To the Editor: Recent studies have suggested that hippocampal neurogenesis may be stimulated by successful treatment of posttraumatic stress disorder (PTSD), either by drugs
1–4 or by behavioral interventions.
5 Three investigations have evaluated the effects of pharmacotherapies and have suggested that antidepressant treatments may increase hippocampal volume.
1–3 Lindauer and colleagues
6 examined the effects of a psychotherapy intervention, the Brief Eclectic Psychotherapy, on hippocampal volumes and observed no changes on hippocampal volumes upon amelioration of PTSD symptoms. However, the authors recently reported
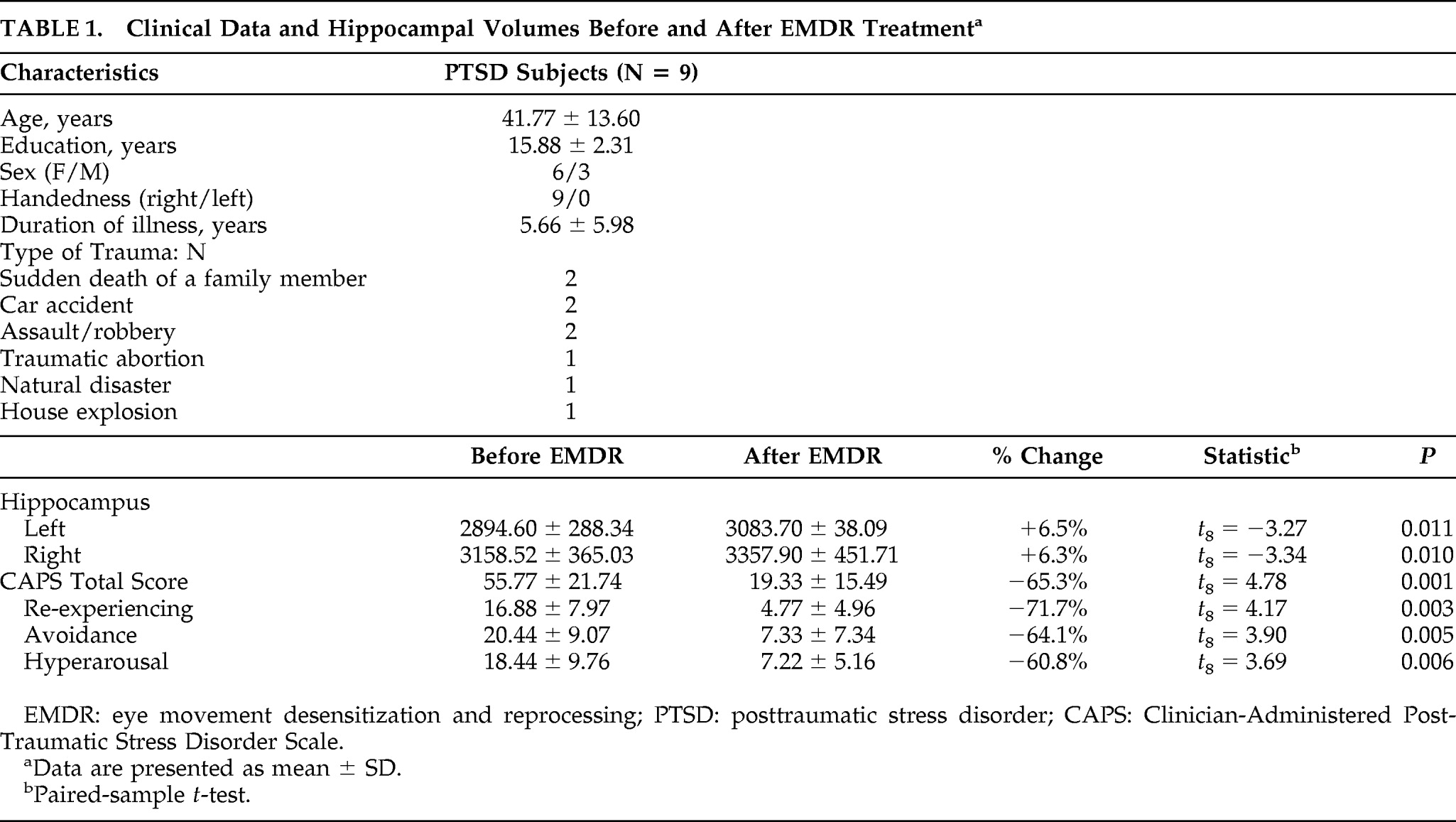
5 the case of a patient treated with Eye Movement Desensitization and Reprocessing (EMDR) who showed an increase in both left- and right-hippocampus upon improvement in PTSD symptoms. The aim of this study was to further investigate the relationship between EMDR treatment and hippocampal volumes in PTSD subjects. The study was conducted at the Department of Psychiatry, University of Siena Medical Center. Inclusion criteria were current PTSD and age 18–65 years. Exclusion criteria were current and/or lifetime comorbid psychiatric diagnoses as ascertained via the SCID; previous or current use of any psychotropic medication; history of head trauma; and presence of neurological, endocrine, or degenerative disorders. The authors recruited 10 outpatients, but one patient was excluded from the study because of MRI signal abnormalities. The remaining nine subjects were three men and six women, mean age: 41.77 (SD: 13.60) years. Subjects were assessed before and after EMDR treatment through the Clinician Administered Posttraumatic Stress Disorder Scale (CAPS) Italian Version,
7 which is known to be a reliable measure of PTSD symptom severity. All volumetric MRI scans were performed with a 1.5 Tesla Philips Intera Machine (Philips Medical Systems; Best, the Netherlands). The imaging protocol included a T1-weighted Fast Field Echo (FFE) 1-mm-thick coronal images (matrix 512 x 512, slice thickness: 1 mm, slice number: 75). Hippocampal volumes were calculated by manually tracing the structure separately for the left and right hemispheres on each coronal slice and then summing these areas of successive coronal slices with the ANALYZE Software Package, Version 5.0 (Biomedical Imaging Resource, Mayo Clinic Foundation, Rochester, MN). The boundaries of the hippocampus were drawn following the guidelines described by Watson Laboratories, Inc.,
8 as described in a previous study.
9 The measurements were performed by a single rater blind to subjects' identity and treatment status. The treatment followed the guidelines by Shapiro.
8 the therapy was given in a 90-minute session and was randomly assigned to three trained psychotherapists. Duration of the treatment was 3 months (12 ± 1 EMDR sessions). The bilateral sensory stimulation included both eye movements while following the finger of the therapist and tapping the hand of the patient. All sessions were videotaped; the fidelity to the treatment protocol was assessed by an independent evaluator, a psychologist and licensed psychotherapist who is an EMDR European-approved consultant and supervisor and who was not involved in the present study. Three months after the start of EMDR treatment, all subjects were reevaluated with MRI and CAPS.
Statistical analyses were performed with SPSS Version 13.0 for Windows (SPSS Inc, Chicago, IL). Hippocampal volumes were analyzed with a repeated-measures analysis of variance. Also, two-tailed, paired-sample
t-tests were used to compare hippocampi, clinical assessments on CAPS total score, and each subscale of the CAPS before and after treatment. An alpha level of 0.05 was used for all statistical tests. The analysis showed that there was a significant difference in hippocampal volumes after the treatment (F=11.70; df=1,8; p=0.009) and a significant difference between the two sides (F=18.95; df=1,8; p=0.002), but no interaction between treatment phase and side (F=0.11; df=1,8; p=0.742). Detailed analyses indicated that there was an increase in both the left (+6.5%;
t = –3.27; df=8; p=0.011) and the right side (+6.3%;
t = –3.34; df=8, p=0.010;
Table 1). After treatment, we also observed an improvement in PTSD symptoms as measured with CAPS total score (−65.3%;
t=4.78; df=8; p=0.001), and on the three CAPS subscales (
Table 1). After the treatment, all subjects no longer met the SCID criteria for PTSD. Despite these promising results, we acknowledge that the present study is only a pilot study because it has several limitations. First, the sample size was small. Second, there was no control group (this choice was motivated by ethical reasons). Third, we do not know whether the increase in hippocampal volume was caused by a promotion of neurogenesis or other reasons, such as, for example, a change in water content in the hippocampus. Despite these limitations, the results of this preliminary study suggest further consideration of the potential effects of psychotherapy on the neurobiology of psychiatric disorders, and not dismissing the question of whether psychotherapy may have beneficial effects on hippocampal structure. Further studies should be carried out in order to validate the present results, possibly with a larger sample of PTSD subjects, a control group, and different types of psychotherapy.