Help seeking for alcohol problems among American Indians appears relatively high (
8,
17,
18,
19 ) and includes significant use of traditional healing resources (
17,
20 ). However, existing information about help seeking among American Indians has been constrained by a narrow focus on specific subgroups (
17,
20,
21 ) and has not included a full complement of need variables, such as those suggested by other studies (
22,
23,
24,
25,
26,
27 ). For example, although comorbid alcohol and mental health disorders are common, little is known about help seeking among persons with co-occurring conditions. Furthermore, although the overlap in help seeking from biomedical, traditional, and 12-step treatment modalities is thought to be extensive, we have little supporting empirical evidence. Finally, despite substantial ethnographic evidence on the importance of spirituality and ethnic identity (
28,
29 ), their roles have yet to be investigated, especially as they relate to the type of help sought.
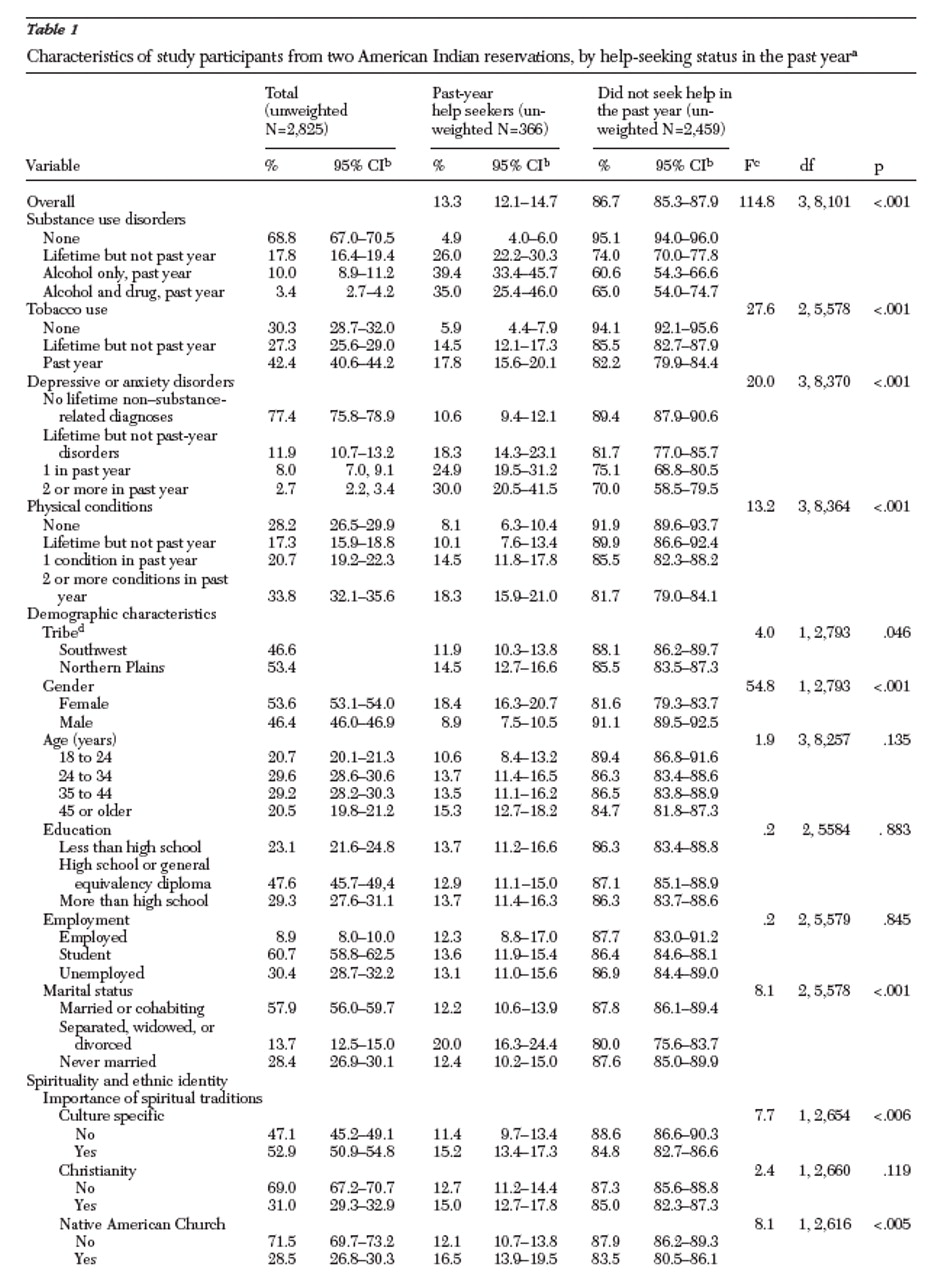
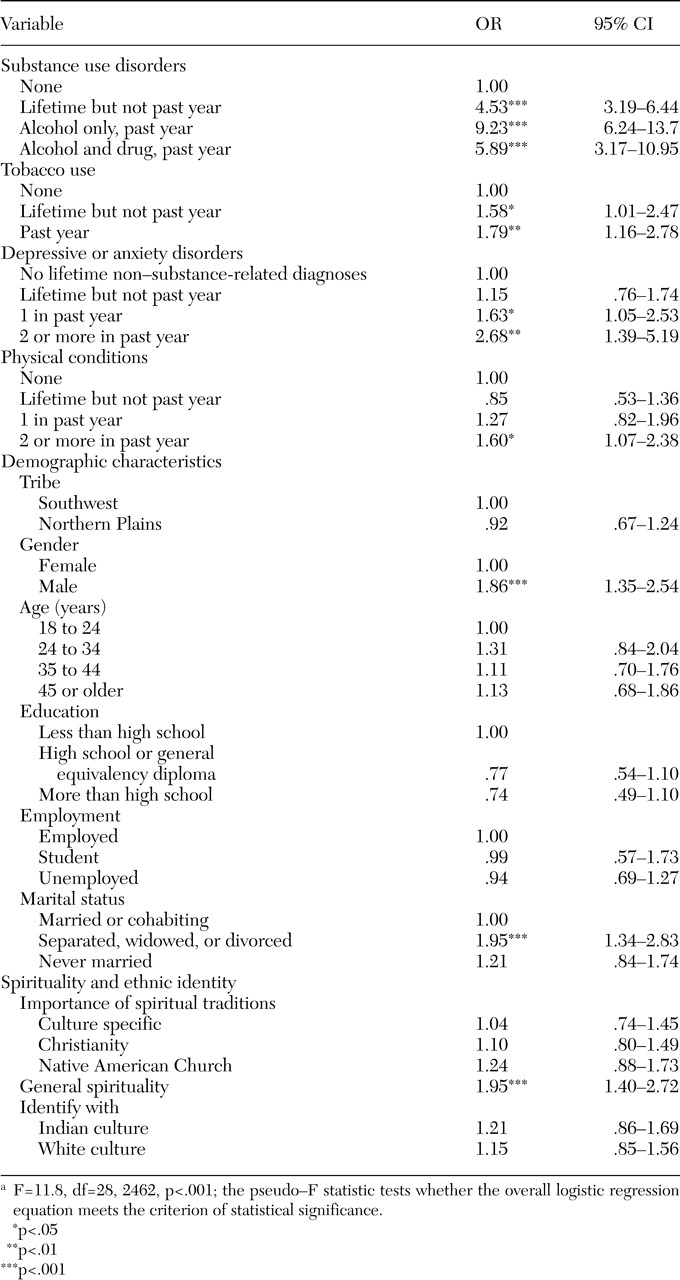
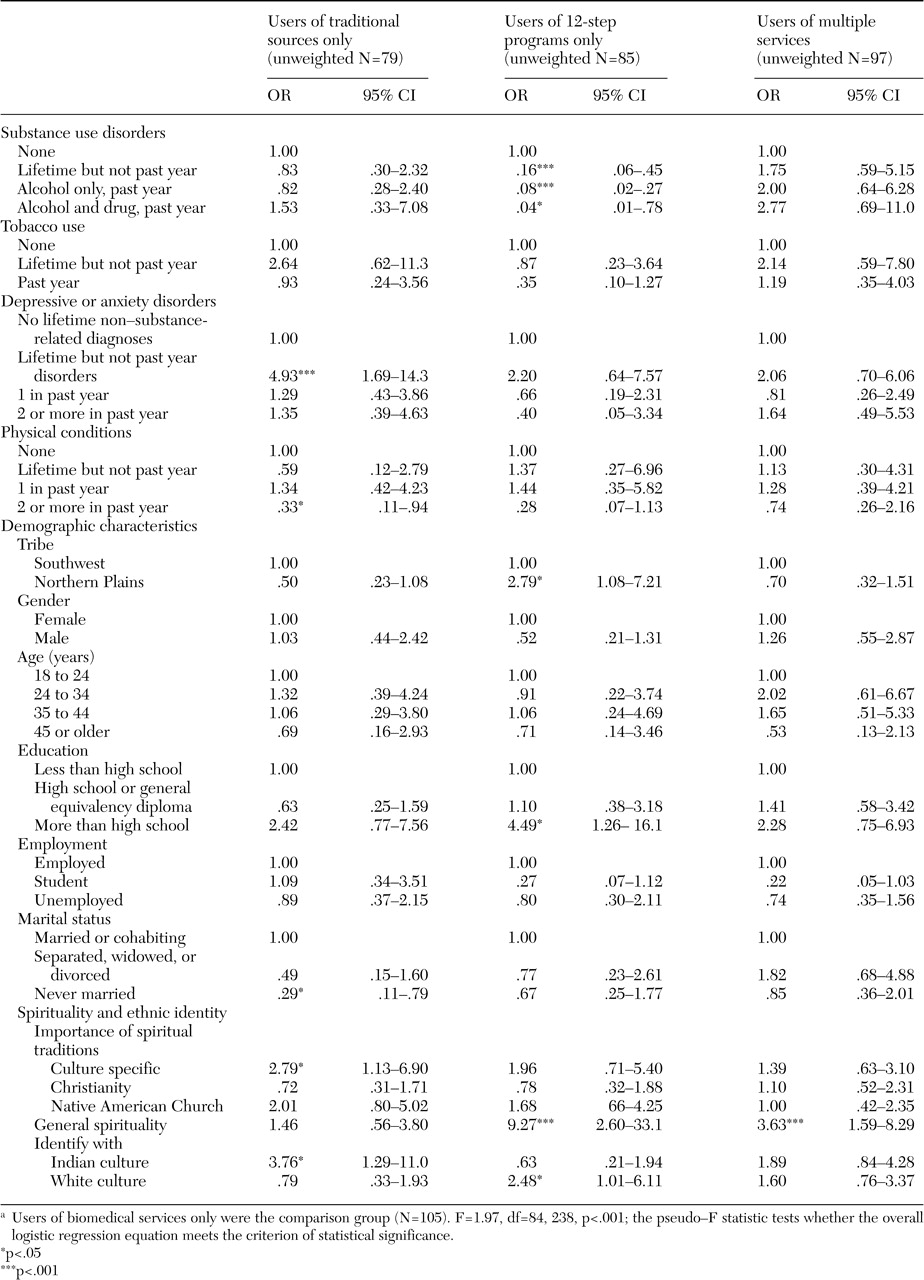
The American Indian Service Utilization, Psychiatric Epidemiology, Risk, and Protective Factors Project (AI-SUPERPFP), a population-based cross-sectional survey of two reservation populations, was designed to address such issues. This study assessed the extent of help seeking for alcohol and drug problems in the year before the interview, both overall and by modality (biomedical, traditional, and 12-step treatment modalities). We hypothesized that American Indians who use services would not only be more likely to have diagnoses of alcohol or drug use disorders but would also be more likely to have comorbid disorders and conditions. We further hypothesized that spirituality and ethnic identity would differentiate participants who sought help from traditional sources and 12-step programs from those who received help from biomedical sources only.
Acknowledgments
AI-SUPERPFP would not have been possible without the significant contributions of many people. The following interviewers, computer and data management staff, and administrative staff supplied energy and enthusiasm for an often difficult job: Anna E. Barón, Ph.D., Antonita Begay, Amelia T. Begay, Cathy A.E. Bell, Phyllis Brewer, Nelson Chee, Mary Cook, Helen J. Curley, Mary C. Davenport, Rhonda Wiegman Dick, Marvine D. Douville, Pearl Dull Knife, Geneva Emhoolah, Fay Flame, Roslyn Green, Billie K. Greene, Jack Herman, Tamara Holmes, Shelly Hubing, Cameron R. Joe, Louise F. Joe, Cheryl L. Martin, Jeff Miller, Robert H. Moran, Jr., Natalie K. Murphy, Melissa Nixon, Ralph L. Roanhorse, Margo Schwab, Ph.D., Jennifer Settlemire, Donna M. Shangreaux, Matilda J. Shorty, Selena S. S. Simmons, Wileen Smith, Tina Standing Soldier, Jennifer Truel, Lori Trullinger, Arnold Tsinajinnie, Jennifer M. Warren, Intriga Wounded Head, Theresa (Dawn) Wright, Jenny J. Yazzie, and Sheila A. Young. The authors also acknowledge the contributions of the Methods Advisory Group: Margarita Alegria, Ph.D., Evelyn J. Bromet, Ph.D., Dedra Buchwald, M.D., Peter Guarnaccia, Ph.D., Steven G. Heeringa, Ph.D., Ronald Kessler, Ph.D., R. Jay Turner, Ph.D., and William A. Vega, Ph.D. The authors thank the tribal members who so generously answered all the questions asked of them.
Furthermore, the AI-SUPERPFP team includes all the authors and Cecelia K. Big Crow, Dedra Buchwald, M.D., Buck Chambers, Michelle L. Christensen, Ph.D., Denise A. Dillard, Ph.D., Karen DuBray, Paula A. Espinoza, Ph.D., Candace M. Fleming, Ph.D., Ann Wilson Frederick, Joseph Gone, Ph.D., Diana Gurley, Ph.D., Lori L. Jervis, Ph.D., Shirlene M. Jim, Carol E. Kaufman, Ph.D., Ellen M. Keane, Suzell A. Klein, Denise Lee, Monica C. McNulty, Denise L. Middlebrook, Ph.D., Laurie A. Moore, Tilda D. Nez, Ilena M. Norton, M.D., Theresa O'Nell, Ph.D., Heather D. Orton, Carlette J. Randall, Angela Sam, James H. Shore, M.D., Sylvia G. Simpson, M.D., and Lorette L. Yazzie. This study was supported by grants R0-MH-48174 (Manson and Beals) and P01-MH-42473 (Manson) from the National Institutes of Health. Manuscript preparation was supported by grants R01-AA-13420 (Beals), R01-DA-14817 (Beals), R01-AA-13800 (Novins), and R21-AA-13053 (Spicer) from the National Institutes of Health.