Bipolar disorder is common—from 1 to 6 percent lifetime prevalence in the United States (
1,
2 )—and chronic. It is characterized by recurring manic and depressive symptoms and often psychosis (
3 ). The disorder is associated with high suicide rates (
4 ) and substantial social dysfunction (
3 ), ranking sixth as a cause of disability worldwide (
5 ). It may be the most expensive mental disorder for U.S. private behavioral health plans (
6 ) and employers (
7 ). Lifetime total costs per patient exceed $250,000 (
8 ), with up to 70 percent of direct treatment costs generated outside the mental health sector (
9 ).
As with other chronic medical illnesses, the cornerstone of managing bipolar disorder is evidence-based pharmacotherapy (
10,
11 ); however, undertreatment in ordinary clinical practice is an endemic problem (
12,
13,
14 ). The President's New Freedom Commission report noted that fragmented care, suboptimal clinical outcomes, substantial functional deficits, and high costs characterize all severe and persistent mental illnesses, including bipolar disorder (
15 ). The Institute of Medicine has recognized that these characteristics also describe other chronic medical illnesses (
16,
17 ).
Underscoring the problems associated with undertreatment, the low medication response rates in recent real-world clinical trials for depression (
18,
19 ), schizophrenia (
20 ), and bipolar disorder (
21 ) indicate that more comprehensive approaches for such illnesses are warranted. The development of structured psychotherapies for bipolar disorder, including cognitive-behavioral therapy (
22,
23,
24,
25 ), family therapy (
26 ), and psychoeducation (
27,
28 ), is promising, although effectiveness appears limited for persons with greater impairment (
25 ).
Moreover, promising treatments for chronic conditions do not easily move from initial clinical trials to general practice for mental illnesses (
29,
30,
31 ) or other medical illnesses (
16,
32,
33 ). The dearth of evidence-based interventions applicable for the public sector is particularly notable; less than 3 percent of mental health clinical trials have been conducted in such settings (
34 ). How, then, can outcome be improved for individuals with bipolar disorder under real-world clinical conditions, particularly in the public sector?
In this article we summarize the conceptual background and development of an intervention model for the treatment of bipolar disorder, describe the design of a three-year, 11-site randomized effectiveness trial, and report data describing its successful implementation.
Intervention development
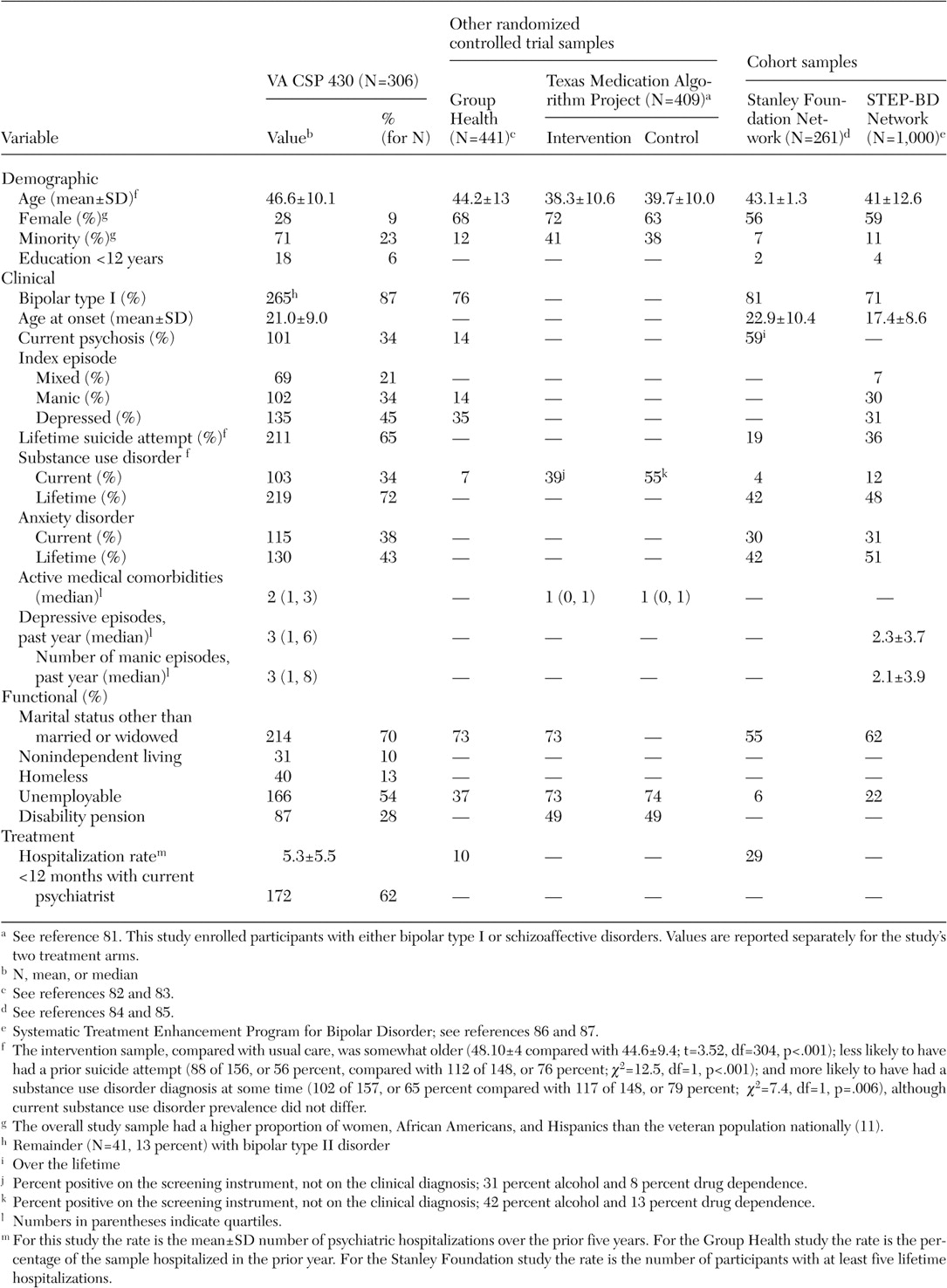
In 1992 we evaluated treatment needs for individuals with bipolar disorder at our Department of Veterans Affairs medical center (VAMC). Comorbidity was common, and the population tended to be poor, have chronic disabilities, and be without families or social support networks. Without funding to develop a mobile treatment team or wraparound services such as a program for assertive community treatment (
35,
36,
37 ), we were limited to reorganizing existing outpatient clinic-based services.
Given the available literature on interventions for chronic illness, we recognized that our intervention would need to address three factors (
38 ). First, the intervention should accommodate severely ill patients with comorbidities, who are common in clinical practice but typically excluded from clinical trials (
39 ). Second, the intervention should minimize the provider-based variability typical of medical-surgical (
40,
41,
42 ) and mental health (
43 ) care. Evidence-based clinical practice guidelines could reduce such provider-based variability, but they have not been well implemented under naturalistic conditions (
44 ). Third, the intervention should minimize the substantial system-related barriers characteristic of chronic care (
32,
33,
45,
46 ) to allow providers and patients to come together for timely, proactive illness management.
After a literature review, consultation with experts in bipolar disorder, and discussion with patients, we identified two main conceptual models (
13 ). First, in the 1970s lithium clinics supported the transition from predominantly or exclusively psychotherapeutic treatment to a medical model of treatment for bipolar disorder (
47,
48,
49,
50,
51 ). These clinics were organized around medication delivery, typically by a team consisting of a psychiatrist and support staff, with an emphasis on standardized care. Patient education was critical; provision of information was often supplemented by support groups to facilitate destigmatization, peer-based learning, and mutual support. Our specific orientation toward patient education derived from nursing practice, which has long emphasized patient education and collaborative decision making (
52,
53 ). The value of a collaborative patient-centered approach was underscored by the feedback we received from patients and has been documented recently in formal studies (
54,
55 ).
Second, we became aware of the chronic care models being developed for chronic medical illnesses by Wagner, Von Korff, and others (
32,
33,
56,
57 ). These models recognize that chronic illnesses are inadequately treated, despite the availability of efficacious medications. They emphasize anticipatory, patient-centered care by addressing four aspects of clinical care. Patient self-management skills are enhanced via education and collaborative goal setting. Provider decision making is supported by expert guidance, which may range from provision of practice guidelines to facilitated specialist consultation. Information flow is facilitated through various methods, ranging from development of complex electronic infrastructure to use of support staff to ensure that the clinician is provided with adequate patient data during the encounter. Work role redesign for both physician and support staff is typically required to achieve these changes.
The central focus of chronic care models, based on principles of social learning and self-regulation theories (
56 ), is to reorganize medical care to support an effective partnership between clinicians and patients to improve outcomes relevant to patients (
58 ). A recent review indicates that such interventions improved process or outcome measures in 32 of 39 clinical trials. All five trials that used all four components showed benefit. Notably, 19 of 20 interventions with a patient self-management component were effective (
30 ).
We therefore defined the collaborative chronic care model as "an organization of care that emphasizes the patient's development of illness management skills and supports provider capability and availability in order to engage patients in timely, joint decision making about their illness" (
13 ). The model articulates "chronic" care not in any pessimistic sense but rather to emphasize ongoing, anticipatory (rather than reactive, crisis-oriented) management (
32,
33,
56,
57 ). In fact, the strong emphasis on patient-centered collaboration anticipates current wellness and recovery orientations (
55 ).
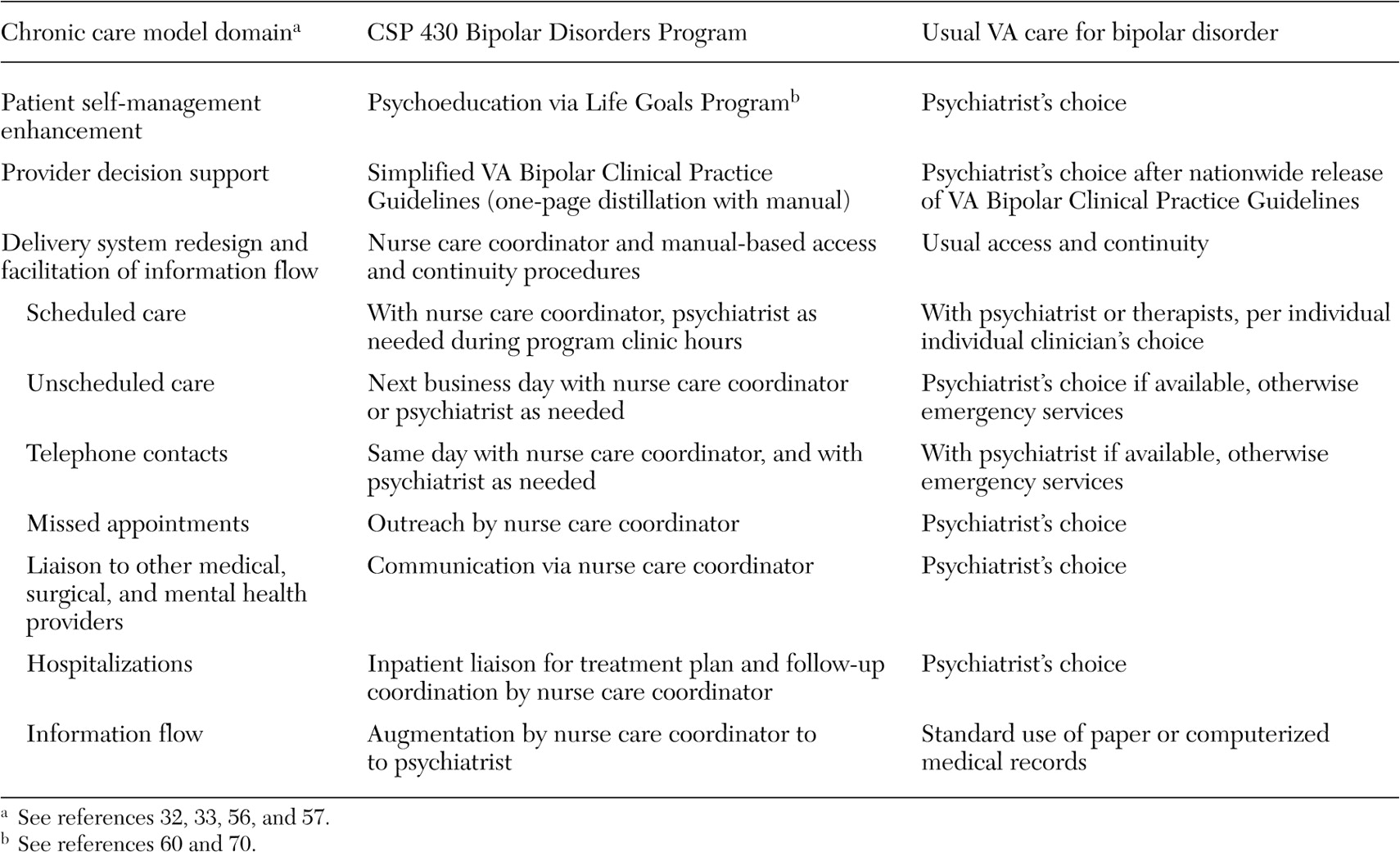
On the basis of these considerations, we organized a team-based intervention (
57 ) that consisted of patient psychoeducation to improve self-management skills, simplified clinical practice guidelines, and use of a nurse care coordinator working in collaboration with a supervising psychiatrist to enhance continuity of care and information flow as described in detail below. We conducted a population-based, quasi-experimental study (
59 ) with 103 veterans with bipolar disorder at our VAMC, excluding only those with dementia. Bipolar care was transferred to the intervention; no other existing care was changed, and specialty care referrals were made as clinically indicated. Compared with baseline, bipolar-specific pharmacotherapy increased without increased side effects, and patient satisfaction increased dramatically; the intervention retained more than 90 percent of participants at one year. Among those hospitalized in the prior year, psychiatric hospital days declined to 57 percent, and direct treatment costs were reduced by 65 percent.
On the basis of these data, in 1996 the VA Cooperative Studies Program (CSP) funded a three-year, multisite randomized controlled trial to test this model (CSP 430). Our hypotheses (
38 ) were that, compared with usual care, the intervention would improve clinical outcome, with gains maximal over years 2 and 3; reduce total direct (mental health plus medical-surgical) treatment costs from the VA's economic perspective over three years; and improve functional outcome by the third year. The lag time to response would be consistent with preliminary data (
59,
60 ) and characteristic of social learning theory (
56 ).
Acknowledgments
This study was funded by Department of Veterans Affairs Cooperative Studies Program 430. The authors especially thank Nancy M. Shea, R.N., M.S., Tracy Wyrostek, Christina Moniz, Tara Burke, Erinn Dawson, M.A., Eileen Richardson, and G. F. Kimpton for their assistance. Additional acknowledgments are available in the online supplement to this article at ps.psychiatryonline.org. Some of the findings in this article were presented at the annual meeting of the American College of Neuropsychopharmacology, held in San Juan, Puerto Rico, December 12-16, 2004, and at the 18th Mental Health Services Research Conference, held by the National Institute of Mental Health in Washington, D.C., July 18-19, 2005.