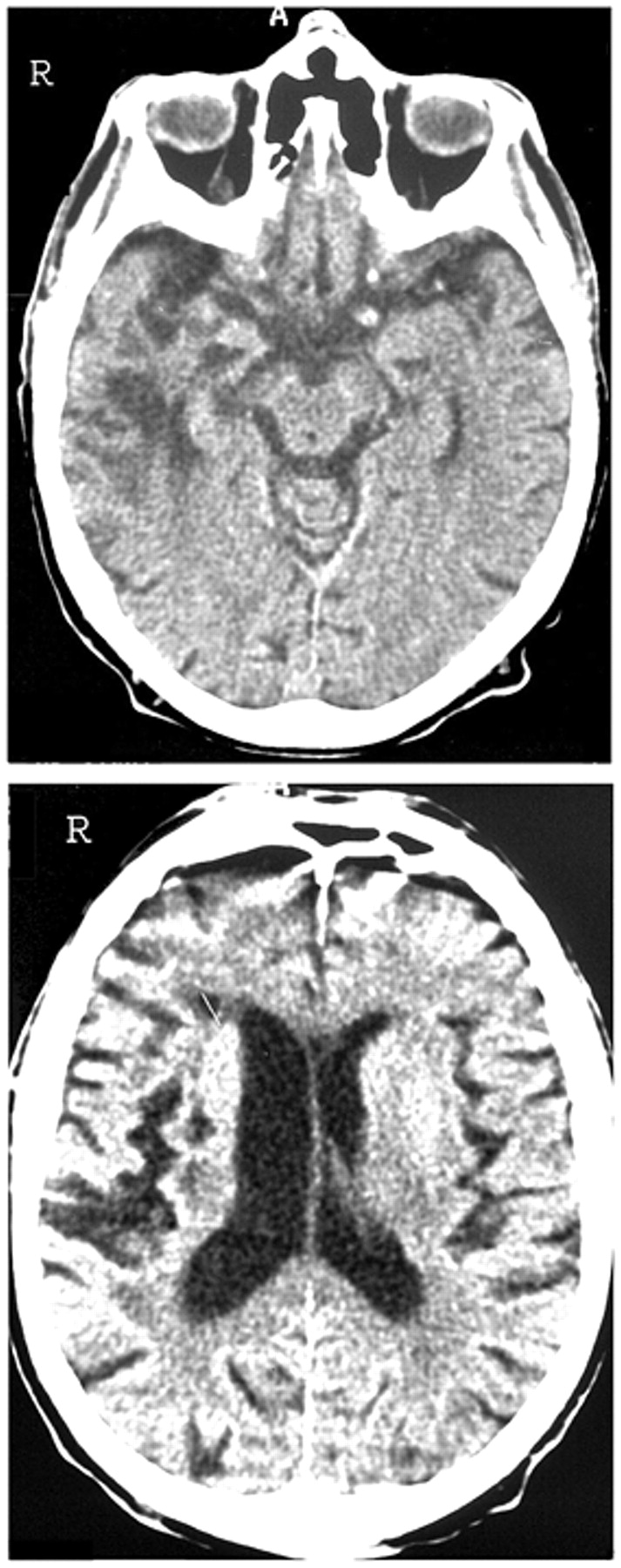
During hospitalization for a transient left-sided hemiplegia after a right middle cerebral artery infarct, a 77-year-old man became convinced that members of the medical staff wanted to steal his house. Although he was rapidly discharged (5 days later), he subsequently declared that his wife had had a love affair with a school master many years before. The patient had always been jealous and envious of the teacher, and he believed that his wife was still seeing him. During the 3 years following his infarct, he had to be hospitalized on several occasions because of verbal and physical abuses toward his wife as well as bouts of severe depression, during one of which he made a serious suicide attempt. On examination, 1 month after his infarct, the patient presented as mildly intellectually deteriorated and the recall test of the Rey figure demonstrated defects in visuospatial memory. Although outwardly calm, he showed a marked lack of emotional control when discussing his wife. It transpired that the evidence he gave to support his beliefs regarding her infidelity were false interpretations of trivial past events. A CT head scan (
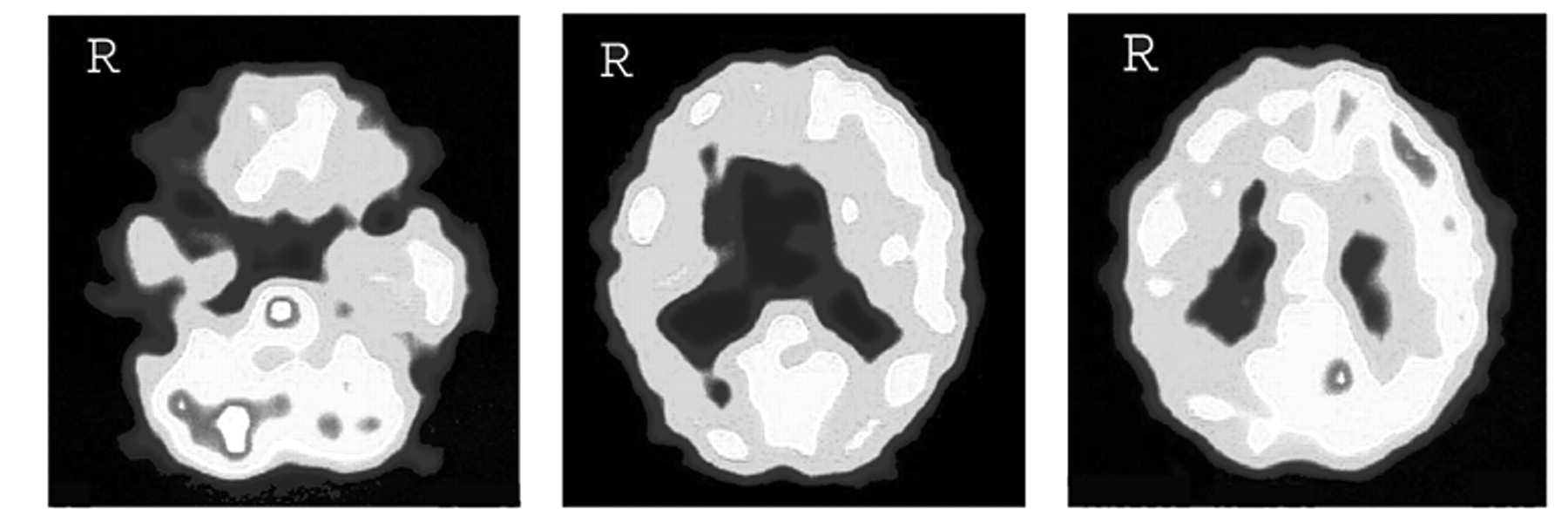
Figure 1 ) showed a low density defect of the right temporal and parietal lobes as well as mild cortical atrophy. Single photon emission computed tomography(SPECT) using hexamethyl-propyleneamine oxime (HMPAO) (
Figure 2 ) revealed a large hypoperfusion of the right hemisphere, involving the right frontal lobe, the possible result of a deafferentation (or diaschisis) effect.
In their study of the anatomical basis of delusions after right cerebral infarction, Levine and Grek
1 argued that delusions depended primarily on premorbid brain atrophy rather than location and size of the lesion. However, this conclusion has been challenged by Westlake and Weeks
2 who described a case, after right infarction, in a much younger patient. Furthermore, Levine and Grek’s conclusions were only based on the results of CT scans, and did not take into account the possible functional effects of the lesions. Malloy and Richardson
3 underlined the role of the lesions of the frontal lobes and the right hemisphere in various content-specific delusions and suggested that, in at least some cases, a dysfunctional frontal system may be a necessary component in the development of fixed delusions. In a case of spatial delirium (reduplicative paramnesia), Nighoghossian et al.
4 demonstrated with SPECT the pathogenic role of functional right hypofrontality. We submit that our case indicates that right frontal involvement is crucial in the emergence of delusional jealousy. This would explain why a similar delusion appeared after a right frontal biopsy in the case described by Silva and Leong
5 when the infarct was in the left frontal lobe. Of course, such neuroimaging correlates do not exclude, particularly in older patients, the etiological role of psychological factors, such as premorbid jealousy and/or paranoid personality traits.