On average, one person died by suicide every 15 minutes from 2001 to 2009 in the United States, which translates into more than 33,000 people each year in that period.
Currently, suicide is the 10th-leading cause of death for Americans and second-leading cause of death among youth. In the past year, more than 8 million adults report having had serious suicidal thoughts, 2.5 million made a suicide plan, and 1.1 million reported a suicide attempt, according to a new report from the U.S. surgeon general and the National Action Alliance for Suicide Prevention (Action Alliance), which is made up of approximately 200 public and private organizations that advocate for achieving a suicide-free nation.
This report is the vehicle for a new updated national strategy to reduce the number of deaths by suicide in the United States over the next 10 years. The new strategy was released in Washington, D.C., on September 10, which was National (and World) Suicide Prevention Day. Secretary of Health and Human Services Kathleen Sebelius, U.S. Surgeon General Regina Benjamin, M.D., Deputy Secretary of Veterans Affairs (VA) Scott Gould, and Administrator of the Substance Abuse and Mental Health Services Administration Pamela Hyde were among the speakers at the event.
“We must take action against suicide together. It starts with reducing stigma,” Sebelius emphasized at the press event. “We have a long way to go, but now we have a roadmap to get there.”
The new national strategy was called for by Sebelius and former Department of Defense Secretary Robert Gates when they launched the Action Alliance in September 2010 in hopes that a new strategy would reflect major developments in research on and understanding of suicide prevention.
The previous national suicide-prevention strategy, created in 2001, used an AIM (Awareness, Intervention, and Methodology) framework. The new plan defines and expands more goals and objectives across broader “strategic directions.”
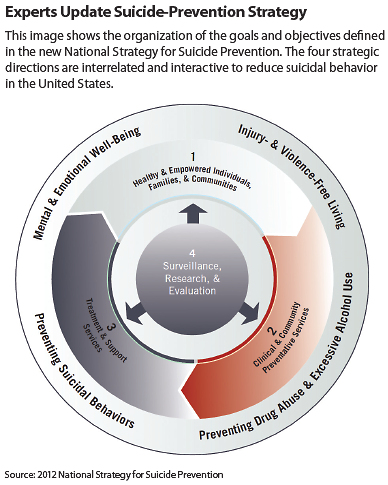
Sixty objectives and 13 goals are organized into four strategic directions (see figure) that are interrelated and interactive rather than separate, such as was the case with the AIM approach.
The strategic directions are described as
•.
creating supportive environments that promote health and empower individuals, families, and communities,
•.
enhancing clinical and community-based preventive services,
•.
promoting the availability of timely treatment and support services, and
•.
improving surveillance, data collection, research, and evaluation regarding suicide-prevention efforts.
Together, these four strategic directions are designed to focus the nation in general and physicians and health care professionals in particular on encouraging dialogue about suicidal behavior and promoting treatment programs and recovery. The 60 objectives within the four strategic directions update, revise, or replace the 2001 goals and objectives to reflect advances in knowledge and areas where goals or actions have been completed.
“Since at least 90 percent of the people who die by suicide have a mental disorder at the time of their deaths, the task of recognizing and treating those mental disorders is central to changing the suicide rate,” said psychiatrist Paula Clayton, M.D., medical director of the American Foundation for Suicide Prevention, in an interview with Psychiatric News. “So anything, as some of their goals do, that aims to decrease stigma about having a mental disorder or receiving treatment for it or improves continuity of care from one point of service to the next should help reduce suicide rates.”
She continued, “The public needs to be educated that severe depression, alcoholism, drug abuse, bipolar disorders, anxiety disorders, schizophrenia—in fact all mental disorders—can lead to death by suicide and be alerted to the warning signs that might help prevent that.”
“We want system changes, and systematic changes,” said Benjamin at the event. “We want you to talk.”
In conjunction with the new strategy, the Obama administration announced activities that will aid in suicide-prevention efforts that include $55.6 million in new grants for national, state, and local community suicide prevention programs. The grants are mostly funded through the Garrett Lee Smith Memorial Act with additional funding by the Prevention and Public Health Fund under the Affordable Care Act of 2010.
In addition to the strategies announced last month, the VA also launched a new outreach campaign called Stand by Them: Help a Veteran, which partners the Department of Defense (DoD) with the VA to focus on support from families and communities to prevent suicide among veterans.
“Successful prevention programs need to cut across all of our society. Nothing is more essential than communication,” said Secretary of the Army John McHugh about the Stand by Them campaign “How we communicate has changed.”
The VA and DoD are reaching out to local communities to connect veterans and service members to community resources, such as the Veterans Crisis Line. The Veterans Crisis Line has received more than 650,000 calls and has saved more than 23,000 lives, explained Gould, and the crisis line will be doubling its workforce by hiring an additional 1,600 mental health professionals.
“Our message today is one of hope,” said Sebelius. “The national strategy will bring together the nation’s resources, both public and private, in an organized effort to provide lifesaving services and improve the ability of individuals, friends, and family members to recognize the warning signs of despair and take action to save lives.”