scale scores range from 0–39 with higher scores indicating more severe delirium and a cutoff score ≥15 consistent with a diagnosis of delirium. Two items of the DRS-R98 specifically assess motor presentation (item 7—agitation, item 8—retardation) and were used as an independent measure for “pure” motor disturbance or “gold standard” assessed by the research clinician (DM, MM, or BE) who was blind to other ratings of motor profile (Delirium Motoric Checklist).
Features from three published psychomotor subtyping schemas
2,
3,
4 were combined to form a new 30-item Delirium Motoric Checklist, without redundant items. Each item was rated as 1-present or 0-absent during the previous 24 hours by the key nurse responsible for the patient at the time of assessment.
Cognitive function was assessed with the Cognitive Test for Delirium,
24 which includes five neuropsychological domains: orientation, attention, memory, comprehension, and vigilance. Scores range from 0 to 30 with higher scores indicating better cognitive function. The Cognitive Test for Delirium reliably differentiates delirium from other neuropsychiatric conditions including dementia, schizophrenia, and depression.
25Informed Consent
The procedures and rationale for the study were explained to all patients; however, because patients had DSM-IV delirium at study entry it was presumed that most were incapable of giving informed written consent. Because of the noninvasive nature of the study, ethics committee approval was given to augment patient assent with proxy consent from next of kin (where possible) or a responsible caregiver for all participants, in accordance with the Helsinki, Finland, guidelines for medical research involving human subjects.
Statistics
Statistical analyses were conducted using SPSS Version 10.1. Continuous variables for demographic and Delirium Rating Scale-Revised-98 (DRS-R98) data are expressed as means and standard deviations. Items from the Delirium Motoric Checklist were entered into a principal components analysis to identify the factor structure of psychomotoric symptom profile in delirium. Pearson’s product-moment correlation values were used to explore the correlation between these factors and independent ratings of agitation (DRS-R98 item 7) and retardation (DRS-R98 item 8). Items with a loading of >0.65 onto the principal two factors were extracted to make a subtyping scheme. Fisher’s exact test was used to compare frequency of individual items on the checklist between delirious patients and nondelirious comparison subjects and to compare scores for DRS-R98 items 7 and 8 between patients with and without each of the individual checklist items (see
Table 1 and
Table 2 ). One-way analysis of variance (ANOVA) was used to compare mean scores on DRS-R98 and Cognitive Test for Delirium for the four subtypes. Where multiple comparisons were made, a Bonferroni correction using significance levels of p<0.001 was applied.
RESULTS
Subjects
The 100 delirium patients (50 male; mean age 70.1±11.5 years, range=33–91) had a mean DRS-R98 severity score of 16.1 (95% CI=15.1–17.4). Seventeen cases had documented preexisting cognitive deficit. The nondelirious comparison subjects were 54% male with a mean age (66.1±10.8 years) somewhat younger than the delirious group (t=2.06, p=0.04).
All delirious patients were receiving medications with a median of six medications per patient (range=1–16). Of these, 91% were receiving at least one psychotropic or psychoactive agent—benzodiazepines (79%), antipsychotics (43%), antidepressants (31%), opiates (72%), corticosteroids (45%), and psychostimulants (6%). The only significant relationship between category of medication and motor profile was that patients receiving psychostimulants had higher scores on the DRS-R98 retardation item (p=0.03) than those who were not.
Medication exposure was similar in the nondelirious comparison group with a median of six medications per subject (range=2–12). The frequency of use of specific agents was not different between delirious patients and nondelirious comparison subjects—benzodiazepines (71%); opiates (60%); corticosteroids (31%); and psychostimulants (6%)—apart from a trend (p=0.06) for less use of antipsychotics (27%) and significantly less antidepressant use (15%) in comparison subjects (p=0.03).
Delirium Motoric Checklist Items in Delirious Patients Versus Nondelirious Comparison Subjects
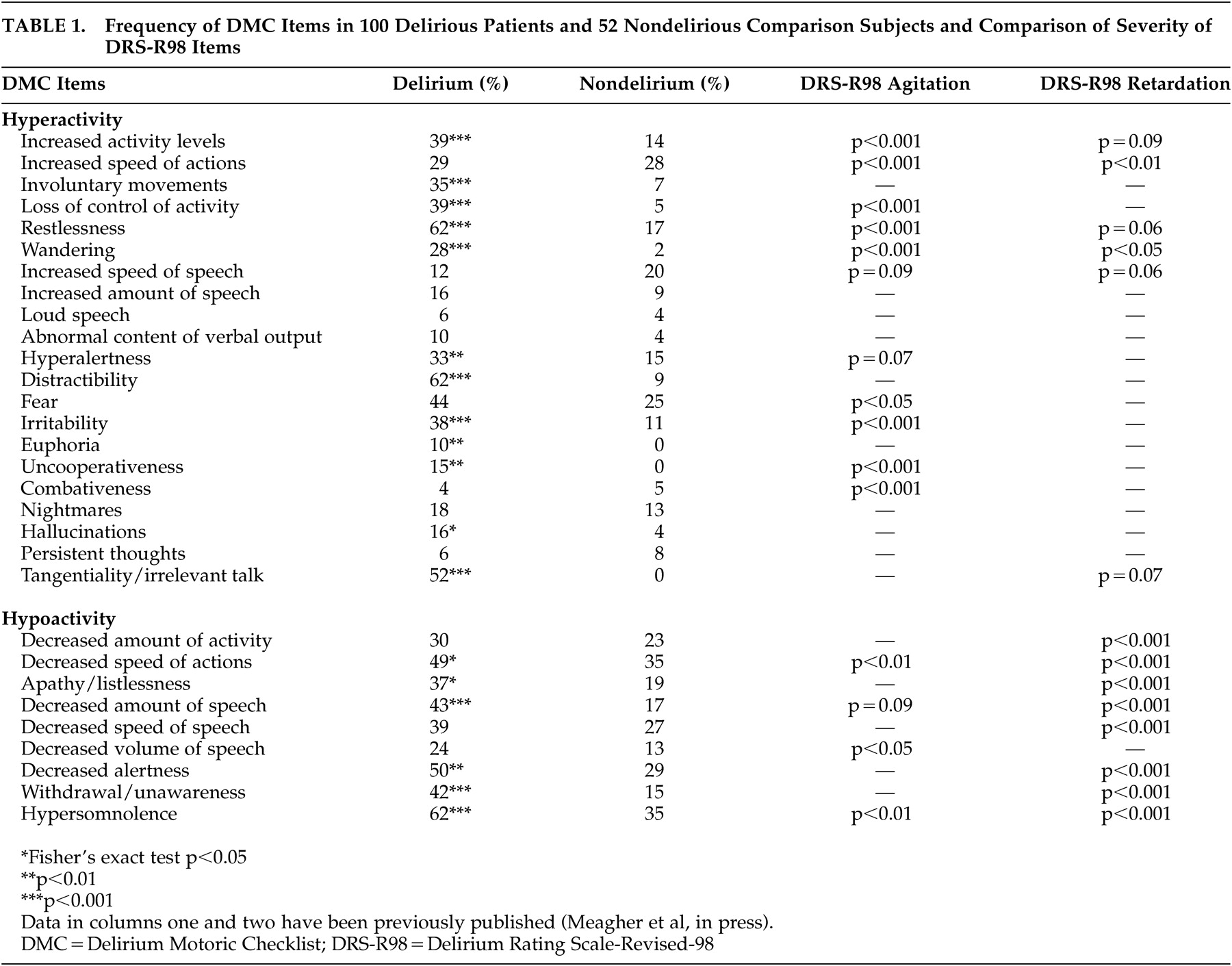
The frequency of motor disturbances in delirium patients and nondelirious comparison subjects using the Delirium Motoric Checklist is shown in
Table 1 . Every delirious patient had evidence of at least some psychomotor disturbance and 76 had evidence of both hyperactive and hypoactive features. However, when considering only “pure” checklist motor features, 92 had motor disturbance (75 hyperactive, 51 hypoactive, including 34 with both). Eighteen items on the checklist were more frequent in delirious patients at p<0.05 level of significance, and after correction for multiple comparisons, 15 items had p<0.01 level and 11 items had p<0.001 level.
In contrast, motor disturbances were less frequent in nondelirious comparison subjects. Although 75% had psychomotor disturbances rated with the Delirium Motoric Checklist, only 33 had evidence of “pure” motor disturbance (15 hyperactive, 19 hypoactive, and only with one both). Overall, motor disturbances were less common in nondelirious than delirious patients (median total checklist score 3 versus 9, respectively, p<0.001; median total hyperactivity score 0 versus 5, p<0.001; and median total hypoactivity score 1.5 versus 3, p=0.001).
Table 1 also shows the frequency of individual psychomotoric disturbances in nondelirious comparison subjects. Although “pure” hyperactive symptoms were more common in delirious patients, many symptoms lack specificity for delirium. Hypoactive features, in particular, are also common in cancer patients without delirium (e.g., reduced speed of actions and hypersomnolence) and were noted in over a third of the comparison subjects. Disturbances of speech (except for reduced amount of speech) did not occur significantly more often in delirious patients compared to nondelirious comparison subjects, nor did many affective (e.g., fear), behavioral (e.g., combativeness), or perceptual disturbances (e.g., hallucinations).
Principal Components Analysis
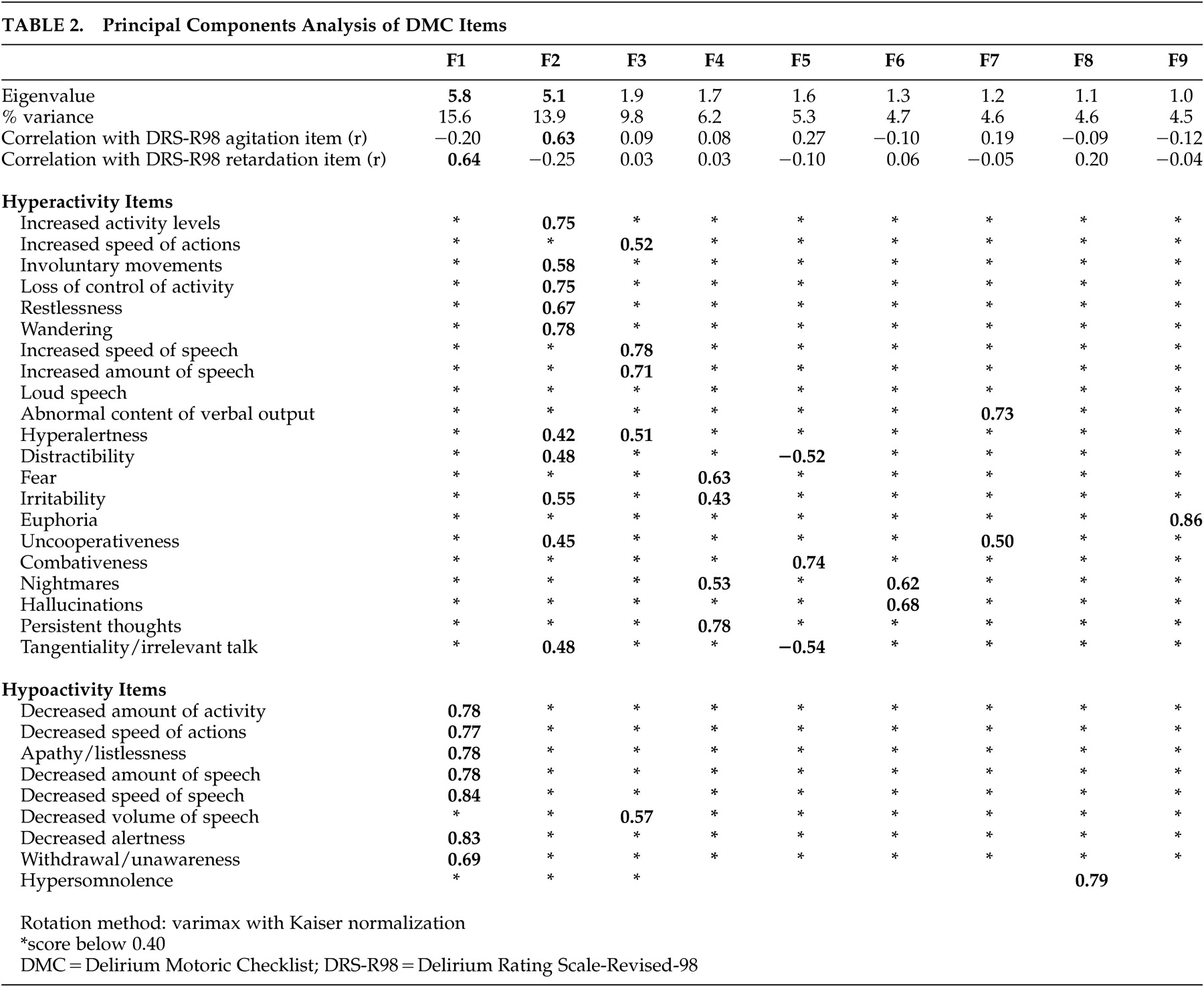
When the 30 Delirium Motoric Checklist items were entered into a principal components analysis, nine separate factors with eigenvalues greater than 1 were identified (see
Table 2 ). Factor 1 (5.8) and Factor 2 (5.1) had the highest eigenvalues. Factor 1 loaded nearly all of the checklist hypoactive items except for hypersomnolence, which loaded alone onto Factor 8, and decreased volume of speech, which loaded onto Factor 3 with some other items including hyperactive speech items. Factor 1 strongly correlated (p<0.001) with the DRS-R98 motor retardation item (r=0.64). Factor 2 loaded 10 hyperactive checklist items and correlated significantly (p<0.001) with the DRS-R98 agitation item (r=0.63). No other factors correlated with the DRS-R98 with such high r values. Other factors encompassed many nonmotor items from the Delirium Motoric Checklist.
The symptoms that loaded most strongly onto Factor 1 were decreased amount of motor activity, decreased amount and speed of speech, reduced speed of actions, listlessness, reduced alertness, and withdrawal/unawareness, all of which have a motor component except alertness. Interestingly, somnolence, which is more related to sleepiness, did not load onto Factor 1. Symptoms that loaded onto Factor 2 were increased activity levels, presence of involuntary movement, loss of control of activity, restlessness, and wandering as motor features, and hyperalertness, distractibility, irritability, uncooperativeness, and tangential/irrelevant talk as nonmotor features.
Process for Determining Subtype Criteria
The items comprising Factor 1 and Factor 2 were considered as candidate features for motor subtypes of delirium. Next, these items were assessed according to their specificity for delirium (compared with nondelirious comparison subjects) and sensitivity for motor features as measured by relationship to DRS-R98 items 7 and 8 (outlined in
Table 1 ). Items were included as subtype criteria if they (a) loaded >0.65 onto either Factor 1 or Factor 2 and
either (b) were significantly (p<0.001) more frequent in delirious versus nondelirious comparison subjects
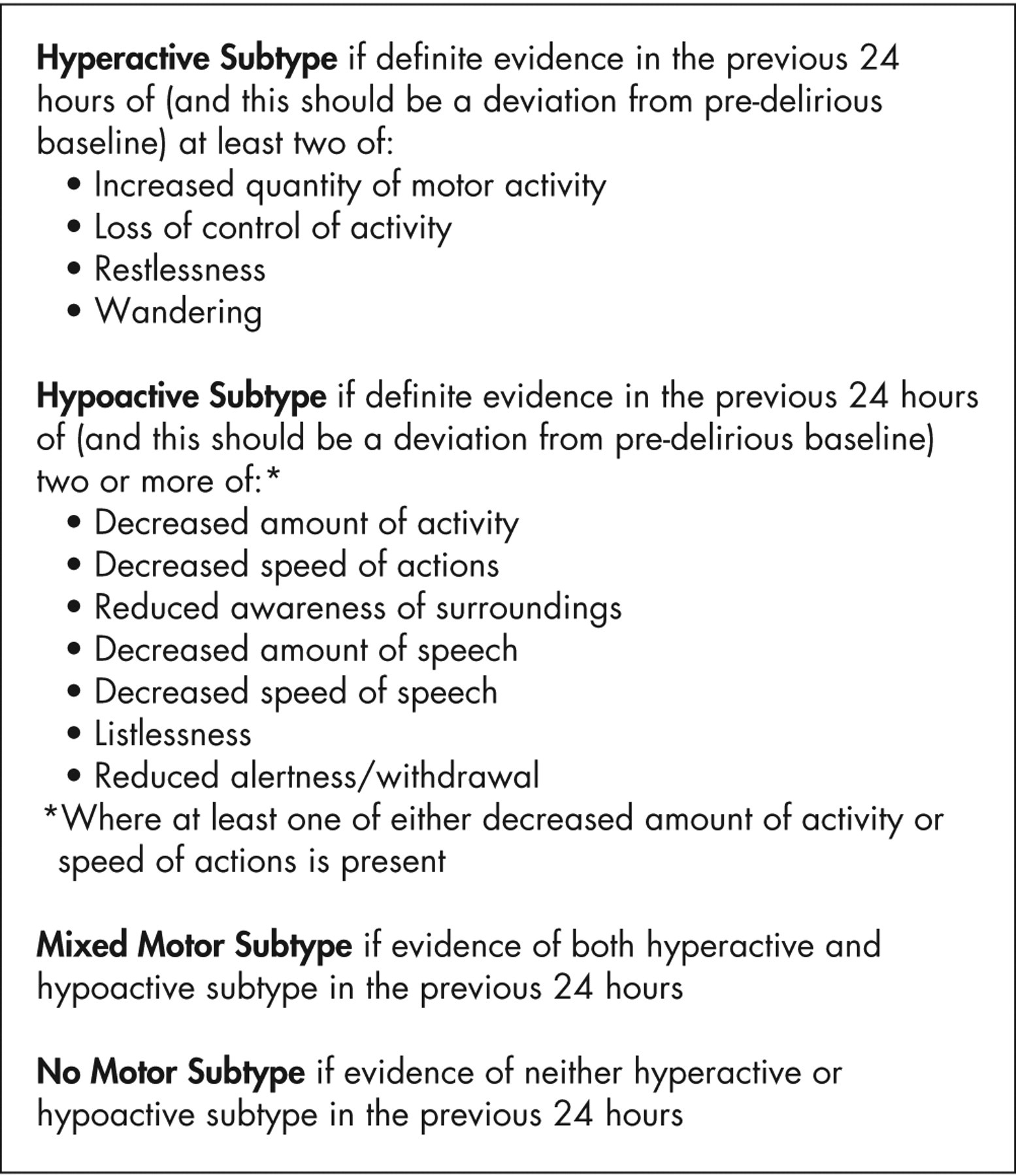
or (c) were associated with significantly greater scores on the DRS-R98 items for either agitation or retardation (p<0.001). From these findings seven hypoactive features and four hyperactive features were included (see
Figure 1 ). Of these, all four hyperactive features were “pure” motor features while two hypoactive items were pure motor features. In order for a patient to be classified with a motor subtype it was considered important that there be evidence of pure motor disturbance. Therefore a further criterion was added for the hypoactive subtype—the presence of at least hypoactive item 1 or item 2 (i.e., reduced amount of activity and reduced speed of actions, respectively).
Checklist Cutoff Determination
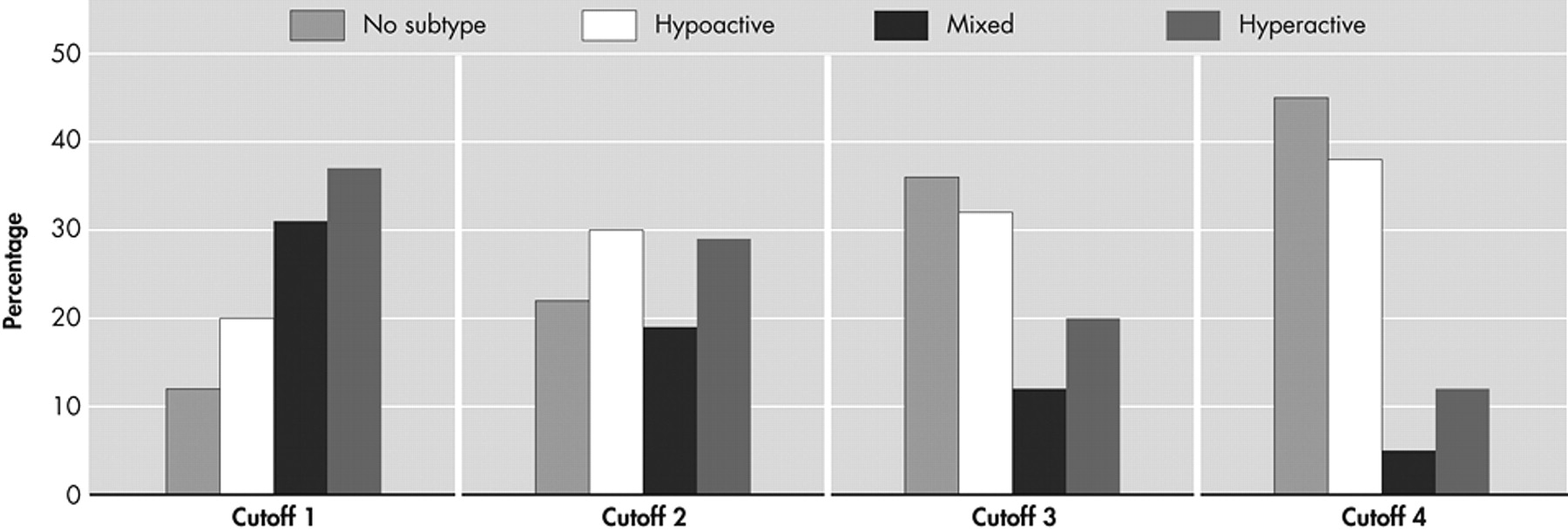
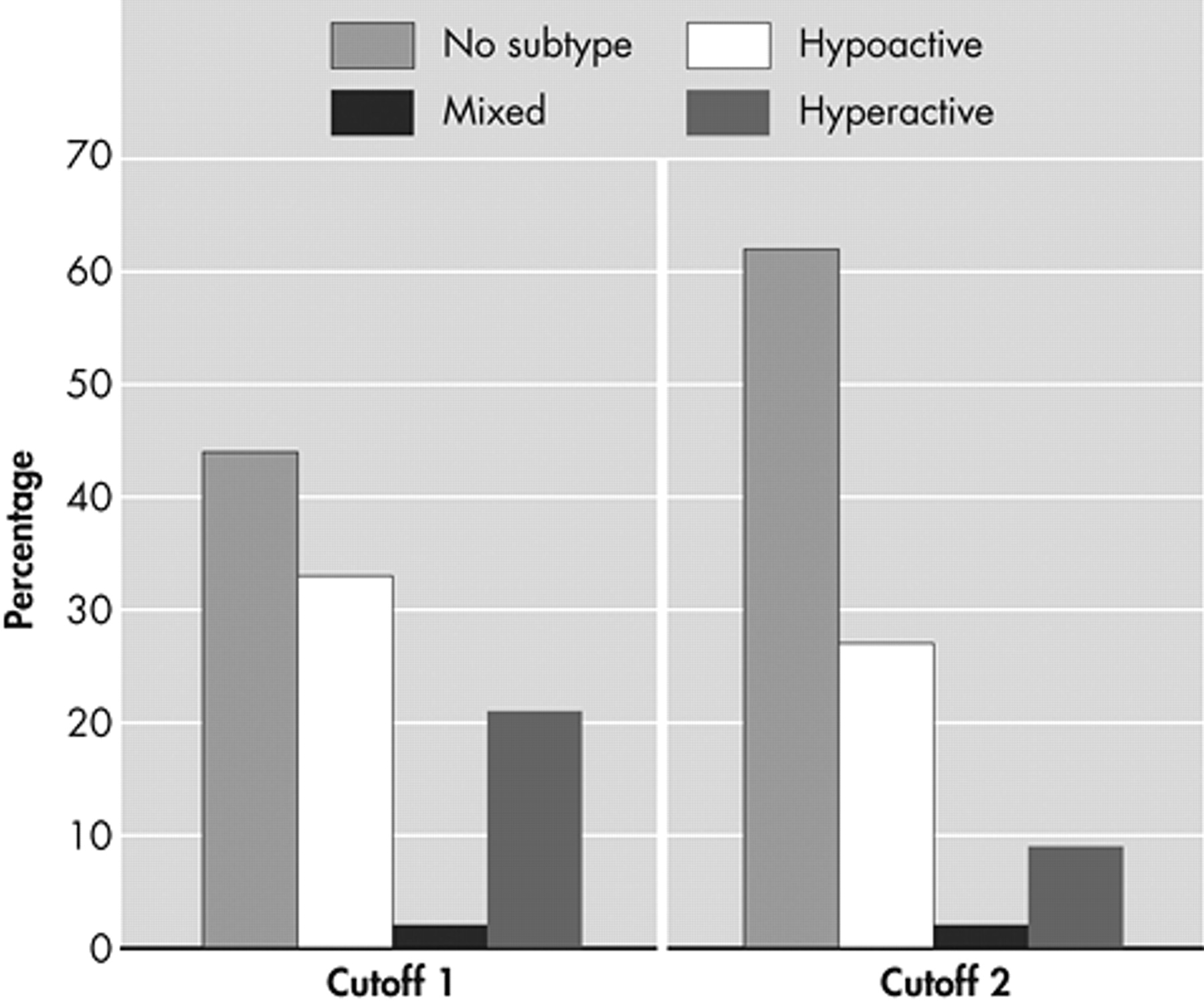
The allocation of a cutoff point for subtyping using this new checklist was explored by identifying the frequency of motor subtypes when applied back to this same population of delirious patients and comparison subjects. Different cutoff criteria were applied for the number of features needed to determine the presence of motor subtypes (see
Figure 2 and
Figure 3 ). When a cutoff of one symptom was used, the majority of delirious patients met criteria for a motor subtype (88%), but the majority of nondelirious comparison subjects also met subtype criteria (56%). When a cutoff of two symptoms was required, 78% of delirious patients met subtype criteria and most nondelirious comparison subjects did not (61%). When a cutoff of three symptoms was required, 36% of delirious patients did not meet subtype criteria; this increased to 45% when four symptoms were required. In view of these findings, a cutoff of two symptoms was considered to allow best inclusiveness for delirious patients while also providing relative specificity for delirium.
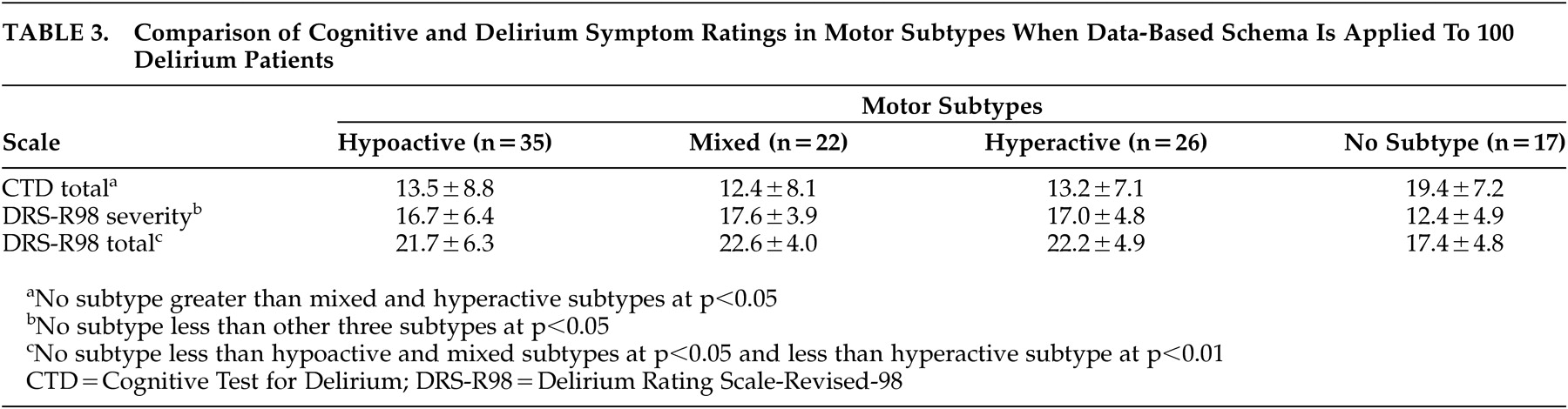
Using the new scale with a cutoff of a minimum two symptoms present, the 100 delirious patients were allocated to motor subtypes, resulting in 30 hypoactive, 29 hyperactive, 19 mixed, and 22 without subtype. Delirium severity and cognitive performance scores were compared between these subtypes (
Table 3 ). Patients labeled “no motor subtype” had significantly lower DRS-R98 severity scores (p<0.01) and significantly better cognitive performance, measured as total Cognitive Test for Delirium score (p<0.05).
DISCUSSION
The purpose of this study was to identify a motor subtyping schema for delirium derived from existing schema by identifying features that best relate to altered activity levels in delirium. This schema can provide a more consistent approach to defining motor subtypes in future work and allow for greater comparability of studies. A major difficulty with previous approaches to subtyping is their reliance on a range of psychobehavioral disturbances that are of uncertain relevance to actual motor activity levels (e.g., perceptual and affective disturbances). One way to reduce the impact of such features is to limit subtyping to an objective quantitative level of activity alone and ignore associated features that suggest motor disturbance. The difficulty with such an approach is that the absolute quantity of motor activity alone is substantially impacted by multiple confounders, such as the level of physical morbidity and exposure to medications. As such, accounting for the complexity of motor disturbances in delirium requires a subtyping schema that combines quantity and speed of activity with other associated features that reflect motor disturbance and are relatively specific for delirium. In this work, principal components analysis explored the interrelationship between these features to assist in formulating an appropriate description of motor subtypes, and features were selected according to their specificity for delirium and their relationship with an independent assessment of motor activity provided by Delirium Rating Scale-Revised-98 (DRS-R98) items 7 and 8.
We describe an approach to subtyping that derives from features that have been accumulated over many years of clinical observation in patients with delirium, though it does not include nondelirious comparison subjects in the same environments. We added measures of specificity for delirium and correlated with independent measures of motor function on a validated instrument designed specifically for delirium assessment. The resulting scale is relatively simple and based on a checklist that can be rated by nursing staff. Most patients fell into one of the three categories, and patients of no motor subtype tended to have less severe (even questionable) delirium as rated by severity of disturbances noted on the DRS-R98 and the Cognitive Test for Delirium, suggesting that the scale relates closely to the prevailing concept of delirium. It is hoped that the use of this scale in future studies of motor subtypes in delirium will allow for greater precision and consistency than is allowed by the present body of work.
Previous studies that have compared the relative frequency of nonmotor symptoms between different motor subtypes have identified significant differences in the frequency of psychosis with a similar severity of overall cognitive impairment.
8 However, cognitive profile has not been compared for individual domains of neuropsychological function, which is thus an important issue for future work.
This work has limitations. The palliative care group studied was highly morbid and, in many cases, in the terminal phase of illness. The high exposure to medications that can impact significantly on the motor profile of delirium means that the use of a comparison group is an important aspect of this work. Nevertheless, it should be appreciated that palliative care populations, such as those studied herein, typically have high levels of hypoactivity
23 that impacts the frequency of hyperactive features and also the motor profile of the nondelirious comparison group. As such the principal components analysis was used as the primary means to detect items suitable for subtyping with the additional requirement of
either significantly greater frequency versus comparison subjects (indicating relative specificity)
or a significant relationship to severity of motor disturbance measured on DRS-R98 motor activity items (a measure of sensitivity to motor disturbance). The further requirement—to meet subtype criteria patients must have evidence of at least one “pure” motor feature—reduced the likelihood that a patient was incorrectly subtyped due to the presence of nonspecific disturbances of motor profile. Further work involving delirium in a range of clinical populations (e.g., general hospital inpatients, geriatric admissions) is required before these observations can be confidently extended to include delirium in general.
The cross-sectional design limits the interpretation of these findings. To date there are no published data relating to longitudinal course of motor subtypes and, as such, little is known about the evolution of individual symptoms as well as actual motor subtypes over time. Lawlor et al.
26 suggest that subtypes are not stable over time but do not describe data to support this contention, while other studies suggest that hypoactivity as a symptom is more enduring.
27,
28 Although medication use was comparable across motor subtypes, a more detailed serial assessment including dose equivalents is needed to more clearly understand the influence of medication exposure on symptom profile.
The use of a separate measure of motor activity in the form of the independent rating with the Delirium Rating Scale-Revised-98 (DRS-R98) motor items is an important aspect of this work. This might be usefully extended to include actigraphic measurements as an objective “hard” measure of motor activity. To date, a single study has applied these methods to delirium and describes eight patients with concomitant dementia where different patterns of motor activity were distinguished.
29 Further work in patients with delirium uncomplicated by dementia and including the type of motor ratings included herein should further advance our understanding of motor disturbance in delirium.
Acknowledgments
The authors wish to acknowledge the support and cooperation of nursing and medical staff at Milford Hospice Palliative care centre. This study was supported through departmental funds at Limerick Mental Health Services. Unrelated to this research, Dr. Meagher has received research grant funding from AstraZeneca and has acted as a advisory consultant for Pfizer, Eli Lilly, Bristol-Meyers Squibb, and Janssen Pharmaceuticals, as well as receiving travel support from GlaxoSmithKline, Eli Lilly, AstraZeneca, Novartis, Wyeth, and Bristol-Meyers Pharmaceuticals Ltd. Dr. Trzepacz is a full-time salaried employee and shareholder of Eli Lilly and Company. Eli Lilly does not have a product with an indication for delirium. As of this time, Dr. Trzepacz has not received royalties for the use of her copyrighted Delirium Rating Scale-Revised-98, nor does she accept payment for teaching or academic research collaborations (including NIH grant).