The New Mexico Medical Disaster Assistance Team aboard an Air Force C-17 cargo plane for the trip to Houston. Psychiatrist Albert Vogel, M.D., is in right foreground wearing an earplug.Psychiatrists don’t normally find themselves delivering babies or running makeshift emergency hospitals. But APA’s Area 7 trustee, Albert Vogel, M.D., seems to be expanding his repertoire of medical experience beyond the typical and into the unpredictable.
As head of the New Mexico Disaster Medical Assistance Team, Vogel is the only psychiatrist to command one of the approximately 28 level-one disaster-relief teams sponsored by the National Disaster Medical System (NDMS). The NDMS draws together the resources and expertise of several federal agencies—the U.S. Public Health Service, Department of Defense, Veterans Administration, and Federal Emergency Management Agency—to bring medical care to disaster victims around the country.
For example, there was a pregnant woman for whom the team performed a Caesarian section in the aftermath of Hurricane Hugo on the Island of St. Croix. More recently, in the wake of the flood that shut down the city of Houston, Vogel was responsible for establishing and administering a temporary emergency department for disaster victims.
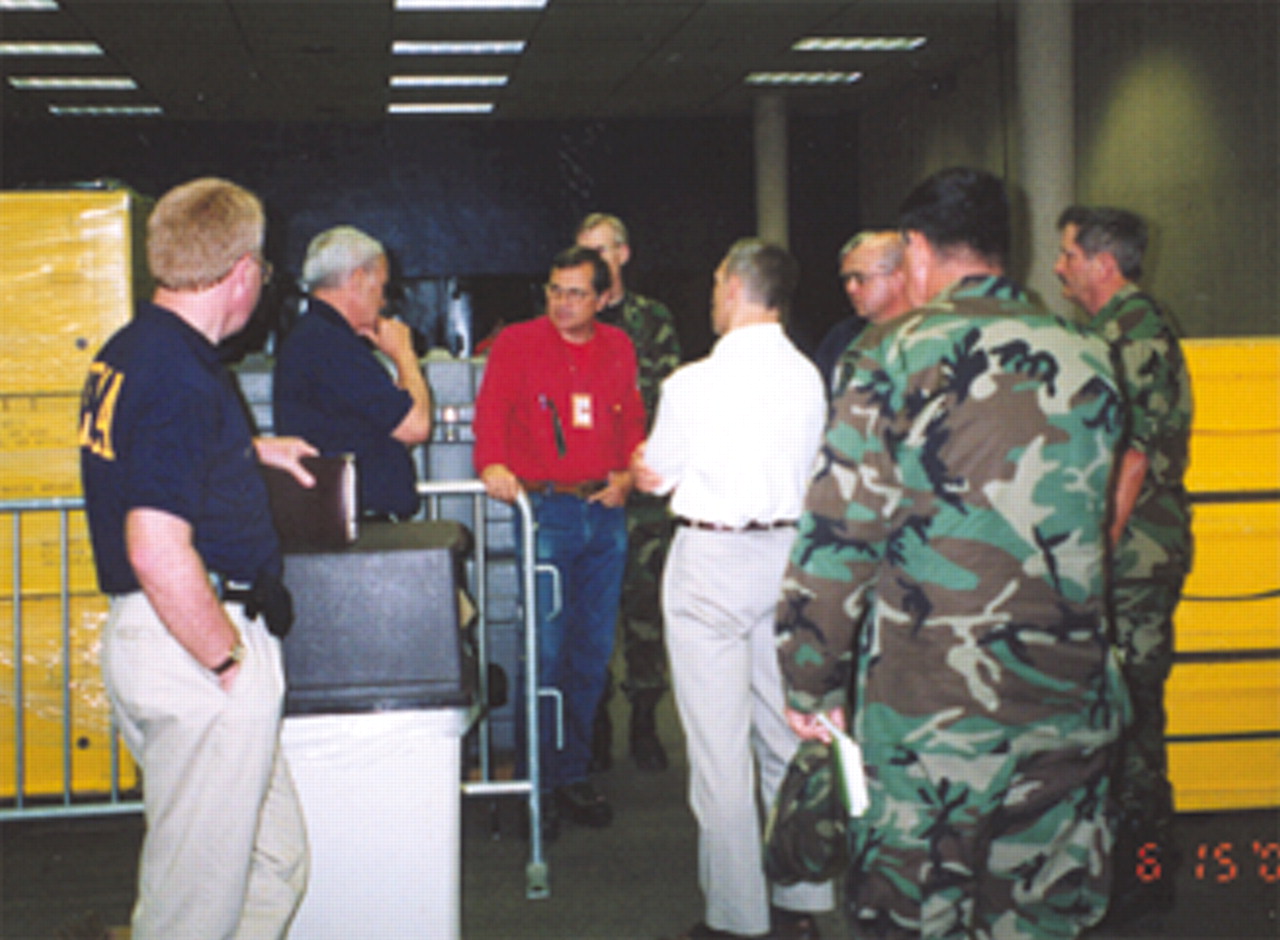
Al Vogel, M.D., (in red shirt) briefs some of the most senior of the VIPs to visit the New Mexico Medical Disaster Assistance Team in Houston. Pictured with Vogel are Lacy Suiter (with hand on chin), executive associate director of the Federal Emergency Management Agency, with his staff, and representatives of the U.S. Air Force 591st Expeditionary Medical Squadron from W. Hall Medical Center, Lackland Air Force Base, San Antonio.In 1984 Vogel’s team was the first to be formed west of the Mississippi. More teams are forming, and there are efforts to regionalize services and to rotate a call schedule. But in practice, Vogel said, the teams go whenever and wherever they are needed.
“We have gone as far as the Virgin Islands for Hurricane Hugo and Hawaii for Hurricane Iniki,” Vogel noted.
And his team appears to have done it all when it comes to disasters: earthquakes, fires, and floods. Most recently, Vogel and his team were sent on very short notice to help provide relief to Houston flood victims in early June.
“We got the call on Saturday about 8:30 in the morning and were put on alert status,” he recalled. “By 11 a.m. we were activated, and we were in Houston in 24 hours.”
Twenty-five team members and 28,000 pounds of gear made the trip on an Air Force C-17. The mission was to set up a makeshift emergency department in the exhibition hall of the Houston Astrodome to serve the overflow of patients from the city’s overextended—and sometimes flooded—emergency rooms.
“Our goal was to help decompress the city’s ERs, which were overwhelmed,” Vogel said. “Many of the basements of hospitals were flooded, shorting out electricity and computers.”
Working closely with the city’s emergency medical service, the team’s goal was to treat not major medical emergencies, but the lesser emergencies that couldn’t be handled at the city’s hospitals. “We started seeing patients on Monday at 8 a.m. and stayed until the next Sunday at 3 p.m.,” he said. “We saw almost 600 patients. Most had minor to moderate medical emergencies. We saw some psychiatric emergencies, but not many—acute stress disorders and some folks with chronic, severe mental illness who couldn’t get their medications.”
The Houston experience is typical in at least one way, Vogel explained. “What has been surprising to the whole NDMS system is that the vast majority of our deployments have not been to treat the direct disaster injuries, most of which are taken care of by the time we get there. What we are doing, instead,” he noted, “is providing typical medical care to people whose regular medical systems have been destroyed. Until the big one comes along, what we do is provide care to people very much like in an urgent care center.”
A typical scenario, for instance, is treatment of children with asthma, whose condition is exacerbated by the stress of the disaster, but who cannot access medical care through their usual sources. Also common are injuries and emergencies resulting from “residual damage,” such as auto accidents, he said.
From a psychiatric perspective, earthquakes can be the most tumultuous event, with their recurrent aftershocks that rob victims of a sense of immediate closure. During the 1994 earthquake in Northridge, Calif., for example, the number of casualties—both physical and emotional—continued to mount even after the main quake was over.
In contrast, Vogel says, a hurricane does its damage and is over.
“After an earthquake the ground is still shaking,” Vogel pointed out. “The aftershocks can be very strong and can cause damage, literally knocking some buildings down. From a psychiatric point of view, the continual changing of the ground increases and prolongs the stress.”
Austere Environment
So what does it take to practice disaster medicine?
Vogel says practicing disaster medicine means a tolerance for the kind of rapid, high-stress, medical improvisation typical of an episode of the television show, “ER.”
“What it takes is the ability to function in an austere environment when you are in a tent and the ground is shaking and there is no power, trying to provide the best medical care you can provide,” Vogel explained.
Some team members receive training in “critical-incident stress management,” designed to help those members of a community—especially police and emergency medical personnel—who are likely to be the first responders to the most horrific sequelae of a disaster. As Vogel said, “It’s designed to help people who have to pick up body parts.”
Not that every disaster situation is so dramatic. “What we do depends on the situation when we get there,” he said. “We have gone to a site and done nothing. Occasionally, we get prepositioned for a hurricane and turn around and come home because the hurricane didn’t cause enough damage or injury for our team to be needed.”
But even in those infrequent situations, the NDMS teams are supplying a critical preventive function. And yes, team members have regular day jobs—so hopping on a plane at a moment’s notice is not all fun and games.
Job Arrangements
“All of our people have to get permission from their employers to take leave,” he notes. “That creates an interesting problem, especially with nurses. The shortage of nurses makes it harder on employers to allow staff to take 10 days or so. We would like to get as much publicity as possible about what we do when we are deployed, so that employers know that when their personnel are off for 10 days, they are providing a valuable clinical service and not going out and playing in the sand.”
Team members are paid during deployment as temporary employees of the U.S. Public Health Service, but are not paid for the four training sessions that take place each year. In any case, however, money is clearly not why doctors and other health care professionals work in disaster relief.
So why do they do it?
“The answer is simple,” Vogel said. “It provides a lot of satisfaction. You have the experience of getting help to people who really don’t have any other source of help.”
And Vogel believes his work as commander of a disaster medical assistance team is a model for younger psychiatrists seeking ways to diversify their careers.
“There are other niches for psychiatrists, other than just practicing psychiatry, per se,” he pointed out. “Psychiatrists have a lot to offer in the provision of disaster medical care, both from the point of view of treating psychiatric conditions—including those that present during disaster settings unrelated to the disaster—as well as psychiatric complications of a disaster. But they also have a role in managing and organizing care in disaster settings. There is the challenge and reward of getting 35 people out the door in 24 hours and allowing them to provide the care that is needed to people who need it.” ▪
When major disasters devastate communities anywhere in the U.S., a New Mexico psychiatrist is ready to board a plane and begin helping victims patch their physical and psychic wounds.
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.