As numerous case studies since the mid-1990s have documented, managed behavioral health care organizations (MBHOs) are clearly effective in reducing the costs of specialty mental health and substance abuse treatment (
1,
2,
3,
4,
5,
6,
7,
8 ). Early studies also showed that these MBHOs achieved cost savings of as much as 30% to 40%, primarily through a cost-control strategy of substituting less expensive outpatient services for inpatient care (
9,
10,
11 ).
However, these studies focused only on what happened within the carved-out specialty mental health sector for which the MBHOs were directly responsible and for which they had incentives for cost control (
12,
13 ). These early studies did not or were not able to include pharmaceutical claims for psychiatric disorders and mental health services provided by general practitioners. MBHOs are usually not financially responsible for psychotropic medication and mental health care provided by primary care physicians, so they may seek to shift costs into these areas in order to reach their contractual cost-savings goals in the specialty mental health sector.
This type of cost shifting, for which there is empirical support (
14,
15 ), within the complex mental health care financing and delivery system is a long-standing concern. The establishment of MBHOs in the early 1990s led to new opportunities to shift service use and costs between service settings or payers. Insurers and employers contract with MBHOs precisely because they expect them to reduce or restrain specialty mental health treatment costs. The MBHOs may be at direct financial risk for specialty mental health and substance abuse treatment services provided to the insurer or employer through a capitation formula or through financial bonuses and penalties. Even when a MBHO is not at direct financial risk for performance, game-theoretic models (
16 ) suggest that the MBHO will be concerned about the renewal of its contracts as well as its reputation to reduce behavioral health services costs. This, in turn, creates incentives to shift costs so that the MBHO is seen as able to keep specialty mental health costs down.
We follow previous studies of cost shifting in managed behavioral health care settings by conceptualizing cost shifting as an incentive for a particular organization, provider, or payer to substitute mental health treatments in settings where such treatments are free goods to the financially responsible entity (
17,
18,
19 ). In this case, the costs of prescription medication and of treatment provided by primary care physicians are effectively zero for the MBHO, whereas the costs of specialty mental health services are not. MBHOs may shift costs directly by substituting pharmacotherapies for specialty outpatient treatment visits and by influencing the behavior of the providers in their network. If this direct cost shifting is occurring, we would expect to find an increase in the use of psychotropic medications and a decrease in specialty treatment visits associated with the introduction of an MBHO.
MBHOs may also shift costs indirectly by restricting access to specialty providers. This would encourage patients to seek treatment from primary care physicians, who are likely to prescribe pharmacotherapies. In this case, we would also expect to observe an increase in the use of psychotropic medications without specialty treatment, above and beyond strong upward trends in prescription of these medications in primary care settings.
To empirically test whether cost shifting occurs, either directly or indirectly, we examined the experience of one insurer that introduced an MBHO to its entire line of business after one of the insurer's largest groups implemented parity in its mental health benefit in the early to mid 1990s. We build on previous analyses of this typical MBHO (
8,
20,
21 ). In particular, one of these analyses found that introduction of the MBHO was associated with a decrease in the rate of growth of psychotropic drug utilization and costs (
20 ), which is inconsistent with the cost-shifting hypothesis. In the study presented here, we undertook an additional empirical test of the cost-shifting hypothesis by investigating whether introduction of the MBHO was associated with an increase in the use of pharmacotherapies without ongoing specialty treatment. The MBHO was not at direct financial risk for the costs of specialty mental health treatment, so we were formally testing our hypothesis that reputation and contract-renewal incentives to control behavioral health care costs led to cost-shifting behavior and changes in treatment patterns (
22 ). It is important to note that this test cannot distinguish between the direct and indirect effects of the MBHO.
This test provides additional evidence for employers, insurers, and other decision makers who remain concerned about MBHO cost-shifting behavior (
23,
24 ). We also focused on this test because concerns continue to be raised about potential differences in the quality of care given by different providers. In particular, some studies have reported that the addition of specialty care improves outcomes for depression (
25,
26 ).
We used both simple t tests and multivariate panel data methods in conducting the empirical test of cost-shifting behavior. The panel data methods allowed us to better control for underlying secular trends (
27,
28 ), for example, primary care physicians' becoming more comfortable prescribing psychotropic medications without referring patients to specialists (
29 ). In addition to the large employer group, we included a collection of medium and small groups that did not implement mental health insurance parity. Little is known about the experience of these smaller groups because previous case studies have focused almost exclusively on large employers. The MBHO faces the same incentives to shift costs as these medium and small groups. However, changes in the medium and small groups were not confounded by parity effects, which provided a cleaner test of the cost-shifting hypothesis.
Background
The MBHO
The MBHO functions included preauthorization of inpatient and outpatient services, concurrent utilization review, and a network of specialty mental health providers (with higher cost sharing for out-of-network services). Before the implementation of the MBHO, mental health treatment was delivered under the traditional fee-for-service products of the insurer, with no prior authorization requirements, utilization review, or provider networks. Importantly, neither the specialty providers nor the MBHO were at direct financial risk for mental health services. However, we hypothesized that the MBHO did face incentives to reduce costs related to reputation and contracting renewal in competitive markets. Typical of carve-out arrangements, the MBHO was not responsible for prescription medication costs, which were administered separately by a third-party pharmacy benefit manager. The insurer also began offering a point-of-service plan with reduced consumer cost sharing for in-network medical services at the same time that it carved out mental health and substance abuse services to the MBHO. The point-of-service plan managed costs through primary care gatekeeping for all specialist referrals, except for those handled by the MBHO.
The large employer
The large employer group comprised mostly white-collar workers employed at multiple locations in a single state (confidentiality agreements limit the details that can be disclosed). Under legislative mandate in the 1990s, this particular group was required to begin providing parity coverage (the same health insurance coverage as for general medical services) for severe mental disorders, which were defined as schizophrenia, schizoaffective disorder, bipolar disorder, major depressive disorder, paranoid disorder, and other psychotic disorders). Introduction of parity coverage resulted in significantly reduced consumer cost sharing, especially for outpatient services. The large employer also reduced consumer cost sharing (but not visit limits) for nonsevere disorders in the point-of-service plan. Prescription medication coverage, however, did not change substantially.
The medium and small employers
We selected a group of medium and small employers from industries with workers who were similar to those of the large employer. However, these groups differed from the large group along a number of important dimensions, including less generous coverage and lower baseline utilization, even after enrollee and coverage differences were controlled for. These medium and small employers also were not subject to a state parity mandate during this time period and did not substantially change their mental health coverage. Because of these differences, the medium and small employers could not serve as a control or comparison group for our large group.
Methods
Data
Data were from enrollment and claims files provided by the insurer for the four-year study period (September 1, 1991, to August 31, 1995)—one year before and three years after implementation of the MBHO on September 1, 1992. The Area Resource File (ARF) provided supplemental data on county-level demographic and resource capacity. For the large group, initial sample sizes were as follows: 167,707 for the first year, 202,786 for the second year, 227,107 for the third year, and 226,852 for the fourth year. For the medium-small group, the samples were 29,848 for the first year, 34,972 for the second, 41,896 for the third, and 44,775 for the fourth.
We followed standard practice and restricted the analyses to the population continuously enrolled during the four-year study period to minimize the potential for adverse selection (
1,
10,
30 ), which resulted in sample sizes of 107,596 and 14,064 for the large and medium-small groups, respectively. The results reported here are not sensitive to this restriction, which we tested by reestimating our models to include all persons who were continuously enrolled for 270 days (three quarters)—the minimum time frame necessary to conduct the analyses. We also excluded the remaining persons who were 55 years old and older in the first year of the study period to minimize the problem of distinguishing employees from retirees and the confounding effects of Medicare and other insurance coverage. Most persons (86%) aged 55 and older were not continuously enrolled over the four-year period.
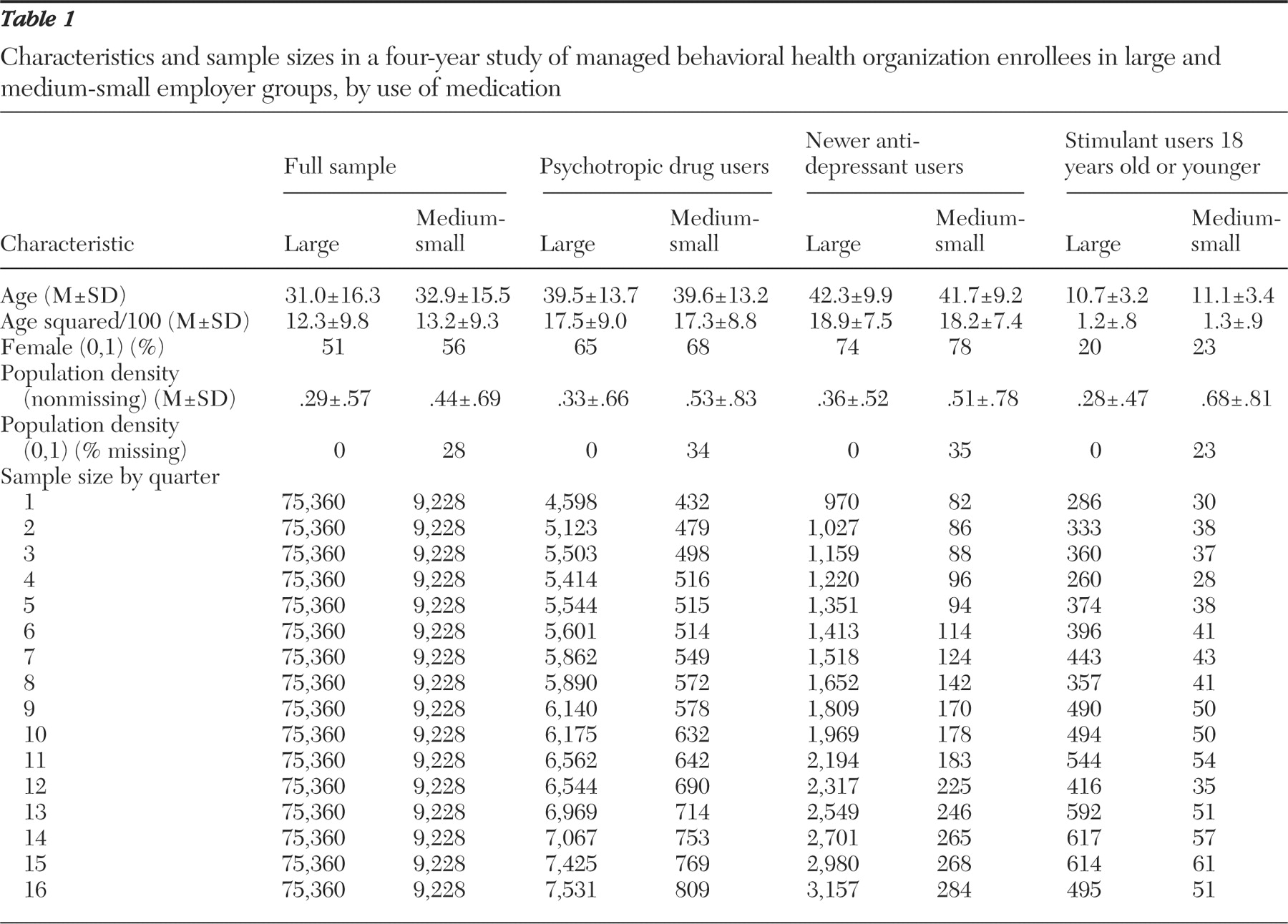
Our final study population sizes were 75,360 continuously enrolled members under the age of 55 for the large group and 9,228 members for the medium-small group (after an additional 3,637 individuals were dropped because we could not determine whether their group provided prescription drug coverage). To facilitate the analyses, we divided the four years of data into 16 quarterly observations for each person (quarters 1 through 4 in the period before MBHO implementation and quarters 5 through 16 in the postimplementation period). Thus the unit of observation for the main analyses was person-quarter.
We used National Drug Codes (NDC) to identify psychotropic medications from the prescription claims data available from the third-party pharmacy benefit management. Data from the U.S. Food and Drug Administration's NDC database (
31,
32 ) were supplemented with NDC data from the Red Book databases (
33,
34,
35 ), resulting in an approximately 99% match rate. We included the following classes of medications: benzodiazepines and other antianxiety medications; barbiturates; sedatives and hypnotics; first- and second-generation antipsychotics; antimanics; substance abuse medications; monoamine oxidase inhibitors; tricyclic antidepressants; and selective serotonin reuptake inhibitors (SSRIs) and other antidepressants introduced since the tricyclic antidepressants (bupropion, citalopram, fluoxetine, fluvoxamine, maportriline, mirtazapine, nefazadone, paroxetine, sertraline, trazadone, venlafaxine), which we refer to here as "newer antidepressants"; and stimulants (amphetamine, dextroamphetamine, methamphetamine, methylphenidate, and pemoline). A full list is available from the authors.
Testing the cost-shifting hypothesis
We implemented our test of the hypothesis that cost shifting would lead to an increase in the use of psychotropic medication without a concurrent increase in specialty treatment by constructing a binary indicator (Y it ) of whether a person using psychotropic medications during a particular quarter also used specialty treatment in either the same quarter, the quarter before, or the quarter afterward. This approach provides a minimum of a 180-day window during which a person using psychotropic medications may have also used specialty mental health treatment, which is a conservative measure of ongoing specialty treatment. We excluded the first quarter (quarter 1) because we did not have information about specialty use in the quarter before, and we also excluded the last quarter (quarter 16) because we did not have information about specialty use in the quarter afterward. We did not attempt to construct treatment episodes, principally because primary care providers frequently do not code mental health diagnoses when billing.
We first tested whether the proportion of patients using any mental health-related medication without ongoing specialty mental health treatment changed from the preimplementaton period (quarters 2 through 4) to the postimplementation period (quarters 5 through 15). However, because many psychotropic drugs have other uses, we also examined the use of two widely prescribed classes of drugs that are primarily used for psychiatric reasons—SSRIs and other newer antidepressants and stimulants. Nationally representative prescription drug data from the 1996-2003 Medical Expenditure Panel Survey (MEPS) suggest that 92% of SSRI and other new antidepressant use and 94% of stimulant use is for mental health-related reasons, whereas only 49% of tricyclic antidepressant use and 71% of benzodiazepine use is for mental health-related reasons (authors' calculations from MEPS public use files).
To implement these tests, we created a subset from the continuously enrolled sample of person-quarters with any mental health-related medication use, any newer antidepressant use, and any stimulant use. Thus the sample included observations from persons who used these medications in every quarter and persons who used these medications in only some of the quarters—that is, the panel is unbalanced. (
Table 1 provides the person-quarter sample sizes for each quarter.) We report results of both simple t test comparisons of means over time and multivariate panel data tests described below.
Multivariate panel data specification
We used the following probit specification to test whether the dependent variable, probability of using psychotropic medications alone (Y it ), changed from the pre- to the postimplementation period:
Y it =Φ(a 0 +a 1 POST it +a 2 QTR it +δ' Z it ), where I is the person and t is 2 through 15 quarters.
First, POST is a binary indicator for whether the observation falls in the postimplementation period (quarters 5 through 15). This provides the direct test of the cost-shifting hypothesis. The variable QTR (2 through 15) was included to control for any underlying linear trend in the use of medications alone—for example, as primary care physicians became more comfortable prescribing medications themselves. We tested an alternative specification that allowed for different pre- and postimplementation trends. However, the estimated trends were nearly identical and not statistically different from one another, suggesting an underlying trend common to both periods. We also tested for nonlinear trends but failed to reject the null hypothesis of a linear trend.
We included as covariates age, age squared, and sex from the limited information available in the membership and claims files in the vector of covariates
Z it . We also included a measure of population density (persons per 1,000 square miles) of the county in which that plan subscriber resided, because the degree of urbanization is likely correlated with use of mental health treatment (
36 ). We tested alternative specifications with a broader set of measures, including whether the person was an employee, spouse, or dependent; per capita number of hospitals beds, psychiatrists, other physicians, and psychologists or social workers; and comorbid health conditions. However, the main results were not sensitive, and we report the more parsimonious specification here.
We estimated the probit model using the generalized estimating equations (GEE) approach (
37,
38 ) to account for the within-person correlation (up to 14 quarterly observations for each person). The theoretically correct within-person correlation structure is unclear, but the GEE estimator is consistent even when this correlation structure is misspecified. For simplicity, we assumed that within-person correlation was constant across time (or exchangeable error structure). We note that the GEE estimates may be biased when estimated with unbalanced panels, but we had no prior expectations about the direction of any potential biases from persons who did not fill psychotropic medications in every quarter. The models were separately estimated for the large and medium-small groups. Standard errors of marginal effects were estimated by nonparametric bootstrap with 1,000 replications, and they accounted for the within-person correlation across observations.
Results
Univariate and bivariate descriptive results
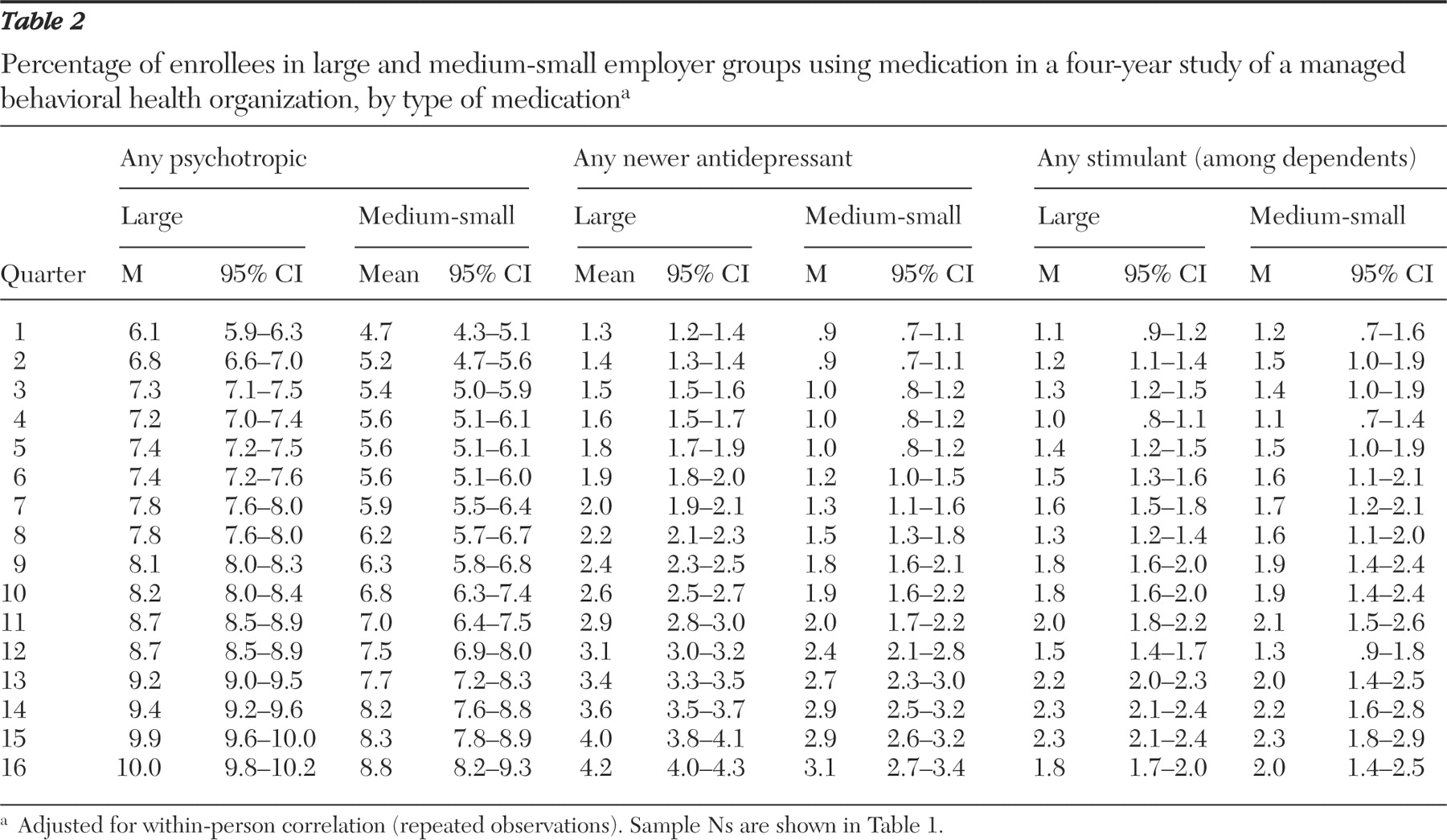
Table 2 shows the rapid increases in psychotropic medication use. From the first to last quarter among enrollees of the large employer group, the use of any psychotropic medication rose 64% in relative terms, or 3.9 percentage points in absolute terms (t=28.03, df=75,359, p<.001). For the medium-small employer group, the respective increase was 87% (t=10.89, df=9,227, p<.001). Much of the overall increase in the use of psychotropic medications was due to increased use of SSRIs and other newer antidepressants, which tripled in both the large group (t=37.04, df=75,359, p<.001) and the medium-small group (t=11.23, df=9,227, p< .001). Stimulant use among dependents also increased substantially—in the large employer group by 84% (t=11.38, df=75,359, p<.001) and in the medium-small employer group by 60% (t=2.90, df=9,227, p=.004). The declines in stimulant use during the last quarter of each fiscal year (that is, quarters 4, 8, 12, and 16) correspond to the summer months, when some children may be taken off stimulants.
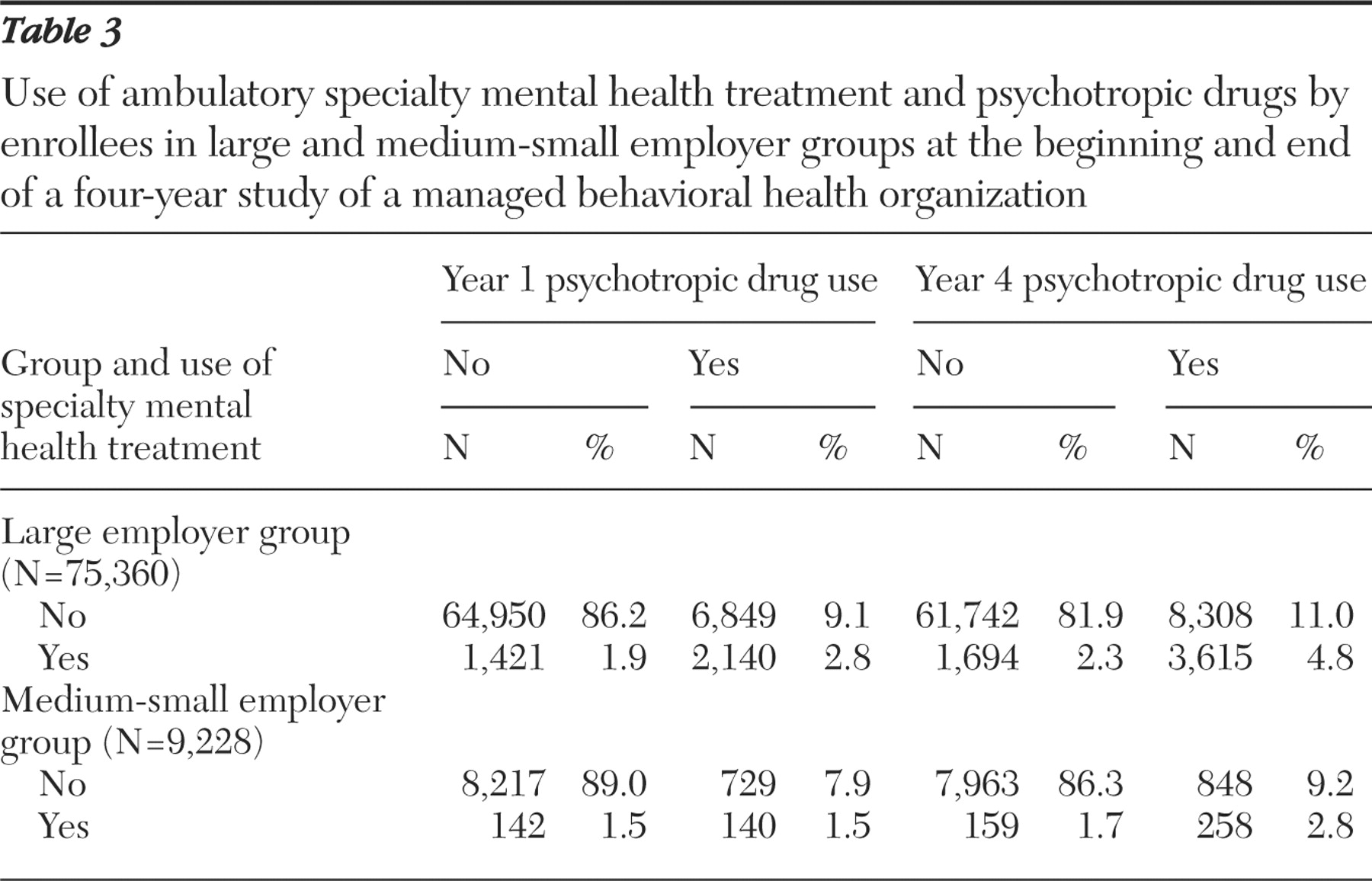
Table 3 illustrates whether there was a shift between specialty care and prescription medication use by presenting 2×2 tables of any psychotropic medication use crossed with any ambulatory specialty mental health use during year 1 and year 4. In the large group, a decrease was seen, from 86.2% with neither specialty nor psychotropic medication use in year 1 to 81.9%; more people used psychotropic medications either alone (11.0% in year 4 compared with 9.1% in year 1) or in combination with specialty care (4.8% in year 4 compared with 2.8% in year 1). A similar pattern of changes occurred for the medium-small group.
Table 3 also shows a clear relative shift away, as measured by percentage of treatment users, from use of specialty care alone toward psychotropic drug use alone or specialty care in combination with psychotropic drug use.
Jointly modeling the changes in the 2×2 tables from year 1 to year 4 in the presence of strong underlying trends presents numerous technical challenges beyond the scope of this article. We focus instead on the simpler strategy of looking at people with psychotropic drug use and examining whether any change occurred in the use of psychotropic medications without ongoing specialty care after introduction of the MBHO. Again, this focus is important because of concerns about potential differences in the quality of care given by providers (
15,
16 ).
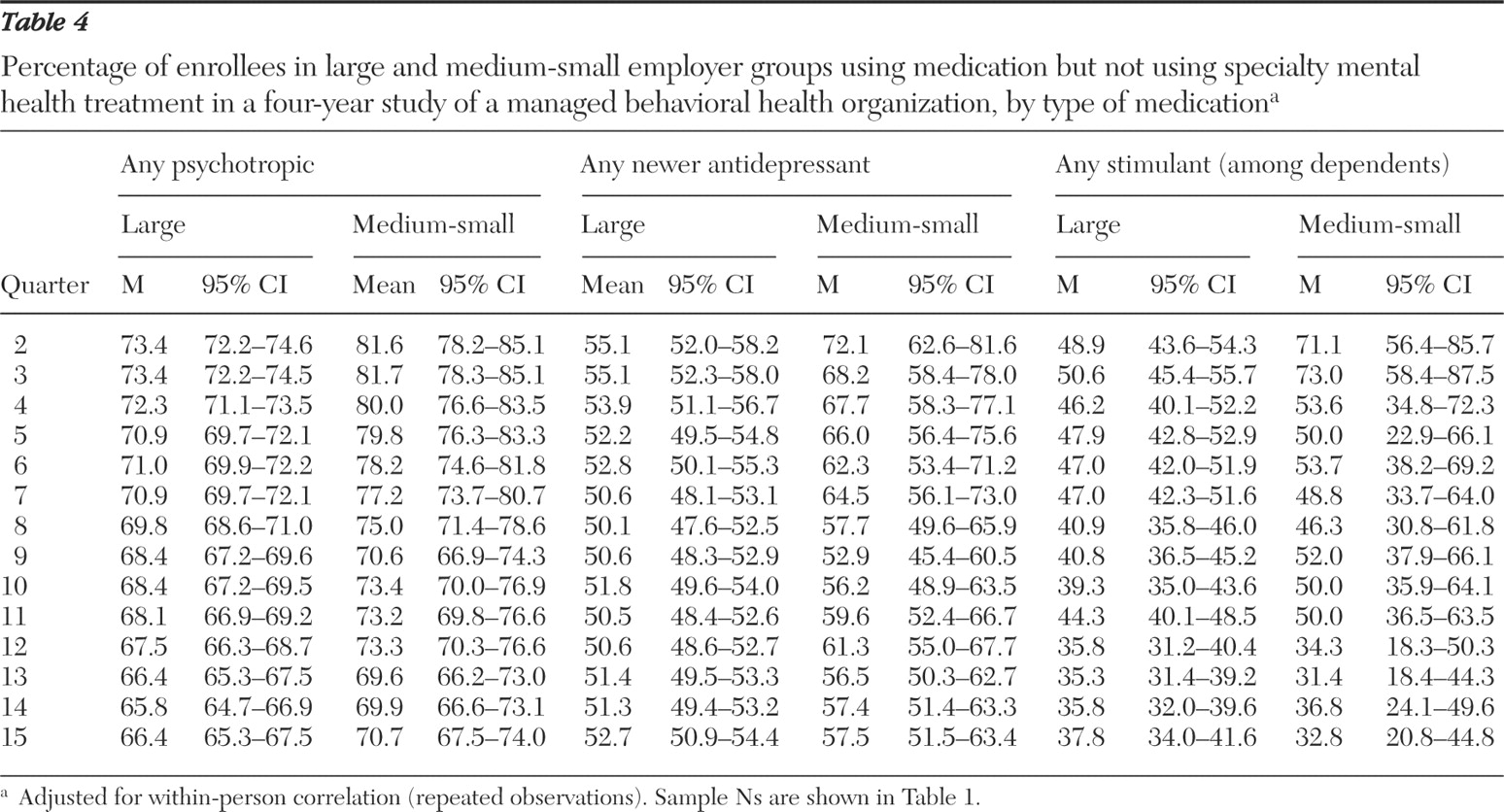
Table 4 shows results of our main test. Among persons using psychotropic medications, the percentage using them alone without concurrent specialty mental health care (that is, without specialty care in the current, previous, or following quarter) tended to decrease over time. The use of newer antidepressants alone remained relatively unchanged in the large group from quarter 2 (55.1%) to quarter 15 (52.7%) but fell substantially from 72.1 to 57.5% in the medium-small group (t=2.72, df=592, p=.007). The use of stimulants alone fell substantially in the large group (t=3.50, df=7,070, p<.001) and by an even greater amount in the medium-small group (t=4.36, df=705, p=.004). Interestingly, although the use of psychotropic medications alone was initially much higher in the medium-small group, the larger drop in this rate in the medium-small group led to convergence with the large group.
Multivariate panel data
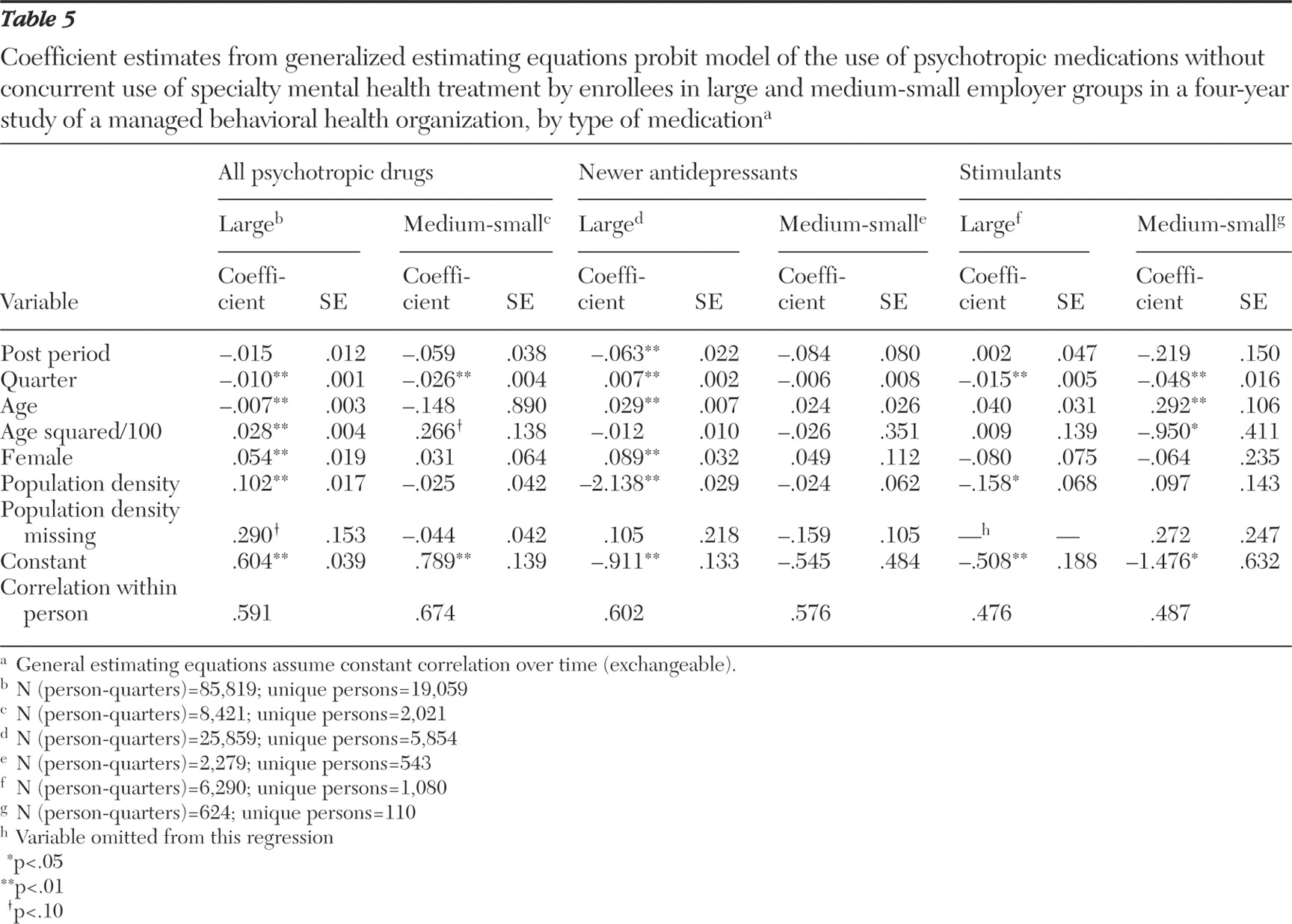
In
Table 5 we present the full results of our more formal test of whether a change occurred in the use of prescription medications alone after the introduction of the MBHO. For ease of interpretation, we have converted the probit coefficient estimates into marginal effects in our discussion of the results. For the POST variable (postimplementation), the marginal effect represents the pre- to postimplementation change in the percentage using medications alone—that is, without concurrent specialty mental health treatment. The marginal effect for the QTR variable (quarter) is the underlying quarterly trend in the percentage using medication alone (QTR), common to both the pre- and postimplementation periods. Again, statistical tests suggest that this trend did not differ between the pre- and postimplementation periods. In other words, there was no abrupt change in trend associated with the MBHO.
Data for all psychotropic medications in
Table 5 indicate that decreases in the use of medications alone after the introduction of the MBHO, as represented by the POST variable, were not statistically significant for either the large or medium-small employer groups. However, the underlying downward quarterly trends in the use of psychotropic drugs were statistically significant for both groups. For the large employer group, use of psychotropic drugs alone was dropping, on average, .3 percentage points per quarter (z=8.17) or 1.2 percentage points per year. The downward trend was even stronger in the medium-small group, .70 percentage points per quarter (z=7.08).
Use of the newer antidepressants followed a somewhat different pattern. For the large employer group, there was a statistically significant decline of 2.4 percentage points (z=2.92) in the use of newer antidepressants by themselves after the introduction of the MBHO. In contrast to use of all psychotropic drugs, there was a statistically significant underlying upward trend in the use of newer antidepressants alone of .3 percentage points per quarter (z=3.27) in the large employer group. No statistically significant changes were seen in the use of antidepressants alone in the medium-small employer group.
Finally, no statistically significant change was seen in the use of stimulants alone associated with the introduction of the MBHO in either the large (z=.05) or medium-small groups (z=1.47). However, the statistically significant negative quarterly marginal effects for both the large group (.56 percentage points per quarter, z=3.01) and the medium-small group (1.79 percentage points per quarter, z=3.04) point to a strong downward trend in the use of stimulants alone.
Discussion
We found no evidence for our hypothesis that introduction of the MBHO increased the use of psychotropic medications without concurrent use of specialty mental health treatment. In fact, we found some evidence of a decrease in the use of psychotropic medications alone. The four-year descriptive trends indicated slight declines in the use of psychotropic drugs without concurrent specialty mental health treatment in the large employer group and substantial declines in the medium-small employer group. Controlling for underlying trends in the panel data regressions, we also found that introduction of the MBHO was associated with a statistically significant decrease in the use of the newer antidepressants alone in the large employer group. Although in other cases the associations were not statistically significant, the marginal effects almost always pointed to decreased use of psychotropic drugs alone.
Our alternative test similarly found no shift associated with introduction of the MBHO from specialty care alone toward specialty care in combination with medication use. At the same time, it is important to note that the number of people receiving psychotropic medications grew substantially over the study period and that these medications were often prescribed in primary care settings. This growth appears to be the result of strong underlying secular trends and not the introduction of the MBHO.
If the MBHO had limited the use of specialty mental health care services, it might result in lower quality of care and poorer outcomes for people with mental illness. Previous work has shown an improvement in mental health when specialty mental health providers are involved in care (
25,
39,
40 ). In addition, because pharmacologic agents are not always the best option for some people, it is important to have access to other forms of therapy (such as psychotherapy) that are offered only by mental health specialists. The continuing growth in the provision of pharmacotherapies in primary care settings only heightens concerns about coordination with and access to specialists. Further research is needed to determine the impact of MBHOs on the overall quality of care received by people with mental illnesses.
The lack of apparent cost shifting by the MBHO is consistent with findings of earlier studies that analyzed the impact of this MBHO on costs and access. Evidence was found that introduction of this MBHO was associated with reductions in the rate of growth of ambulatory specialty mental health treatment (
21 ). By itself, this might indirectly imply that the MBHO engaged in cost shifting either to the primary care sector or to the pharmacy benefit—the MBHO was not financially responsible for either. However, a previous study found that introduction of the MBHO was also associated with a decrease in the rate of growth of psychotropic drug use and spending (
20 ). Moreover, neither the average number nor the distribution of specialty mental health visits changed after the introduction of the MBHO (
8 ), which further suggests that the MBHO did not shift treatment to pharmacotherapies. Taken together these results do not show any evidence that the MBHO shifted costs directly to the pharmacy benefit or indirectly to primary care settings. We note that previous studies also found mixed evidence of cost shifting (
18,
19 ).
Several explanations may be consistent with the apparent lack of evidence for cost-shifting behavior. Because the MBHO was not at direct financial risk for specialty treatment services, the incentives to shift costs to the pharmacy benefit may have been somewhat weaker than if the MBHO were capitated. However, the MBHO was expected to reduce specialty treatment costs, and other incentives, including contract renewal, were tied to meeting these targets. The MBHO lowered specialty treatment costs by substantially reducing inpatient spending, even as outpatient specialty treatment was increasing (
8 ). The savings achieved by reducing inpatient spending may have allowed the MBHO to meet performance targets without aggressively shifting costs. Over time, however, the savings that can be achieved through reduction in inpatient treatment might be exhausted and the increasing demand for outpatient specialty treatment would then be expected to create stronger incentives to shift costs if further reductions in costs are needed.
Finally, although there is evidence that the MBHO decreased the rate of growth of both outpatient specialty treatment visits (
21 ) and prescription drug use (
20 ), it may have done so by simply restricting access to specialty providers rather than influencing the mix of services delivered by the specialty providers toward pharmacotherapies. If the MBHO had restricted access to specialty mental health treatment, we would have observed a substantial increase above general trends in the use of prescription drugs without specialty treatment only if primary care providers could sufficiently meet the increased demand in primary care settings. Capacity and other supply constraints may have prevented primary care providers from meeting increased demand. In other words, instead of shifting costs to either the primary care sector or pharmacy benefits (that is, increased use of psychotropic medications), the MBHO may have avoided an increase in costs by reducing access to any mental health treatment.
A number of caveats apply. As with most studies of this topic, our case study involved a single insurer and MBHO and a limited number of employer groups. This necessarily limits the ability to generalize to other populations. A lack of an adequate control or comparison group also limits our analyses to pre- and postimplementation differences in levels and trends. We cannot, for example, differentiate a change in the underlying secular trend from the impact of the MBHO. Use of a control group would better capture changes in secular trends, allowing for stronger inferences to be drawn. Our sample for the medium-small employer group is small, especially for the stimulant analyses, limiting our power to detect the effects of the MBHO. Finally, our data are more than ten years old, but we expect that the same incentives to shift costs still exist.
Conclusions
The rapid growth of carve-outs to MBHOs in the past two decades heightened long-standing concerns about cost shifting in mental health treatment. In this particular case study of the implementation of a single MBHO, we found no evidence of cost-shifting behavior toward primary care settings. However, carve-outs to MBHOs are now ubiquitous, and powerful market incentives remain for MBHOs to shift costs toward alternative treatment modalities and treatment settings.
Acknowledgments and disclosures
The authors are grateful to Darrel Regier, M.D., M.P.H., who established and developed the partnership with the health care plans and the large employer group to pursue this research, and to the knowledgeable staff of the health care plans for their guidance in preparing the data for analysis. Donald Rae, M.A., provided programming support. The authors also thank Steve Hill, Ph.D., John Fleishman, Ph.D., Chad Meyerhoefer, Ph.D., and Jessica Banthin, Ph.D., for their insightful comments and suggestions.The views expressed in this article are those of the authors, and no official endorsement by the Agency for Healthcare Research and Quality, the National Institute of Mental Health, or the Department of Health and Human Services is intended or should be inferred.
The authors report no competing interests