At first glance, the big picture about eliminating discriminatory coverage of mental illness looks good, according a study reported in the September-October Health Affairs.
But lead author Colleen Barry and her colleagues ultimately concluded that without “broader parity laws, progress toward benefit parity could prove difficult to achieve.”
The authors used data from the 2002 national survey about health care benefits conducted by the Henry J. Kaiser Family Foundation and Health Research and Educational Trust (KFF/HRET) of 2,014 randomly selected public and private firms. Since firms are selected randomly, statistical weighting enables researchers to draw both national conclusions and conclusions about various subsets of data, such as benefits related to firm size and region of the country.
The authors tracked trends by comparing results from previous studies with the KFF/HRET results.
Ninety-eight percent of workers with employer-sponsored health insurance had coverage for mental health care in 2002, according to the KFF/HRET survey.
Large firms were significantly more likely than small ones (those with three to 199 workers) to offer mental health benefits.
From 1991 to 2002, the proportion of covered workers offered mental health benefits increased, according to a comparison of data from three surveys. For outpatient care, the respective percentages for 1991, 1995, and 2002 were 86 percent, 92 percent, and 98 percent covered.
The authors noted, however, that firms continue to place special limits on mental health benefits. Loopholes in federal and state parity laws permit “persistent differences in coverage between mental health and general medical benefits.”
The Mental Health Parity Act (PL 104-204), for example, prohibits annual or lifetime dollar limits on coverage for mental illnesses unless equal dollar limits apply to other medical services. It does not, however, mandate nondiscriminatory coverage for day and visit limits and copayments.
The authors cited a study by the General Accounting Office (GAO/HEHS-00-05) that found that about two-thirds of employers who complied with the law made at least one other mental health benefit design feature more restrictive.
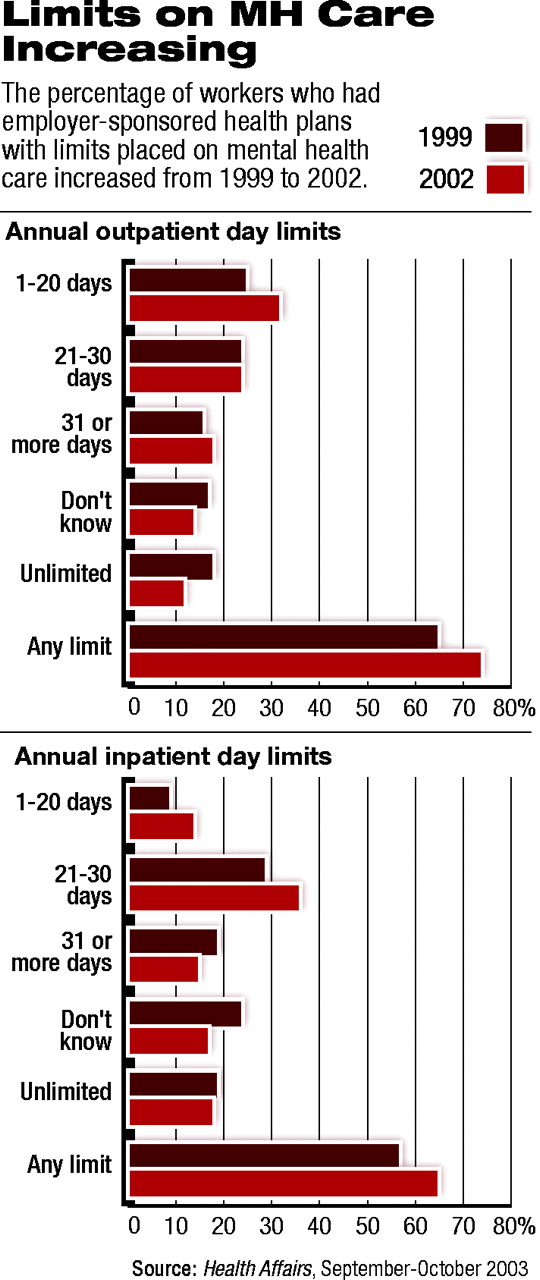
According to the KFF/HRET survey, the majority of covered workers in 2002 were still subject to day and visit limits for mental illness. Seventy-four percent of covered workers were subject to an annual outpatient-visit limit, and 64 percent were subject to an annual inpatient-day limit.
In fact, it appears that day and visit limits for mental health benefits have increased. The proportion of covered workers subject to outpatient-visit limits increased from 65 percent in 1999 to 74 percent in 2002. Fifty-seven percent of covered workers had inpatient-day limits in 1999, compared with 65 percent in 2002. A higher number of firms reported “don’t know” in 1999, complicating the comparison (see chart).
Cost sharing represents another tool by which employers control costs for benefits. According to the authors, the federal Bureau of Labor Statistics found that a majority of enrollees in medium and large firms during the 1980s paid a 50 percent coinsurance rate for outpatient mental health care, rather than the usual 20 percent paid for other illnesses.
The 2002 KFF/HRET survey data showed a decrease to 22 percent of covered workers with higher cost sharing for mental health benefits.
Barry and her colleagues speculated that people covered for mental illness under HMOs or through carveouts might be less likely to be subjected to cost sharing and benefit limits than those who are not in HMOs or subject to carveouts.
Their reasoning was that managed care, in theory, was intended to produce savings that could be used to expand benefits.
The authors found, however, that “nominal benefits under HMOs and carveouts tend to be at least as restrictive as conventional plans.”
They speculated that “benefit restrictions could be motivated by a health plan’s desire to avoid enrollees with a propensity to avail themselves of mental health care.”
“Design of Mental Health Benefits: Still Unequal After All These Years” can be accessed for a fee at the Web site of Health Affairs at www.healthaffairs.org; access is free to subscribers. ▪
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
For more information or tips please see 'Downloading to a citation manager' in the Help menu.
View Options
View options
Login options
Already a subscriber? Access your subscription through your login credentials or your institution for full access to this article.
PsychiatryOnline subscription options offer access to the DSM-5-TR® library, books, journals, CME, and patient resources. This all-in-one virtual library provides psychiatrists and mental health professionals with key resources for diagnosis, treatment, research, and professional development.
Need more help? PsychiatryOnline Customer Service may be reached by emailing [email protected] or by calling 800-368-5777 (in the U.S.) or 703-907-7322 (outside the U.S.).
If the address matches an existing account you will receive an email with instructions to retrieve your username
Create a new account
Change Password
Password Changed Successfully
Your password has been changed
Login
Reset password
Can't sign in? Forgot your password?
Enter your email address below and we will send you the reset instructions
If the address matches an existing account you will receive an email with instructions to reset your password.
Change Password
Congrats!
Your Phone has been verified
×
As described within the American Psychiatric Association (APA)'s Privacy Policy and Terms of Use, this website utilizes cookies, including for the purpose of offering an optimal online experience and services tailored to your preferences. Please read the entire Privacy Policy and Terms of Use. By closing this message, browsing this website, continuing the navigation, or otherwise continuing to use the APA's websites, you confirm that you understand and accept the terms of the Privacy Policy and Terms of Use, including the utilization of cookies.