Sample
One hundred ninety-nine elders were enrolled in the study, and they were hospitalized for major depression on a 34-bed geropsychiatric unit of a large urban hospital and discharged home between March 1997 and May 2000. Only patients discharged to the community were considered in our study because home is the place where most patients go after discharge. Our study focus was the relationship between needs met through community-based services and depression outcomes after patients had been discharged from the hospital.
A consecutive 568 admissions were screened for study eligibility. Inclusion criteria were that depression was the primary reason for hospitalization, patients met DSM-IV axis I depression criteria, and the destination after discharge was a community setting rather than a nursing home, hospital, or other institutional setting. The medical director of the geropsychiatric unit, a geropsychiatrist, reviewed each patient's diagnoses. After routine cognitive testing and observation of patients, nurses provided information about the cognitive status of patients who met the inclusion criteria. If a nurse reported that cognitive impairment prevented informed consent, we obtained assent from the patient and consent from a family member. We excluded two patients who could not provide reliable information because of cognitive impairment and not having a collateral source of information. Of 269 eligible patients hospitalized during the study period, 199 patients (74 percent) consented to participate. Gender, race, marital status, and age did not vary between study participants and those who refused. The human studies committee of the university approved data collection and protocol of the study, and all participants gave informed consent.
At patients' discharge, research assistants abstracted medical records and baseline measures and interviewed the study participants. Service use was assessed from self-reports of depressed elders. Despite some inaccuracy, self-reports are efficient and are commonly used to measure service use (
21,
22,
23 ). When study participants could not be interviewed because of cognitive impairment, we interviewed their family members (62 proxies at six weeks, or 31 percent; 22 proxies at six months, or 11 percent). Service use was assessed by research assistants through telephone interviews conducted six weeks after discharge, and 186 of 199 participants (response rate of 93 percent) were interviewed. The six-month service use and outcome assessment was conducted during in-home interviews, and interviews were attempted with all 199 participants except three who had died within six weeks of discharge. The response rate was 87 percent, and 174 persons were interviewed.
Of 199 patients who were initially discharged to the community, only 148 were living in the community six months after discharge. Excluded from our analyses were 51 elders, including 20 who moved to nursing homes during the six months, 13 who died, and 18 lost to follow-up for other reasons, such as refusal to participate or our inability to locate them. Those included in the sample and those in the three excluded groups (those in nursing homes, deceased, or lost to follow-up) did not differ in terms of gender, age, race, living areas, or depressive symptoms at discharge. For instance, Geriatric Depression Scale (GDS) (
24 ) scores, which could range from 0 to 30, with higher scores indicating depressive symptoms, were not significantly different between those included in the sample (mean±SD=12.4±6.7) and the three excluded groups (in nursing homes, 13.4±8.0; deceased, 12.3±6.9; lost to follow-up, 12.1±8.2).
Measures
Needs met for quality of care. Quality of postacute care was measured by assessing the extent to which service needs were met. Following a recommendation by Dickey and colleagues (
25 ), we developed our criteria for assessing whether needs were met by using evidence- or consensus-based standards of care and disorder-specific treatments, which were assumed to yield the best clinical outcomes. As reported elsewhere (
11,
26 ), and consistent with a biopsychosocial perspective on mental disorder (
27 ), we assessed service needs at discharge in four domains: psychiatric, medical, functional, and psychosocial.
Specifically, using standardized instruments and review of medical records for services ordered at discharge, we identified 11 service needs: five potential service needs in the psychiatric domain (psychiatric care, electroconvulsive treatment, monitoring of psychotropic medication, psychotherapy, and supervision for cognitive impairment), two potential service needs in the medical domain (medical care and monitoring medication for chronic conditions), two potential service needs in the functional domain (human assistance for dependencies in activities of daily living and human assistance for dependencies in instrumental activities of daily living), and two potential service needs in the psychosocial domain (socialization services and casework or counseling for psychosocial situations).
In the psychosocial domain, socialization services included visiting an adult day care center, senior center, or senior citizen club; participating in a telephone support program; or seeing a companion, friendly visitor, or hospice visitor. The following services were included in casework or counseling in the psychosocial domain: counseling about psychosocial problems with a psychiatrist or other professionals, such as another doctor, a mental health specialist, a cleric, or a medical social worker; attending an adult day care center, senior center, or day treatment program or partial hospice program for counseling; meals services; transportation services; family support groups; telephone services, although not for socialization; legal or financial services; caseworker services; or social services.
Needs were coded as met in a given domain if a patient had at least one service encounter for each needed service type. For example, if the medical record reflected that a follow-up appointment with the admitting psychiatrist was arranged, and if the patient went home with a prescription for psychotropic medication, that patient was deemed to need two types of psychiatric service. The domain was coded as "needs met" if the patient received at least one service corresponding to each of the two types of psychiatric service—that is, at least one appointment with the psychiatrist and at least one contact with a professional in which medication compliance and side effects were assessed.
We determined whether needs were met in each domain six weeks after discharge (six-week needs-met variables) and six months after discharge (six-month needs-met variables). For each patient, each of the four domains of service need was coded as needs met, needs unmet, or no need. Because every patient had psychiatric needs by virtue of study eligibility, the no-need category was not applicable for quality of psychiatric care. Each quality-of-care variable was dummy coded with a reference group of "needs met" for statistical analyses.
Depression outcomes. Depression was measured by the GDS, developed to assess depressive symptoms specifically for older adults (
24 ). Higher scores on the GDS (range 0-29) represent greater depressive symptoms, and the mean score at discharge and at six months was 12.6±6.6 and 12.0±7.2, respectively. Reliability (
α =.94) and validity of the GDS are well documented (
24 ).
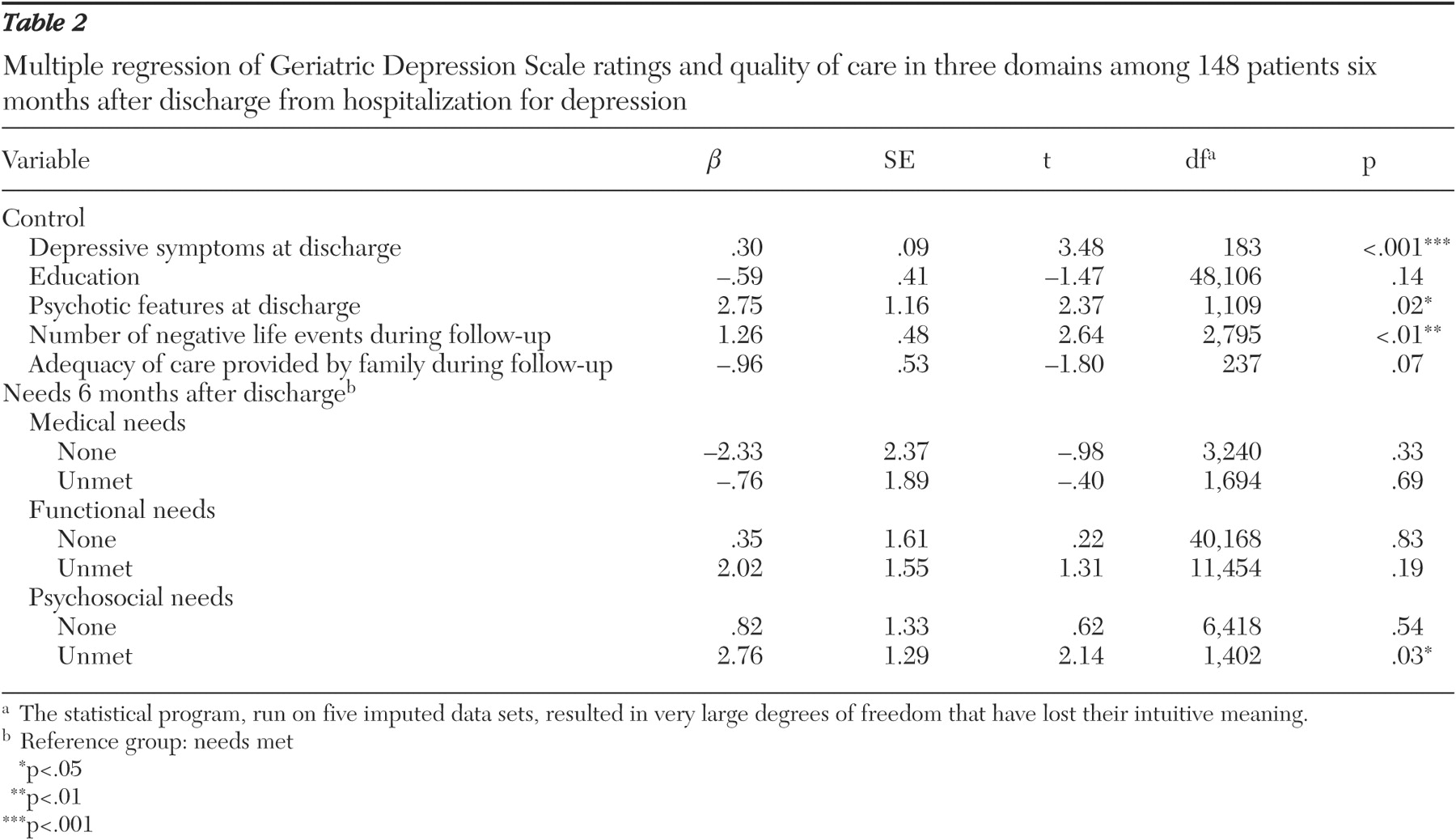
Control variables. Variables that were empirically related to depression outcomes in the literature and that were significant in our bivariate analyses were used as control variables. We identified as control variables education, presence of psychotic features, the number of negative life events, and adequacy of care provided by family caregivers. Education was measured by a 5-point scale (from 1, eighth grade or less, to 5, undergraduate degree or higher); 87 patients (59 percent) attained an education level of at least graduation from high school. Forty-five patients (30 percent) exhibited psychotic features assessed by the geropsychiatrist's clinical judgment during the hospital stay. The number of negative life events during the six months after discharge from hospitalization was assessed through the Duke Life Events Scale (
28 ) in the interviews at six months. We asked whether older adults experienced 14 events (for example, "Did you experience an illness or injury that required staying overnight or longer in the hospital?") and then counted the number of events that they perceived as negative (sample mean, .95±1.13, range 0-5). Adequacy of care provided by family caregivers was rated by the patient's social worker at discharge (from 1, poor care, to 5, excellent care; 3.69±1.18).
Data analyses
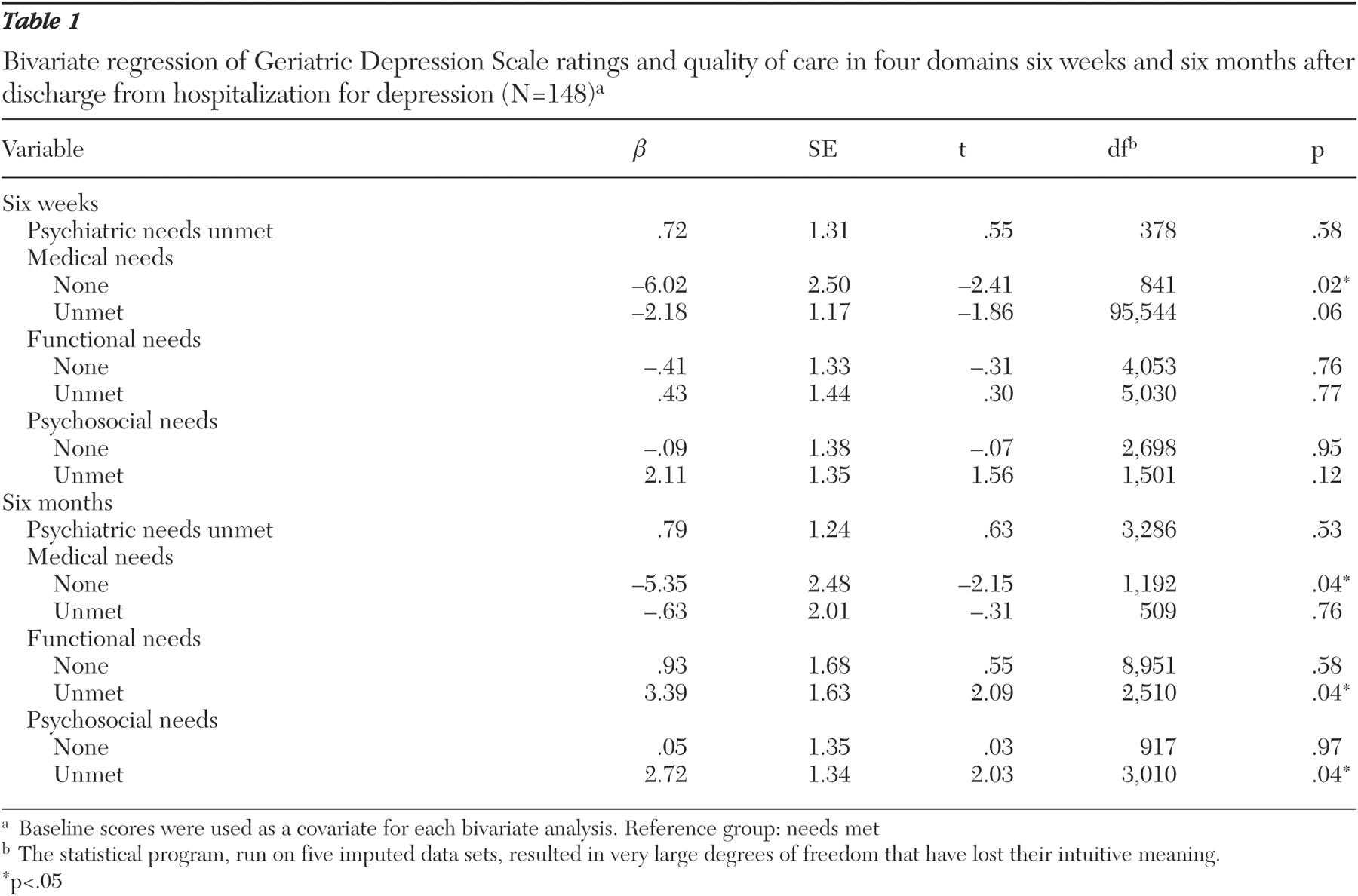
We ran bivariate analyses for depression outcomes with four domains of six-week and six-month needs-met variables after controlling for GDS scores at discharge. By controlling the baseline scores as a covariate, we avoided the statistical unreliability of change scores and made groups comparable from the same baseline score (
29 ).
To select control variables for multivariate analyses, we performed bivariate analyses. Because of nonsignificant results of the bivariate analyses, we eliminated age, gender, race, living areas, marital status, cognitive impairments, self-rated health, functional status, medical comorbidity, first episode of mood disorder, onset age of mood disorder, electroconvulsive treatment during hospitalization, suicide attempts during the month before hospitalization, income, private insurance coverage, and service use barriers. Only education, presence of psychotic features, the number of negative life events, and adequacy of care provided by family caregivers were associated with depression outcomes in bivariate analyses (p<.05), and they were included in the multivariate model. The significance level was set at p<.05 in multivariate models. Because depression outcome variables were measured continuously, we ran bivariate and multiple ordinary least-squares regression models.
Data on depression ratings were missing for 33 patients (22 percent) at discharge and for seven patients (5 percent) at the six-month follow-up. Data for some control variables also were missing. For missing data, we used the multiple random imputation method to generate five independent data sets without missing data (
30 ). This method assumes that missing data occur randomly. Each missing value is filled in with a set of plausible values that are created with information from other values of a variable and some associated variables (such as physical health and depression outcome), which usually do not have missing data (
30 ). After generating the five imputed data sets, we performed identical analyses on each data set and combined or "rolled up" the results to yield less biased parameter estimates in the overall regression model. This method is superior to other kinds of imputation methods, such as mean substitution, hot decking, regression imputation, and single imputation, in terms of producing more accurate estimates (
30 ).