Patients are more likely to continue taking second-generation antipsychotics than older antipsychotics, potentially improving overall outcomes simply through improving medication adherence, three new studies suggest.
The studies were presented as poster abstracts at the International Congress on Schizophrenia Research (ICOSR) in Savannah, Ga., in April. Each of the three addressed some aspect of time to relapse in patients with schizophrenia. They were funded by Eli Lilly and Co., maker of the Zyprexa brand of olanzapine.
Olanzapine is a close chemical offspring of clozapine, the first second-generation antipsychotic. It was specifically developed in an attempt to maintain the high efficacy of clozapine for positive symptoms while mitigating the severe blood dyscrasias associated with the parent compound. Olanzapine has done well in these two areas, but other side effects have become apparent, including significant alterations of lipid and glucose metabolism potentially leading to cardiovascular disease and diabetes.
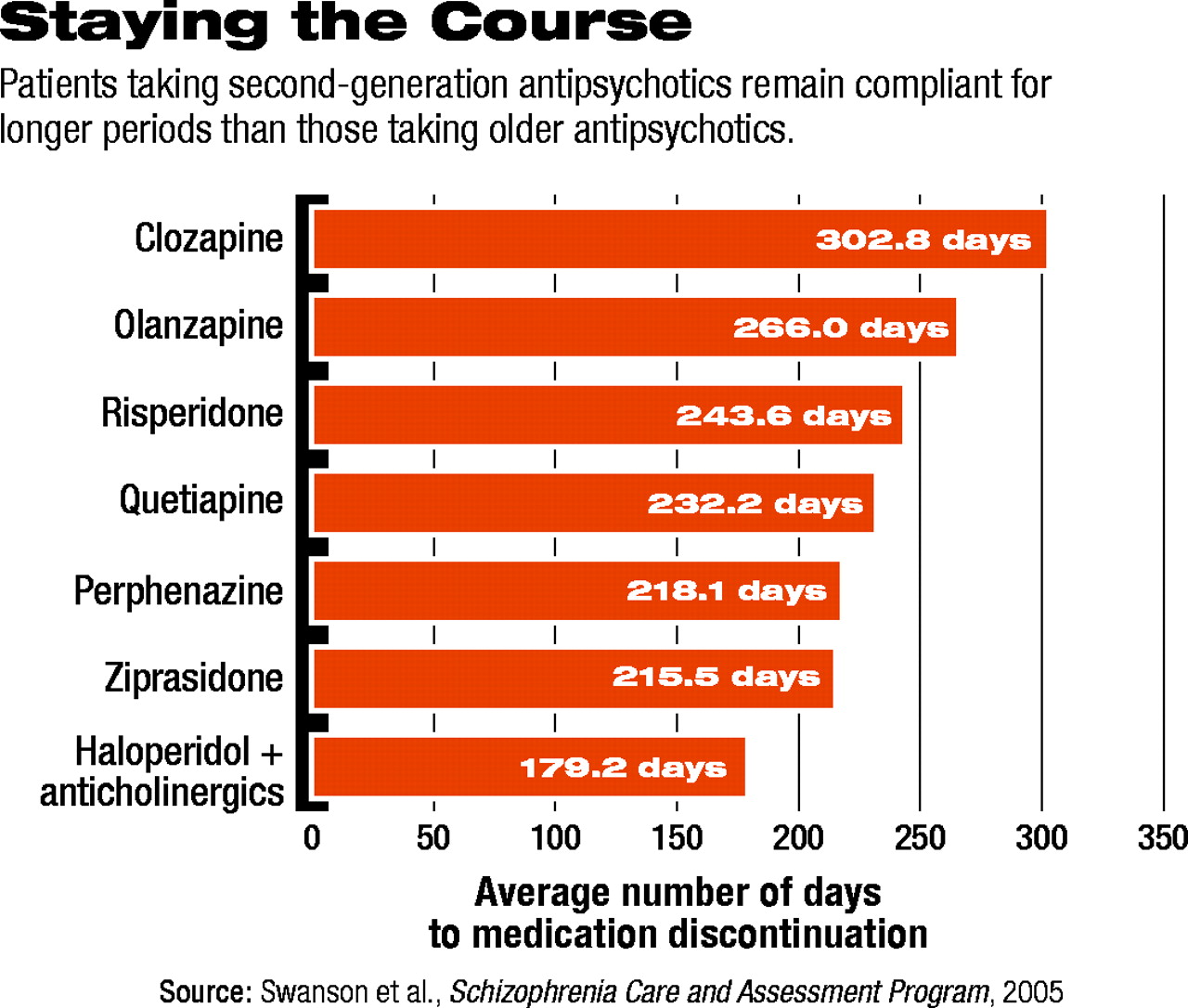
One study presented at ICOSR showed that patients taking clozapine or olanzapine continue taking their medication significantly longer than patients taking other second-generation antipsychotics (risperidone, quetiapine, or ziprasidone; aripiprazole was not available at the time the study was conducted) or the typical antipsychotic perphenazine.
“You have to buy into the idea,” said Jeffrey Swanson, Ph.D., an associate professor of psychiatry and behavioral sciences at Duke University and study leader, “that [time to discontinuation] is a sort of proxy measure for effectiveness—that if people remain on their medication, then it is tolerable enough for them to continue taking it, and their physician hasn't stopped the medication because of lack of efficacy or adverse effects.”
Swanson and his colleagues collected their data as part of the Schizophrenia Care and Assessment Program (SCAP), funded by Lilly. SCAP was a three-year naturalistic, observational, prospective study of 2,327 patients. The study enrolled ethnically diverse patients at Veterans Affairs medical centers, community mental health clinics, community and state hospitals, and university-based health care systems across the country. Each patient was systematically assessed at six-month intervals over the study period.
Patients taking clozapine remained on their medication significantly longer on average than patients on the other antipsychotic medications (303 days; see chart at right). Olanzapine was second, followed by risperidone and quetiapine. In contrast, patients taking haloperidol, even when compensated by anticholinergic medications, discontinued their medication earlier than any other group, after only 179 days.
“The results for clozapine are very strong, and strong for olanzapine,” Swanson noted, “and that is consistent with previous research. If this were the only study to indicate this type of pattern, one would have to be more skeptical. But this falls in line with an accumulating literature, so I think it is an important finding.”
Swanson added, “I'm less confident that the relatively negative results for the last two drugs to be introduced [during the course of the study], quetiapine and ziprasidone, really mean a whole lot.”
Patients on these two drugs, Swanson explained, may represent some component of treatment resistance. As new drugs became available, patients may have been put on the latest medication simply because the medication they were already taking was not working well for them. That could include, Swanson said, some patients who did not respond well to olanzapine.
Swanson is also an investigator for the National Institute of Mental Health's Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE), which is a 10-year study of differential effectiveness between first- and second-generation antipsychotics.
“I think there are some very valuable synergies there,” he told Psychiatric News. “CATIE and SCAP look very similar in some of the important baseline characteristics,” he said.
The second study presented at ICOSR detailed data collected by Alan Green, M.D., chair of psychiatry at Dartmouth Medical School. Green's data directly link a longer time to discontinuation with significantly greater improvements in clinical and functional outcomes. The third ICOSR poster abstract, led by John Davis, M.D., a professor of psychiatry at the University of Illinois at Chicago, presented a meta-analysis of continuation on antipsychotic medication in randomized, double-blind clinical trials, again showing an advantage for clozapine and olanzapine, relative to risperidone, ziprasidone, and haloperidol.
More information on the International Congress on Schizophrenia Research is posted online at<www.schizophreniacongress.org>.▪