A recent rise in teen suicides recently ended a long, steady decline in such deaths.
The rate of suicides among youngsters and young adults aged 10 to 24 increased by 8 percent from 2003 to 2004 to total of 4,599 deaths. The jump in deaths among this age group, announced in September by the Centers for Disease Control and Prevention (CDC), was particularly pronounced among girls aged 10 to 14, among whom the number of suicides jumped by 76 percent. Suicides were also up 32 percent among girls aged 15 to 19, and 9 percent among boys aged 15 to 19.
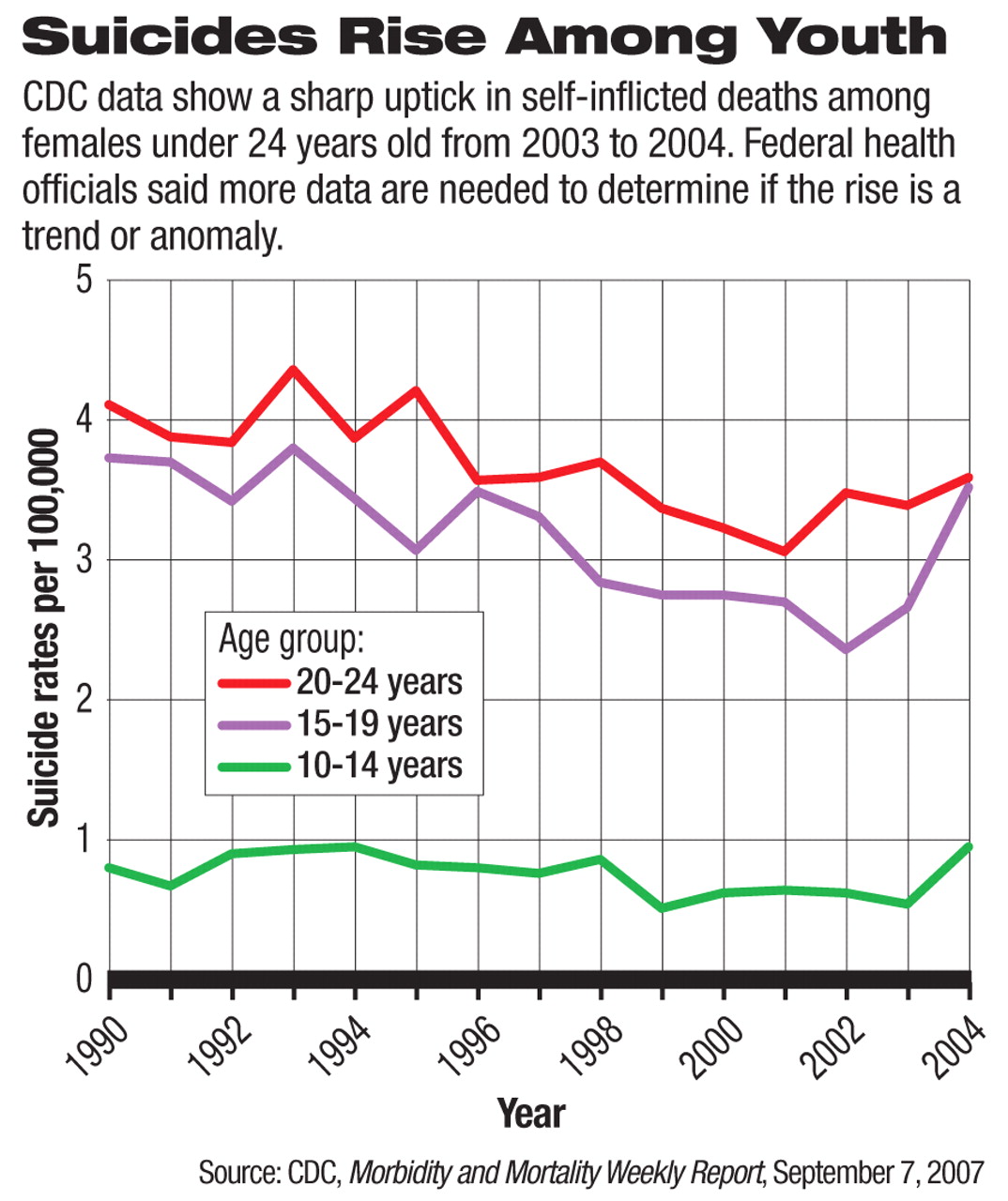
The CDC found that the spike occurred after 14 years of declines in youth suicide. The suicide rate dropped 19 percent from 1990 to 2003 before the sharp rise in 2004, which was the most recent year data were collected.
“This is the biggest annual increase that we've seen in 15 years,” said Ileana Arias, Ph.D., director of CDC's National Center for Injury Prevention and Control. “We do not yet know if this is a short-lived increase or if it's the beginning of a trend.”
The method many young girls use to commit suicide also has changed. In 2004 hanging or suffocation was the most common method among girls in all age groups and accounted for 71 percent of suicides among girls aged 10 to 14, 49 percent of suicides in girls aged 15 to 19, and 34 percent of suicides among young women aged 20 to 24.
A particularly dramatic jump in the rate of suicide by hanging or asphyxiation was found in girls aged 10 to 14. In 2004 the rate was 6.8 per 1,000,000 population, but in the years since the CDC began keeping records on suicides in 1990, this rate was never higher than 3.5 per 1,000,000 girls in the same age group, according to the report in the September 7 Morbidity and Mortality Weekly Report.
“So while we can't say this is a trend, we are confident that that is definitely an usually high number in 2004,” said Keri Lubell, Ph.D., one of the study authors in comments at a press conference.
The report's authors theorized that the trend toward hanging and asphyxiation is linked to a choking game that has recently become popular among youngsters. Although the CDC does not believe that a significant number of these deaths have been misclassified as suicides, it remains unclear whether the game is linked to the growing acceptability of hanging and asphyxiation as a suicide method.
Black-Box Link Questioned
The surge in teen suicide also coincides with a drop in prescribing of antidepressant medications after the Food and Drug Administration mandated the addition of warning language to the labels of antidepressants about possible links between their use and suicide among children, adolescents, and young adults (see
Suicide Data Prompt Call for Black Box Review).
Reported prescriptions of antidepressants for children and adolescents decreased by 19 percent in the third quarter of 2004 and 16 percent in the fourth quarter of 2004, compared with the year before, according to an article in the September Pediatrics that cited data from pharmacy benefit manager Medco Health Systems.
Some psychiatrists and other researchers believe that the decline in antidepressant prescribing is responsible for the surge in teen suicides.
A growing body of research bolsters the position that antidepressants effectively treat depression. An example of the effectiveness of such medications in adolescents was documented in a study by John March, M.D., and others in the August 18, 2004, Journal of the American Medical Association that found that a combination of an antidepressant and cognitive-behavioral therapy led to significant clinical improvement in 71 percent of adolescents with major depression. That outcome was compared with improvement of 61 percent for the medication alone, 43 percent for cognitive-behavioral therapy alone, and 35 percent for placebo, according to the study (Psychiatric News, September 3, 2004).
FDA Awaits More Evidence
Regardless of the data on the benefits of antidepressants outweighing the risks, the FDA will need to see more evidence over time before the agency will consider linking declines in prescriptions to a growth in suicide risk and revisiting any of its previous warnings, said Thomas Laughren, M.D., director of the Division of Psychiatry Products at the FDA, in a September 6 conference call with reporters. “It's true that antidepressant prescribing in pediatric patients has come down. And that coincides with this one-year uptick in adolescent suicide, so obviously that's a concern,” Laughren said.“ On the other hand, we do, as a regulatory agency, have an obligation to alert prescribers and patients of risks that we find with drugs that are being used. So it's a dilemma for us, but clearly it's a concern.”
In December 2006, an FDA advisory committee urged antidepressant medication product labeling to reflect the apparent beneficial effect of antidepressants in older adults and to remind health care professionals about the danger of untreated depression (Psychiatric News, January 19). As a result, this past summer the FDA required manufacturers of antidepressants to include on their labeling the statement, “Anyone considering the use of [name of antidepressant] or any other antidepressant in a child, adolescent, or young adult must balance this risk with the clinical need.... Depression and certain other psychiatric disorders are themselves associated with increases in the risk of suicide.”
It is possible that some subgroups of patients become more suicidal when given antidepressants, Laughren said, while the larger population benefits.
Thomas Anders, M.D., president of the American Academy of Child and Adolescent Psychiatry (AACAP), urged physicians, educators, parents, and teens to learn the signs of suicidal behavior and to take action and seek help when they see those signs.
The significant increase in adolescent suicides demonstrates the need for more information on how to prevent violent deaths, including suicide, according to Sean Gerow, chair of the board of directors of the Suicide Prevention Action Network USA (SPAN USA).
The CDC suicide data, which federal health officials describe as likely underestimating the extent of the problem, are based on the National Violent Death Reporting System (NVDRS), which collects data from medical examiners, coroners, police, crime labs, and death certificates to understand the circumstances around violent deaths, including suicides. The system's data, however, come from only 17 states.
SPAN USA has urged a $1.5 million federal expansion of the NVDRS.
The CDC “Morbidity and Mortality Weekly Report” is posted at<www.preventviolence.net/pdf/MM5635%20eBook.pdf>. AACAP's “Practice Parameter for the Assessment and Treatment of Children and Adolescents With Suicidal Behavior” is posted at<www.aacap.org/galleries/PracticeParameters/Suicide.pdf>.▪