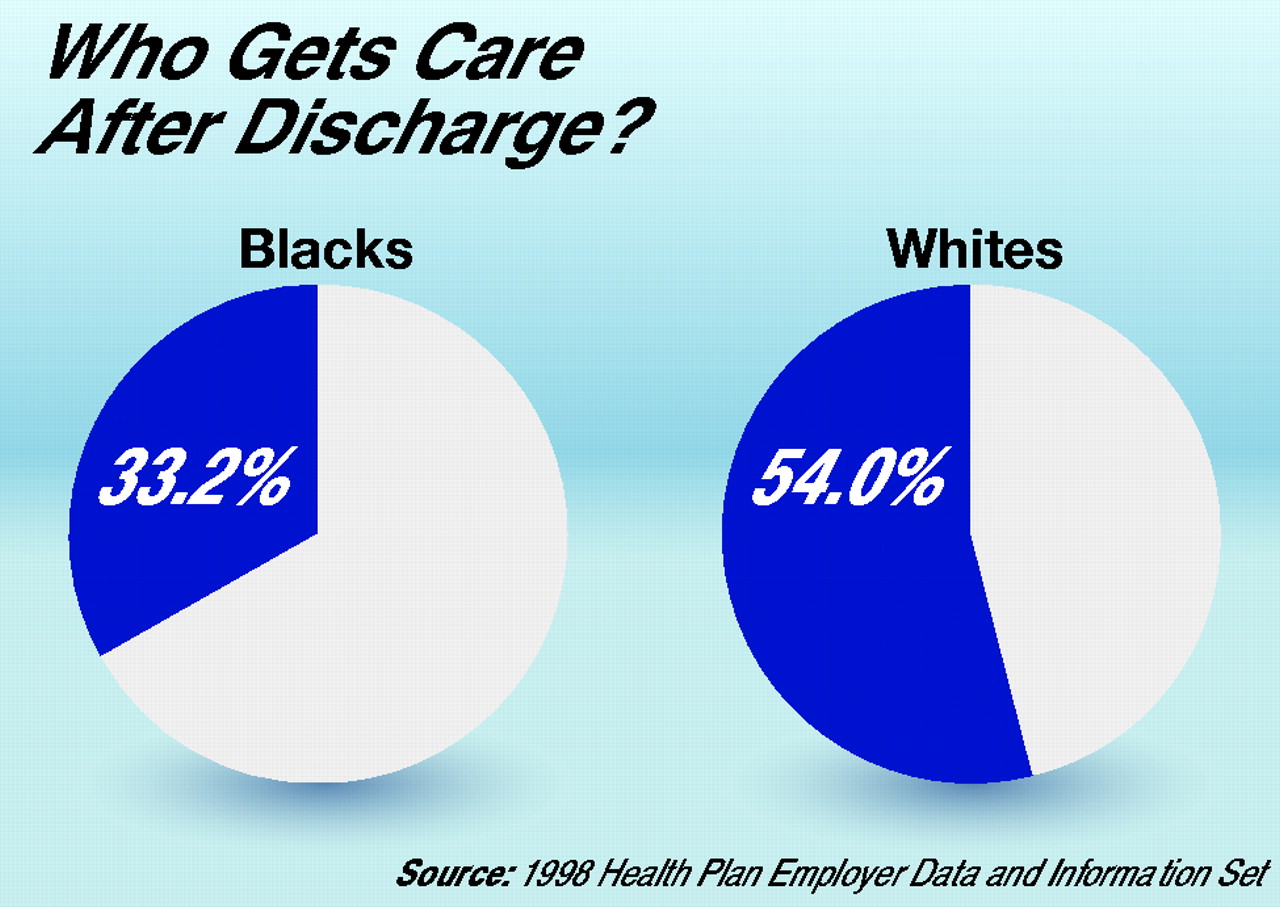
A study of 305,000 Medicare+Choice beneficiaries showed that whites are far more likely than blacks to receive follow-up care for mental illness after being discharged from the hospital.Medicare+Choice was authorized by the Balanced Budget Act of 1997 as a way to bring more managed care “benefits” to Medicare beneficiaries. But in the last few years, more and more managed care plans have withdrawn from the program, decreasing Medicare beneficiaries’ enrollment options.
In addition, those Medicare beneficiaries remaining in managed care plans—now less than 20 percent of Medicare beneficiaries—have been hit with increasing premiums and reduced benefits (Psychiatric News, December 21, 2001).
And now Medicare+Choice appears to have another failing as well: Black participants are receiving health care, including mental health care, that appears to be inferior to that of white participants.
This finding comes from Eric Schneider, M.D., of Harvard University School of Public Health and colleagues and is reported in the March 13 Journal of the American Medical Association.
Since 1997 all managed care plans participating in Medicare+Choice have been required to report, on an annual basis, Health Plan Employer Data and Information Set (HEDIS) measures of quality care to the Centers for Medicare and Medicaid Services. The Medicare HEDIS data for 1997, for example, included four yardsticks of quality care: breast cancer screening, eye exams for patients with diabetes, beta-blocker use for persons who had had heart attacks, and follow-up for individuals who had been hospitalized for mental illness.
So Schneider and his colleagues decided to analyze 1997 HEDIS data on about 305,000 beneficiaries enrolled in 294 Medicare managed care plans. The 305,000 beneficiaries in turn represented approximately 8 percent of the 4 million Medicare beneficiaries enrolled in Medicare+Choice in 1997.
Schneider’s study was designed to answer this question: Are blacks enrolled in Medicare+Choice receiving health care that is equivalent to that which whites enrolled in the program are receiving? The answer to that question is no, their study report revealed.
Black participants, they found, were significantly less likely than white participants to receive breast cancer screening, eye exams for diabetes, beta-blocker medication after heart attacks, and follow-up after hospitalization for mental illness, causing them to conclude, “Among Medicare beneficiaries enrolled in managed care health plans, blacks received poorer quality of care than whites.”
Their findings, however, were most disturbing in the mental health arena: The disparity between black and white participants was smallest for breast cancer screening and largest for follow-up after hospitalization for mental illness. In fact, as the researchers noted in their study report, “We know of no prior literature suggesting that blacks are less likely to receive follow-up after hospitalization for mental illness. The magnitude of this previously unrecognized disparity is formidable.”
So why might black participants in Medicare+Choice receive substantially less follow-up after hospitalization for mental illness than white participants? Socioeconomic factors are probably part of the explanation, but not the only one. The reason is that after Schneider and his colleagues adjusted their data for individual socioeconomic factors, racial disparities regarding follow-up after hospitalization for mental illness were somewhat smaller, but still statistically significant.
So might the reason that black participants get less follow-up after hospitalization for mental illness reside in quality differences between Medicare managed care plans? In other words, might blacks be more likely to get care in plans of lesser quality? The answer is probably no, for when Schneider and his coworkers reanalyzed their data with “dummy variables for individual health plans”—that is, a statistical method that controls for between-plan effects—the racial disparity regarding follow-up after hospitalization for mental illness was smaller, but still statistically significant.
So what other factors might explain why blacks in Medicare+Choice plans get less follow-up after mental illness hospitalization than whites in such plans? Schneider and his colleagues speculate that difficulty paying copayments for follow-up care, lack of transportation for follow-up care, reluctance to seek follow-up care because of the stigma, and insensitivity on the part of health care staff toward blacks might be among the reasons.
Michelle Clark, M.D., a Los Angeles psychiatrist and chair of the APA Committee of Black Psychiatrists, found the study sound and is not surprised by its conclusions, she said.
“It is very clear that there are [racial] disparities,” she asserted. “This has been the case for centuries. Everywhere you look there are disparities.”
One solution to these disparities is to educate health care personnel about the belief systems, fears, and health care needs that may be characteristic of black patients. “Just one good clinician in a system that is structurally racist, or shall we say ‘culturally incompetent,’ will not stem the tide.”
Psychiatric News also asked Altha Stewart, M.D., chair of the APA Council on Psychiatric Services and head of an APA task force to implement the Surgeon General’s recommendations on minority mental health care (see page 2), to comment on the findings.
Stewart said, “We’ve known for some 30 years that there are disparities between blacks and whites in terms of access to mental health care. So I can’t say that I am surprised that they reached the conclusion that, in addition to disparities in access, there are also disparities in the quality of care provided.”
In other words, she explained, “if you are a member of Medicare+Choice and black, you are less likely to not get the aggressive follow-up required to decrease the level of disability related to your mental illness. That translates into a lot of suffering, a lot of medical complications.”
Like Clark, Stewart believes one of the reasons for this disparity is that mental health care staff are not as competent in caring for blacks as they could be.
“Cultural competence is a nice concept,” Stewart said, “but it hasn’t been fully integrated into the overall health care delivery system.
“I think that has to be the next big change that happens,” Stewart said. “We do not have enough black doctors to see black patients, or Hispanic doctors to see Hispanic patients, or Asian doctors to see Asian patients. We’ve got to cross the great divide so that the health care provider recognizes the need to become competent across cultures in providing service, so that whoever walks into the office gets the best possible care based on who they are.”
The study by Schneider and his coworkers was funded by the Commonwealth Fund and the federal Agency for Healthcare Research and Quality.
An abstract of the article, “Racial Disparities in the Quality of Care for Enrollees in Medicare Managed Care,” is posted on the Web at www.jama.ama-assn.org/issues/v287n10/abs/joc11037.html. ▪
Add to the growing list of complaints about Medicare+Choice that it also appears to provide lower-quality health care, including mental health care, to African Americans.
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
Get Access
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.