More than 30,000 Americans commit suicide every year, highlighting the need for improved evaluation and prevention of suicidal behavior.
1 Although the base rate for suicide among psychiatric patients is low, about 90% of people who do commit suicide have a psychiatric illness.
2 Previous research indicates that people diagnosed with schizophrenia, affective disorders, and personality disorders are 10 times more likely to commit suicide than those in the general population.
3 Neurocognitive functions, such as planning ability, impulsivity, and other executive skills could contribute to the risk of suicidal thinking and behavior. In an effort to better understand the association between mental illness and suicidal behavior, recent studies have focused on cognitive abilities as potential moderating factors. We will consider the emerging literature on neurocognition and suicide against a backdrop of neurobiological and neuroimaging research establishing a strong connection between cerebral function and suicidal behavior. It has long been known from postmortem studies that suicide completers have decreased levels of serotonin or its main metabolite, 5-hydroxyindoleacetic acid (5-HIAA).
4,5 Lower 5-HIAA in cerebrospinal fluid is also associated with suicidality and suicide attempts among patients with depression
5 and other psychiatric illnesses, including schizophrenia and personality disorders.
4 There are also indications that suicidality is associated with smaller brain volumes in orbitofrontal cortex and anterior corpus callosum
6,7 and with lower perfusion of the medial prefrontal and subgenual areas and ventral tegmentum.
8 Abnormalities such as these have been hypothesized to contribute to impaired impulse-control and decision-making, which directly relate to executive functioning and suicidal behavior.
Executive functions appear particularly susceptible to impairment in psychiatric populations, particularly among individuals with bipolar disorder, borderline personality disorder, depression, and psychotic disorders.
9–13 Executive functions include 1) reasoning and problem-solving; 2) planning, strategizing, and organizing behavior; 3) switching and cognitive flexibility; 4) monitoring and adjusting one's own performance; and 5) inhibiting inappropriate behavior. Prefrontal areas of the brain, which are responsible for the evaluation of changing alternatives and the execution of plans, are often implicated in executive tasks.
14 Most executive functions are linked to the dorsolateral prefrontal cortex, whereas response inhibition is associated with the orbitofrontal region.
15Recent neuropsychological research suggests that suicide attempters do, in fact, show deficits in executive functioning, which could contribute to suicidality. For example, Keilp and colleagues
16 found that depressed, high-lethality suicide attempters performed worse than nonpatients on several neuropsychological measures, and also performed significantly worse than low-lethality attempters on tests of executive functioning. A follow-up study concluded that impaired attention was related to suicidal behavior beyond what could be explained by depression alone.
17 Furthermore, several studies have suggested that decision-making and impulsivity are associated with suicide attempts, to the extent that impulsivity may increase the risk of suicidal behavior but may dampen the planning required to cause death.
18–21Other studies, however, have shown contradictory findings. Westheide and colleagues,
22 for instance, found that executive dysfunction was evident only in recent attempters who still had suicidal ideation at the time of assessment. A study comparing depressed patients with and without suicidal ideation showed that those with ideation performed significantly worse on some measures of reasoning and flexibility, but not on a test of inhibition.
14 Other analyses have yielded no significant relationships between neuropsychological performance and measures of suicidality in patients with depression and psychotic disorders, leading some to hypothesize that suicidality is a separate domain that is distinct from psychiatric symptomatology and neurocognitive performance.
23,24Furthermore, a small number of studies have demonstrated that individuals with a history of suicidality perform
better on some measures of cognition than do those without suicidality. For example, Nangle and colleagues
25 reported that participants with at least one lifetime suicide attempt performed better than did nonattempters on measures of attention and verbal fluency, suggesting that better executive-related ability is associated with greater ability to formulate plans and initiate goal-directed behavior (i.e., the suicide attempt). Similarly, another study demonstrated that those with a lifetime history of suicidality outperformed participants with no history of suicidality on multiple neuropsychological measures, including tests of executive function.
26 After controlling for hopelessness, however, neuropsychological measures did not predict either current or lifetime suicidality, suggesting that hopelessness, rather than cognition, should be targeted for intervention. Given such conflicting results over a wide range of clinical diagnoses and methodologies, further research is warranted to clarify the nature of neurocognitive impairments in suicidal psychiatric patients.
The present study was designed to examine the role of executive functioning in individuals with psychiatric illness receiving acute care for either a recent suicide attempt or severe suicidal ideation. We included suicide Attempters and suicide nonattempters (Ideators) to enable comparisons between those who think about suicide
and make an attempt versus those who think about suicide but
do not make an attempt and instead access psychiatric care. Because of the diffuse neuropsychological impairment common in severe mental illness,
9,11,12,27,28 we hypothesized that 1) participants would demonstrate impairment in executive function at a group level; and 2) suicide Attempters would show greater impairment than suicide Ideators.
METHOD
Participants
Participants included 77 individuals (37 Attempters and 40 Ideators) with psychiatric illness recruited from 1) the Maricopa Integrated Health System Psychiatric Inpatient Unit in Phoenix, AZ, (N=35); 2) the University of California, San Diego, CA, Inpatient Psychiatric Unit (N=2), or 3) San Diego, CA, Community Research Foundation Short Term Acute Residential Treatment Centers (N=40). All participants met the following inclusion criteria; they were 1) between the ages of 18 and 60; 2) currently receiving treatment for either a suicide attempt or suicidal ideation; 3) diagnosed with major depressive disorder, bipolar affective disorder, borderline personality disorder, or a primary psychotic disorder (schizophrenia or schizoaffective disorder); and 4) their primary language was English. Potential participants were excluded if they had a history of epilepsy, dementia, mental retardation, or traumatic brain injury with loss of consciousness greater than 30 minutes. The study was IRB-approved, and we obtained informed consent after participants received a complete description of the study.
Procedure
After hospitalization or crisis-house admission, each patient's diagnosis was determined by the treating psychiatrist and treatment team, and suicidal ideation and behavior were confirmed via chart review. Patients who met the inclusion criteria were invited to participate by a treating clinician and provided written informed consent to a research assistant. Participants first gave a brief history of their life circumstances and history of suicidality, then completed a 1-hr. neuropsychological battery. After assessment, each test was scored according to published norms.
Measures
American National Adult Reading Test (ANART; estimated premorbid IQ):
premorbid intellectual functioning.29The Delay=Go Computer Task (G.C. Pluck, personal communication, June 9, 2002; total early starts): sustained attention and inhibitory control.
Trail-Making Test, Parts A and B (completion time
T score):
processing speed and cognitive flexibility.30The Controlled Oral Word-Association Test (COWAT; FAS total
T score; Animals total
T score):
verbal problem-solving and verbal processing speed.31The Stroop Test (interference condition, total correct
T score):
response inhibition, impulsivity.32The Wisconsin Card-Sorting Test (WCST-64; Total Errors
T score):
reasoning, problem-solving, self-monitoring, and switching.33Statistical Analysis
All variables were inspected for normality; number of lifetime suicide attempts and number of early starts on the Delay=Go Computer Task were skewed, and these data were analyzed using square-root–transformed variables. For the first hypothesis, mean neuropsychological performance for the entire sample was calculated. All T scores are scaled such that a score of 50 and a standard deviation (SD) of 10 characterize the normal population, where higher scores indicate better performance; T scores greater than 40 are considered average to above-average. T scores were not calculated for the Delay=Go Computer Task because norms for this test are not available, so raw scores were used for this test. For the second hypothesis, group differences on demographic, clinical, and neuropsychological variables were analyzed with t-tests and chi-square tests. Equal variances were not assumed for any t comparison in which Levene's test for equality of variances was significant. The final prediction model of suicide Attempter status was analyzed using logistic regression, in which all participants with complete data were included. We also performed a likelihood-ratio test to examine whether each block of demographic, clinical, and neuropsychological variables contributed significantly to the final model. Alpha for significance was set at 0.05, and all tests were two-tailed. Data were analyzed using PASW Statistics for Windows (Version 18). There were no significant diagnostic group differences on neuropsychological performance (one-way ANOVA; all ps ≥0.061), so the diagnostic groups were combined for all analyses.
RESULTS
Sample Characteristics
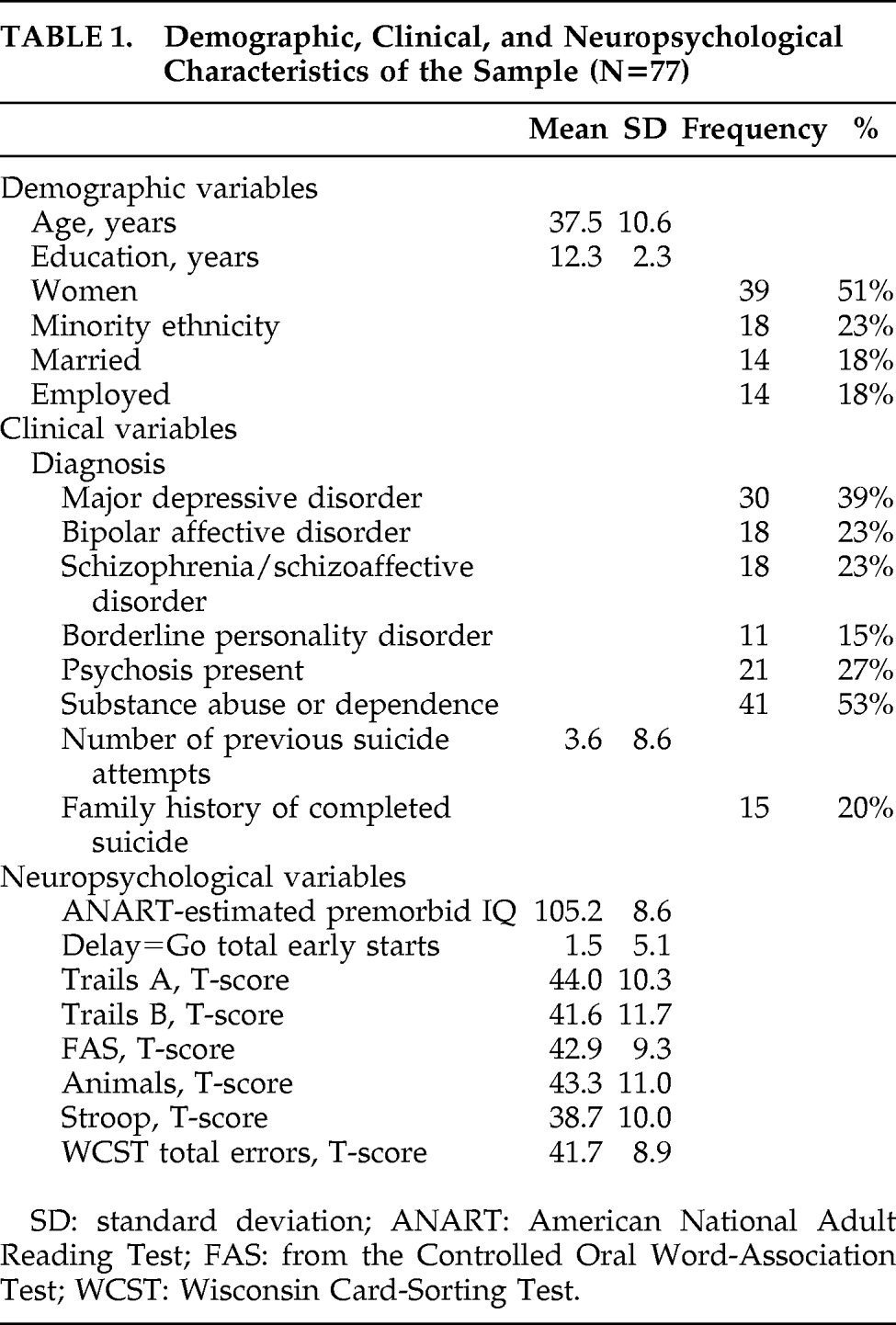
Demographic, clinical, and neuropsychological characteristics of the sample are presented in
Table 1. Participants had a mean age of 37.5 years, and most had completed high school; about half were women, and one-quarter were of minority ethnicity. The majority of participants had a comorbid substance- or alcohol-use disorder, and, on average, participants had four previous suicide attempts.
Hypothesis 1:
The first hypothesis was only partially supported: participants performed in the average range on all neuropsychological measures except the Stroop test, on which they were mildly impaired, as a group (
Table 1).
Hypothesis 2:
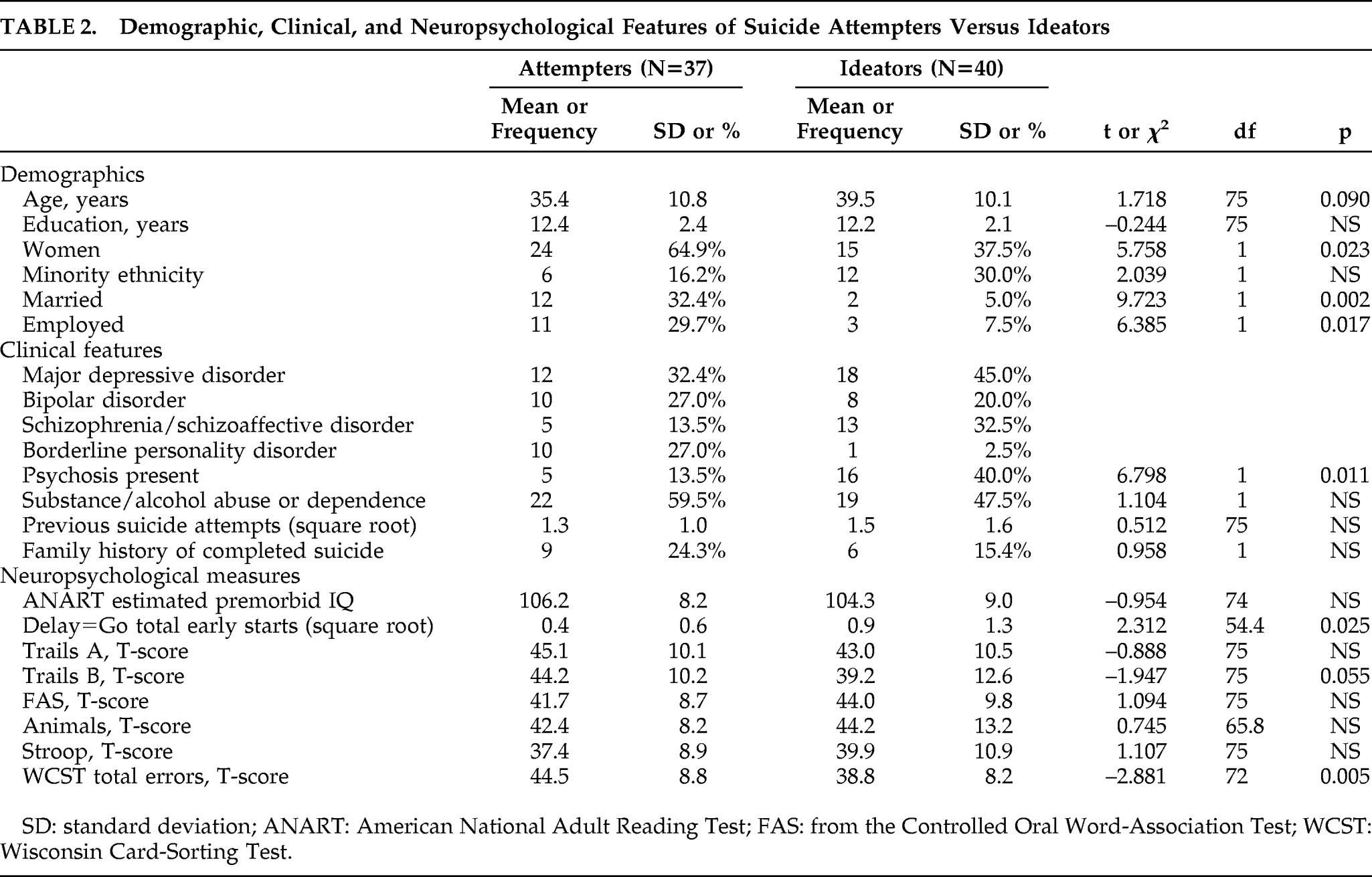
To examine differences between suicide Attempters and suicide Ideators, we first compared groups on demographic and clinical variables. Suicide Attempters were significantly more likely to be women, married, employed, and have a nonpsychotic diagnosis (
Table 2). Groups did not differ on age, education, ethnic minority status, presence of substance-use disorder, or family history of completed suicide (all ps≥0.09; see
Table 2).
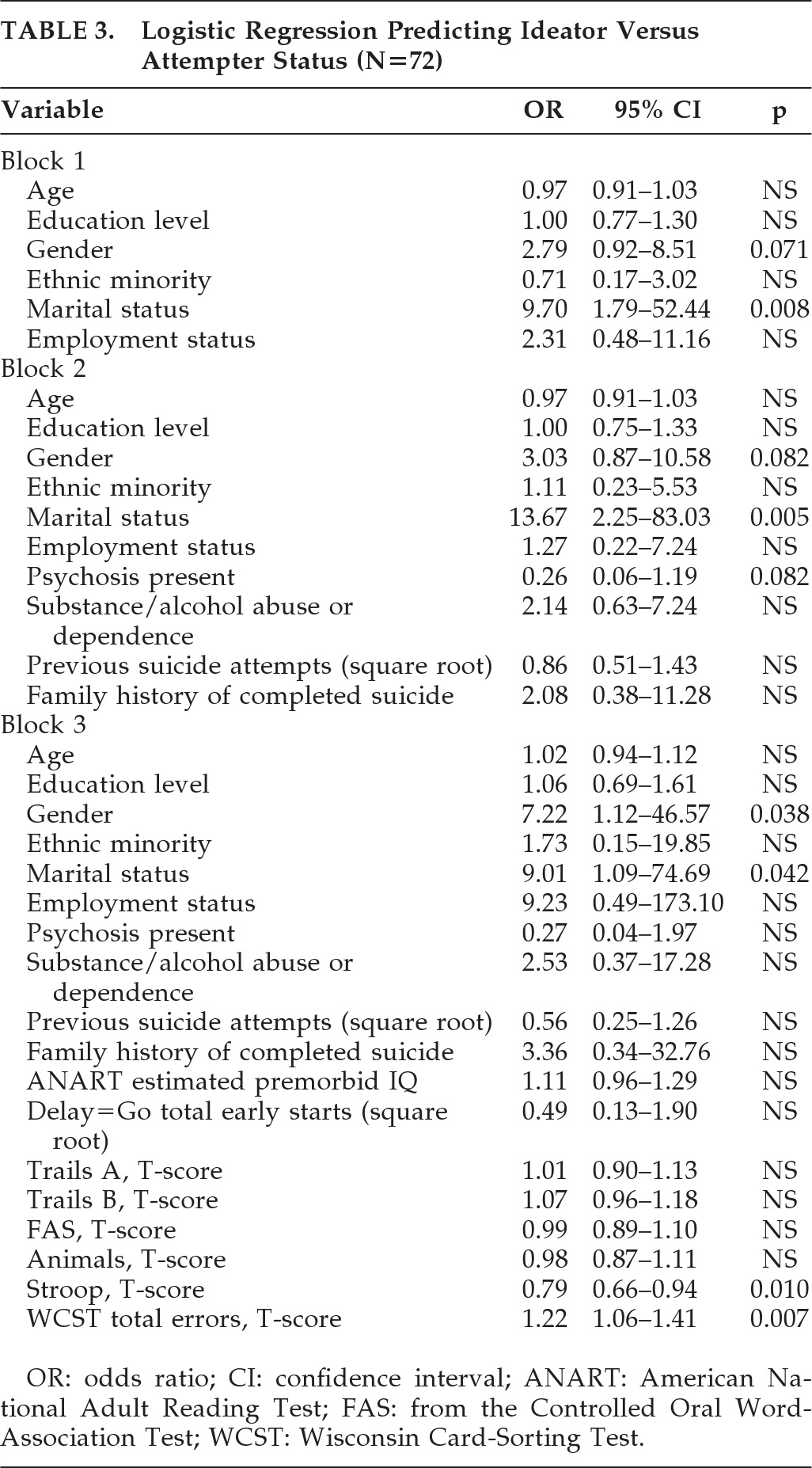
Because the identified group differences would limit inferences about neuropsychological performance between Attempters and Ideators, we performed logistic-regression analyses, with demographic variables entered in Block 1, clinical variables entered in Block 2, and neuropsychological variables entered in Block 3 (
Table 3). Likelihood-ratio tests showed that the block of demographic variables contributed significantly to the full model, as compared with the intercept-alone model (χ
2=18.73, df: 6, p=0.005), but the block of clinical variables did not (χ
2=6.15, df: 4, p=0.188). The third block of neuropsychological variables also contributed significantly to the full model (χ
2=26.47, df: 8, p=0.001).
Consistent with our second hypothesis, worse inhibition performance was associated with suicide Attempter group membership (Stroop Interference total correct
T score; odds ratio (OR): 0.79, p=0.010), however, better problem-solving ability was also associated with the Attempter group (WCST total-errors
T score; OR: 1.22, p=0.007). Also, being married (OR: 9.01, p=0.042) or female (OR: 7.22, p=0.038) increased the odds of membership in the Attempter group. No other variables were significant predictors of group membership (all ps≥0.14; see
Table 3).
DISCUSSION
To our knowledge, this is the first study to compare recent suicide attempters to recent suicide ideators, based on the concept that there may be subtle cognitive differences between those who consider suicide but do not act on their impulses and those who make a suicide attempt. To better pinpoint these hypothesized differences, we aimed to evaluate executive functioning in acute-care psychiatric patients with either a recent suicide attempt or recent suicide ideation. Contrary to our first hypothesis, participants in this study demonstrated various cognitive strengths; they performed in the average range on all measures except a measure of inhibition, on which they were mildly impaired. However, their
T scores on the executive functioning tests were all at the low end of the average range. These data suggest that our participants' distribution of executive-function performances overlaps to some extent with that of the healthy individuals on whom these tests were normed. Consistent with previous research,
20,21 impairment in inhibition may be a specific risk factor for suicidal ideation and behavior.
Support for our second hypothesis was mixed: in a model controlling for demographic, clinical, and other neuropsychological variables, disinhibition was significantly associated with the suicide Attempter group, again suggesting that disinhibition may represent a dominant pathway to a suicide attempt. In fact, Mann and colleagues
2 asserted that prominent impulsivity and aggression are characteristics of people at risk for suicide, independent of psychiatric diagnosis. Contrary to our expectation, better problem-solving ability was also associated with the suicide Attempter group. This finding may lend support to Nangle and colleagues′
25 assertion that better executive functioning (e.g., better problem-solving) is associated with better planning and initiation of behavior, which may lead to increased risk of attempting suicide.
Although we did not hypothesize any demographic differences between attempters and ideators, our results indicated that women and those who were married were more likely to have attempted suicide. This gender difference is not unexpected; women attempt suicide three times more often than do men.
34 Marriage, however, is often reported as a protective factor against suicide.
35,36 Given these conflicting findings, further investigation is merited to clarify the role of marital status in suicide risk.
Limitations of the study include small sample size, which may have limited power to detect significant differences between the suicide Attempter and suicide Ideator groups. Replication of these findings with a larger sample is needed. Also, no structured diagnostic interview was used to supplement chart diagnoses, and acute-care settings such as inpatient psychiatric units and crisis-houses necessarily gather cross-sectional information rather than longitudinal data to inform clinical diagnosis and treatment. Therefore, it is possible that some participants were misdiagnosed and were consequently included in the wrong diagnostic group, which could have affected our finding that the groups were neuropsychologically comparable. Also, suicidal ideation and depressive symptoms like hopelessness at the time of the assessment were not evaluated, which precluded analyses controlling for these variables. As previous research has demonstrated, these clinical features may be important to consider.
22,26 Finally, because this was a cross-sectional study, we could not examine long-term outcomes (e.g., completed suicide). Longitudinal data would be helpful to examine neuropsychological profiles not only of suicide ideators and attempters, but completers as well.
Despite these limitations, our results suggest that neuropsychological functioning may differentially influence the suicidal behavior of psychiatric patients. Specifically, lowered inhibition but better problem-solving appears to be associated with making a suicide attempt, rather than just thinking about suicide. It therefore seems pertinent to develop interventions to target impulsivity and inhibition in an effort to reduce suicidal behavior in people with mental illness. Another important consideration is whether and how the preservation of certain cognitive skills may increase the chances that an individual will attempt suicide. If it is the case that those with better planning ability are more likely to carry out a plan for suicide, then interventions may be able to target individuals who demonstrate good problem-solving ability but are impulsive. Given our results, it may be that disinhibition and intact problem-solving represent a specific neuropsychological profile for those at risk for suicide. Additional investigation is needed to support these conclusions and emphasize the need for targeted interventions to decrease the number of deaths by suicide in psychiatric populations.
Acknowledgments
This work was presented at the 38th Annual Meeting of the International Neuropsychological Society, Acapulco, Mexico, February 3–6, 2010.