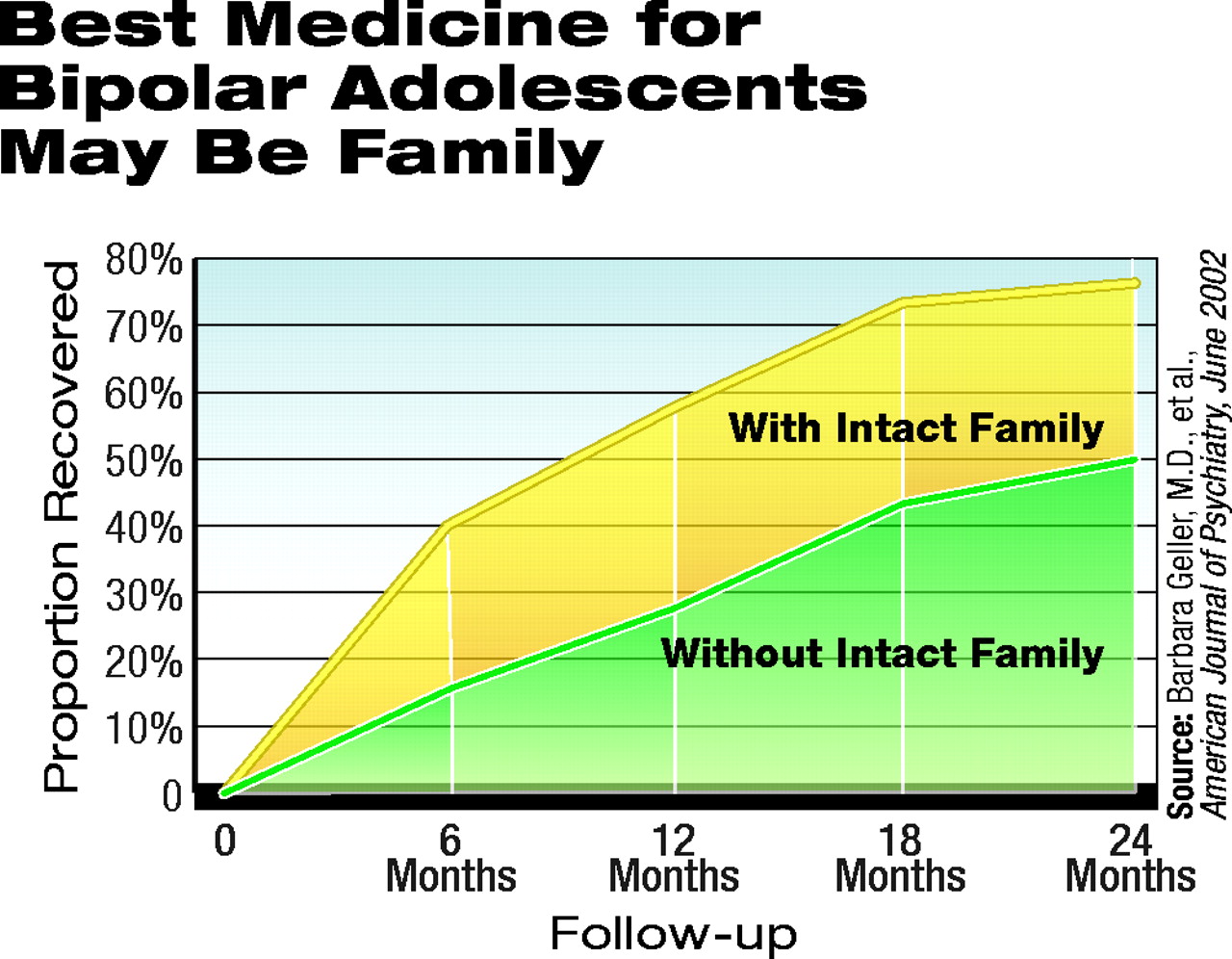
Of the 89 children in the two-year study, 58 had recovered at some point during the two-year period. Of these 58, 39 lived with both biological parents, and 19 lived in other situations.Children with bipolar illness can sometimes be difficult to live with—irritable, aggressive, bossy, or depressed—and they sometimes suffer from extreme psychological anguish.
And now more disheartening news about youngsters with this illness comes from a study conducted by Barbara Geller, M.D., a professor of psychiatry at Washington University School of Medicine, and colleagues. Even if the youngsters are treated, they may not necessarily get better. Details about the study and its results were published in the June American Journal of Psychiatry.
In a two-year study of children with moderate to severe bipolar disorder, Geller and her research team studied 89 children whose average age was 11. All met DSM-IV criteria for mania—that is, with elation and/or grandiosity. They had to experience mania for at least two weeks or hypomania for at least two months to be included in the study. All of the children were also moderately to severely impaired by their condition, as indicated by the Children’s Global Assessment Scale. For instance, 60 percent had psychosis as defined by delusions or hallucinations, and 25 percent were suicidal.
Geller and her colleagues interviewed the 89 children and their mothers at the start of the study, and again at six, 12, 18, and 24 months into the study, to obtain information about the youngsters’ mental health, the types of treatments they were receiving for bipolar disorder, and their living environments. Mothers were used instead of fathers for the interviews, Geller told Psychiatric News, “because they are better informants than fathers.”
The instruments that the researchers used to make these assessments included the Washington University at St. Louis Kiddie Schedule for Affective Disorders and Schizophrenia, the Children’s Global Assessment Scale, and the Psychosocial Schedule for School-Age Children—Revised.
Geller and her colleagues first analyzed their data to see how many of their subjects had recovered from mania at some point during the two-year study and how many of those who recovered subsequently relapsed during the same period. Recovery was defined as at least eight consecutive weeks without meeting DSM-IV criteria for mania or hypomania. Relapse after recovery was defined as two consecutive weeks of meeting DSM-IV criteria for mania or hypomania with clinically significant impairment.
The results were not especially encouraging. Only 58 (65 percent) of the youngsters were found to have recovered at some point during the two-year study, and of these 58, 32 (55 percent) had subsequently relapsed. The average time between recovery and relapse was 29 weeks. The average time to recovery was 36 weeks.
Geller and her colleagues also analyzed their data to see whether the types of treatments the children received influenced their bipolar outcomes. Analyses of medication effects were performed by combining data for drugs of a similar class or action (that is, lithium, any anticonvulsant, any neuroleptic, any antidepressant, any stimulant) and by a category of any antimanic drug (defined as lithium, any anticonvulsant, or any neuroleptic). Medications needed to be administered for at least two consecutive weeks to be counted. Psychotherapies that the children received included individual, group, or family therapy. To be considered for analysis, there needed to be at least four sessions within a consecutive eight-week period.
Here, too, results were not encouraging. For instance, the researchers found no significant difference in the rate of recovery in the 47 percent of the children who got lithium or an anticonvulsant drug than for the children who did not get such drugs. One possible explanation for such a finding, Geller and her coworkers pointed out in their study report, is that such therapies had a positive impact, but that it was not picked up because the therapies were given in naturalistic (community) settings, not in strictly controlled research environments.
Another possible explanation is that such treatments truly didn’t help. Bipolar children may simply be less responsive to mood-stabilizing drugs than bipolar adults are, Fred Volkmar, M.D., of the Yale University Study Center speculated in an editorial accompanying the study report. “There are currently no placebo-controlled trials of mood-stabilizing agents in children with bipolar disorder,” he noted.
But the study results were even more discouraging in that certain types of treatments seemed to make the children’s bipolar status even worse than it already was. For instance, youngsters who received a neuroleptic drug between the start of the study and recovery or between the start and end of the study—40 percent of subjects—were much less likely to recover than those children who did not get a neuroleptic drug under these conditions. And children who received either individual or group psychotherapy between the start of the study and recovery or between start and end of the study—54 percent of subjects—were much less likely to recover than those who did not get such therapy under these conditions.
It is possible, of course, that such treatments really had a malevolent impact on the outcome of the children who received them. But what is more likely, Geller and her colleagues proposed in their study report, is that psychosis rather than the treatments led to the children’s poor outcomes. Why might this be the case? The youngsters who got neuroleptics, individual psychotherapy, or group psychotherapy had significantly more psychosis at the start of the study than did the youngsters who did not receive neuroleptics, individual psychotherapy, or group psychotherapy.
The study produced one unexpected result, though. Children living with both biological parents were twice as likely to recover as were children living in other situations. This was an “unexpected finding,” Geller and her coworkers wrote.
David Rosenberg, M.D., a professor of psychiatry at Wayne State University, is familiar with this study by Geller and colleagues. It “is work of the highest scientific caliber. . .in a vastly understudied area,” Rosenberg told Psychiatric News. “[Geller and coworkers are] defining the outlook for youngsters with moderate to severe bipolar disorder. . . . [Their] work is going to ultimately result in better assessments and treatments for this severe, debilitating, and typically chronically disabling illness.”
Edwin Cook Jr., M.D., a professor of psychiatry at the University of Chicago, is also familiar with the study by Geller and her coworkers. “It’s excellent science,” he told Psychiatric News.” However, he said, “I’m not surprised at the results that earlier onset [of bipolar disorder] appears to be more severe than later onset. This is generally true of other disorders in medicine. . . .”
So what happens next in the research realm of Geller and company? They will continue to track the mental health outcomes of the children in this study until they become adults, Geller informed Psychiatric News. Also, she said, “We are conducting a family study of psychopathology in the first-degree relatives of these subjects.”
The study was funded by a grant from the National Institute of Mental Health.
The outlook for youngsters with moderate to severe bipolar disorder isn’t so favorable, a new study suggests. However, having an intact biological family can tilt the odds toward recovery.
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.