To the Editor: Prosody refers to the patterns of stress and intonation in language. A few studies suggest that Alzheimer's disease (AD) patients have deficits in production, repetition, and comprehension of emotional prosody. The authors present the case of an AD patient with prosodic speech alteration; to test such impairment, we administered an extensive test battery investigating emotional comprehension and production. The patient was tested for visual channel information by an Ekman and Friesen series. The authors found that prosody impairment can early occur in the disease course, and, for many primary emotions, impairment in the auditory channel seems to mirror the visual channel. Prosody is a term used to cover features of speech such as the emphasis placed on certain syllables, changes in tempo or timing, and differences in pitch and intonation. Ross and Mesulam
1 demonstrated that prosody can be impaired independently of other language functions. Most studies that have examined emotional prosody (the nonverbal affective components of language) have used normal control subjects and patients with unilateral brain damage. These studies suggest that the integrity of the right hemisphere is important for both expression and comprehension of emotional prosody. Ross
2 proposed that the right hemisphere is organized for affective language expression and comprehension in a manner that is comparable to the organization of propositional language in the left hemisphere. This difference (supralexical semantic information, such as interrogative or assertive mode, versus emotional connotation, such as happiness, anger, sadness, etc.) has been investigated by a few fMRI studies that have reported activation in the right hemisphere, especially in the right inferior frontal area,
3 during emotional detection versus verbal detection. This finding is remarkably congruent with neuropsychological studies of aprosodias. In AD, damage to the right hemisphere structures occurs as part of the widespread progressive degeneration, suggesting that emotional prosody and other areas of affective communication may be compromised. A study of linguistic functioning in AD patients
4 reported that transcortical sensory and sensory aphasias were prominent in the early stages of AD, with global aphasia appearing at the end stage. The progression of prosodic alteration seems to mirror the model proposed by Appell. In fact, Roberts et al.
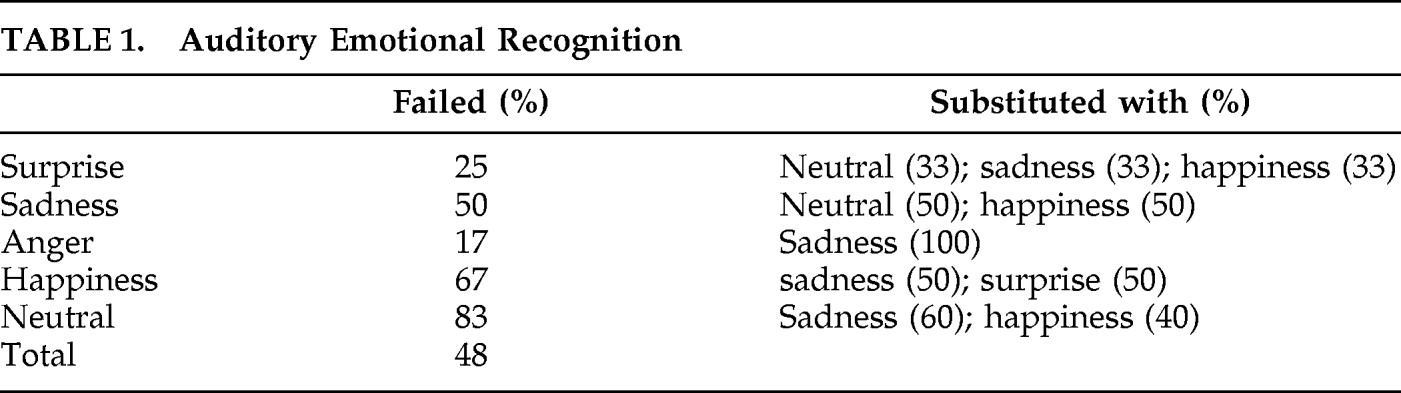
2 suggested that AD patients have deficits in production, repetition, and comprehension of emotional prosody (
Table 1). Deficits in comprehension of emotional prosody seem to appear relatively early in the course of AD and are relatively resistant to further decline throughout the mild and moderate stages of the disease. Repetition and production of emotional prosody are relatively preserved early in the course of the illness, whereas a significant impairment emerges in the moderate stage of the disease.
We present the case of an AD patient who, in spite of the relative early stage of his disease, suffered from an evident impairment of prosodic comprehension and production: caregivers indicated the patient's speech alteration, described as “flattened,” “without emotions,” as one of the first hints of the disease. In order to test such prosodic impairment the patient underwent an extensive battery investigating comprehension (auditory emotional decoding), production (auditory emotional coding), as well as emotional decoding through the visual channel (images taken by Ekman and Friesen series, 1976).
Case Report
The patient, a 55-year-old man, was diagnosed with early-onset AD. The first symptoms (reported by the patient and caregivers) were memory impairment and anomia, followed by apathy, depression, and irritability, as well as the reported speech alteration. Neurological exam was normal as well as Mini-Mental State Exam score (29/30). MRI showed cortical/subcortical atrophy in fronto-parietal areas; the 18-FDG PET scan evidenced hypometabolism in the right frontal-temporal-parietal areas as well as left posterior parietal areas and basal ganglia. The patient underwent to an extensive neuropsychological test battery assessing episodic memory (both verbal and visuospatial), constructional abilities, attention-shifting abilities, abstract thinking, verbal fluency, and naming. A widespread, mild cognitive impairment, more pronounced on tasks sensitive for both right-hemisphere and executive functions congruent with PET result was reported. Also, in order to evaluate the patient's speech, Melodic Alteration—an experimental protocol—was designed:
Emotional Decoding
Auditory verbal task (Task 1): Twelve recorded sentences with emotionally neutral content (e.g., I bake a cake in the oven.) to be presented to the subject, conveyed by a professional actor, with surprise, sadness, anger, and happy emotions, plus the neutral intonation as a control, in a randomized order (total stimuli: 60). The results were compared with those of a control group of 10 healthy subjects, matched for age, education, and sex (mean age: 54.5; mean education: 14 years). Visual task (Task 2): Thirty facial expressions to be presented in six blocks, each of them showing the same five emotions of Task 1 in a randomized order. The patient was asked to indicate each emotion on a separate sheet, to avoid any naming difficulty.
Emotional Coding
Repetition task (Task 3): This was a reproduction of the emotional prosody of the first six-sentence-block of Task 1, to be presented in a randomized order; performance was recorded and then reviewed by two independent raters, who evaluated the similarity between the patient's and the actor's intonation. Production task (Task 4): This was an evaluation of the patient's ability to spontaneously produce emotional prosody, by presenting the second six-sentence block of Task 1, given in a written form. The patient was asked to convey the sentences with surprise, sadness, anger, happy, and neutral intonation. This performance was also recorded and submitted to the same raters who assigned an emotion to each sentence.
Task 1: The patient only recognized 31 out of 60 sentences (versus 58 [SD: 2] of the control group). A prevalent recognition impairment was evident for happiness (67% failed recognition), sadness (50%), and neutral intonation (87.5%). Remarkably, these three emotions were constantly confused with each other (
Table 1). T
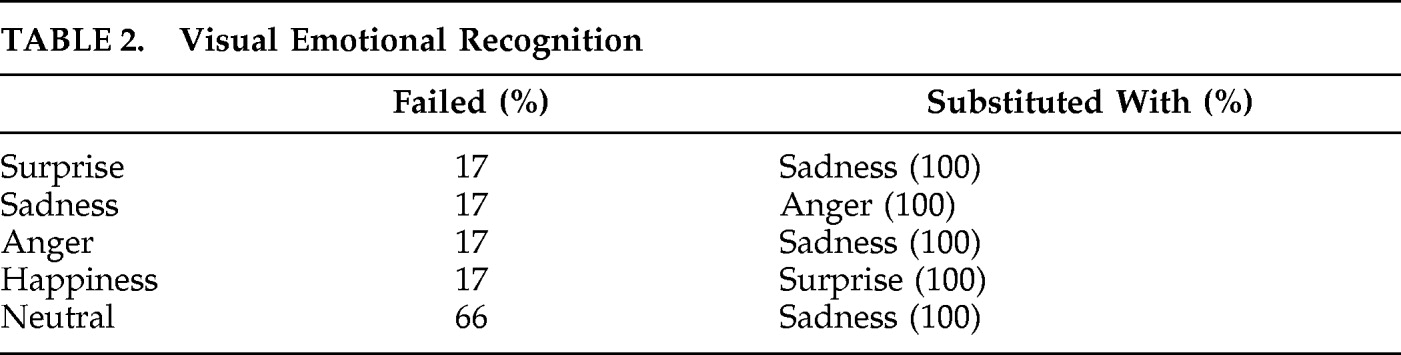
ask 2: The patient recognized 73% of facial expressions (versus 92% of control group) with a prevalent impairment of “neutral,” which was detected as “sadness” in 67% of cases (
Table 2). T
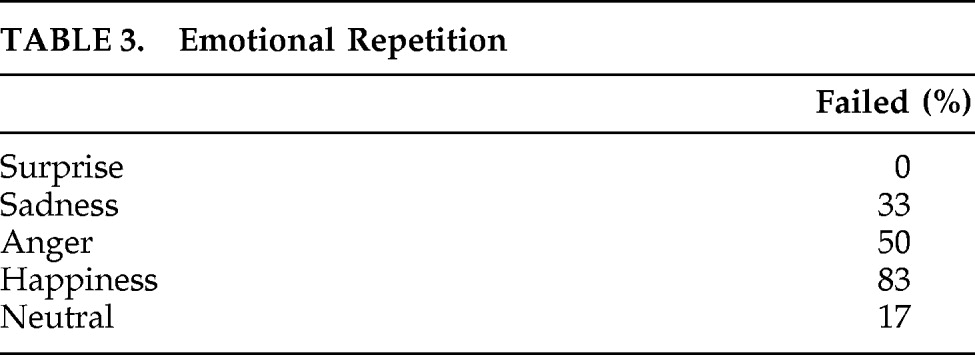
ask 3: Two independent raters reported sentence repetition as “wrong” in 33% of cases, with a high level of concordance (K index=0.86; IC 95%: 1.9–25.2). Because of this concordance, only the first rater's results are shown (
Table 3). T
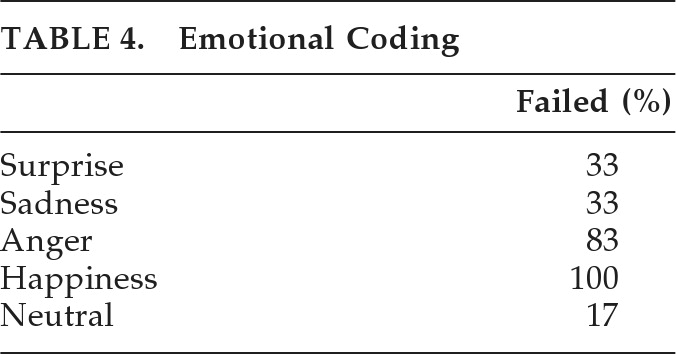
ask 4: Spontaneous production of emotional intonation also showed a consistent deficit, with a major impairment on Anger (83% failed) and a complete impairment in Happiness (
Table 4; K index=0.93; IC 95%: 0.01–0.59).
Discussion
We present a patient showing prominent prosodic deficits occurring in the early stage of AD, with regard to both visual and auditory emotional coding and decoding. In Task 1, prevalent recognition impairment was evident for Happiness (confused with Sadness and Surprise), Sadness (constantly confused with Neutral intonation and Happiness), and, finally, Neutral intonation (confused with Sadness and Happiness). In Task 2, Neutral expression was constantly confused with Sadness. These results could be explained by the association of “neutral” intonation (as well as “neutral” facial expression) with a reduction of melodic intonation (as well as reduction of facial expression), both typical of sadness also. On the other hand, misdiagnosing of surprise and happiness is evident in the auditory tasks, probably for the positive valence of both intonations, whereas, in the visual task, the act of “smiling” well distinguishes happiness from surprise. Task 3 showed deficits in repetition in all tasks except for Surprise, probably because of the strong pitch and intonation of such emotion, easier to repeat for the patient. Finally, Task 4 also showed a complete impairment on Happiness (100%) and a clear deficit to conveying Anger intonation: these deficits appear to be related to the difficulties in production of emotions that require strong intonation and tempo changes. In fact, in this task, only Neutral coding is correctly performed, obviously the only one that conveys absence of emotional sharing. A few studies, to our knowledge, have investigated the ability of emotional decoding through both auditory and visual modalities in AD; most of them lack the support of functional neuroimaging. Data in the literature are dissonant about facial expression recognition in AD
6,7; the present case, instead, demonstrates that such impairment can occur early in the disease course, along with deficits in recognition of prosody; and shows that impairments in the auditory channel for many primary emotions seems to mirror impairments in the visual channel. Such conditions should be seriously considered by therapists and caregivers in order to improve communication and relationships with AD patients.