Univariate analyses
Tables 1,
2,
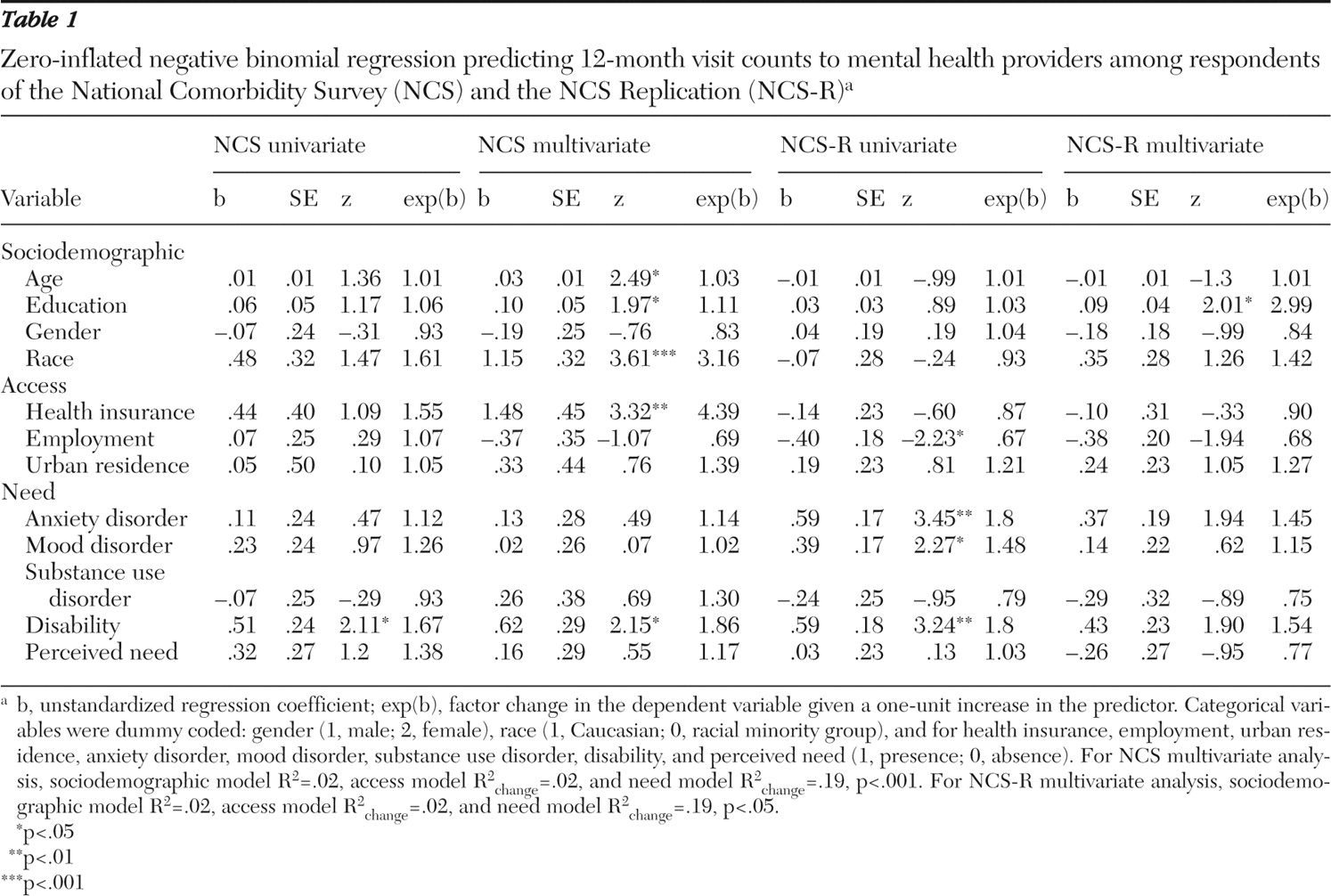
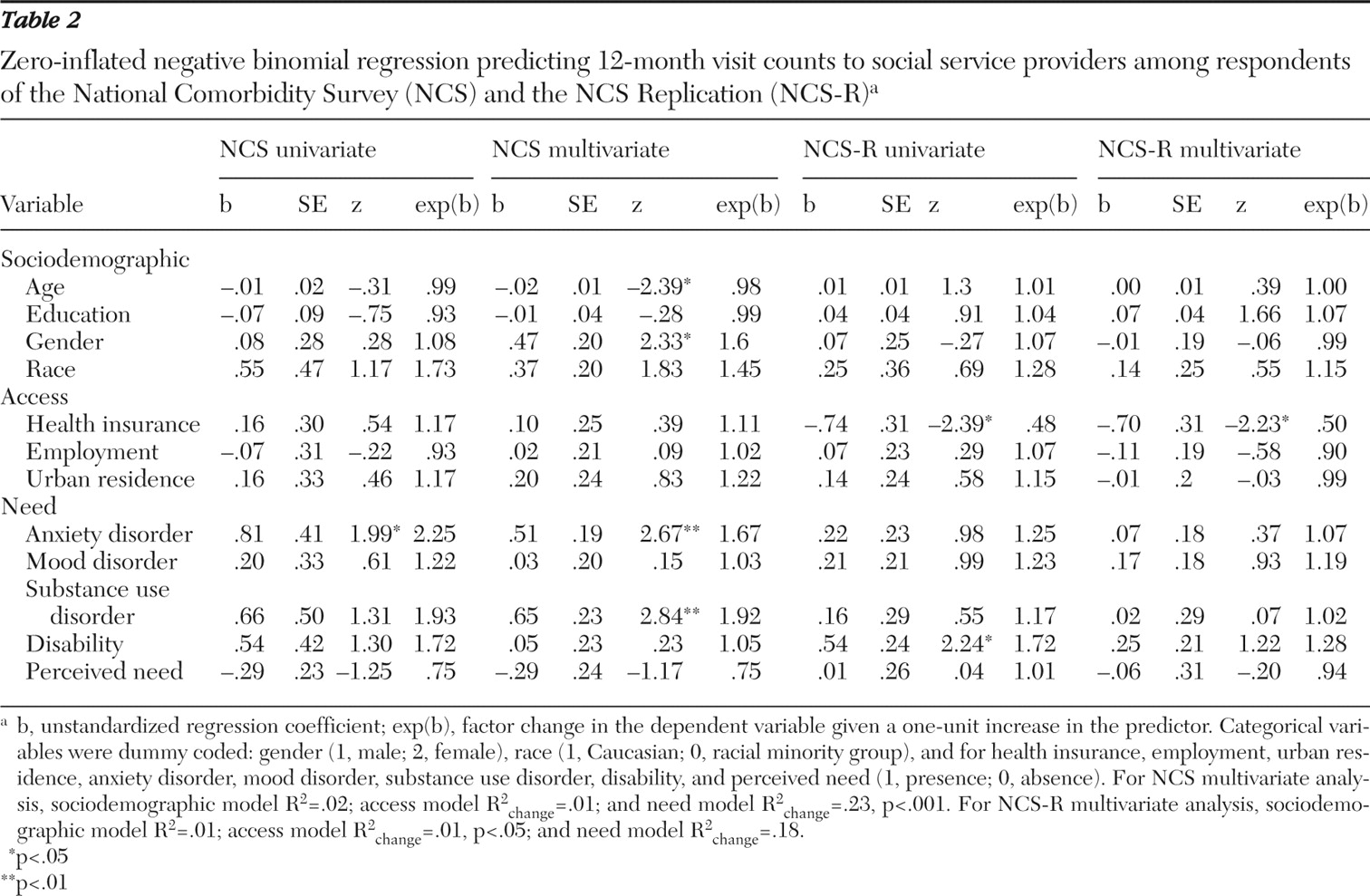
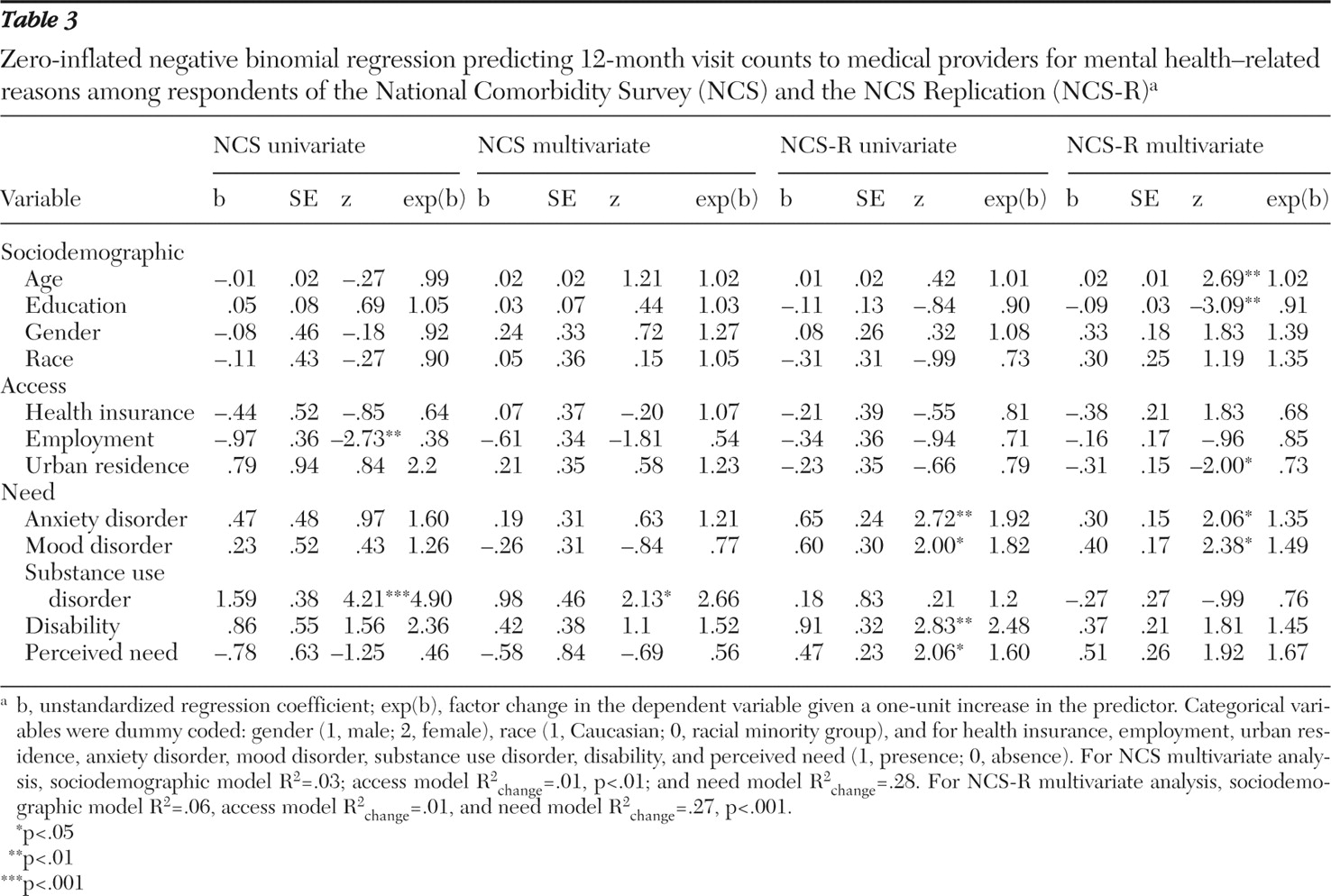
3 report univariate associations between individual predictor variables and visit count outcomes, using univariate ZINB analyses.
Mental health providers. In the NCS data set, only mental health disability was related on a univariate basis to mental health provider visit counts. In the NCS-R data set, in addition to psychiatric disability's association with visit counts, three additional variables were significant: being unemployed, having an anxiety disorder, and having a mood disorder.
Social service providers. In the NCS, only the presence of an anxiety disorder was related on a univariate basis to social service provider visit counts. In the NCS-R data set, two variables were related to social services visits: lacking health insurance and having a mental health disability.
Medical providers. In the NCS data set, two variables were significantly related on a univariate basis to medical provider visit counts: unemployment and having a substance use disorder. In the NCS-R, need variables were related to medical provider visit counts: having an anxiety or mood disorder, having a psychiatric disability, and perceived treatment need.
Multivariate analyses
Tables 1,
2,
3 also present results from multivariate ZINB analyses (final models), testing associations between need variables (step 3) and provider visit count outcomes after first controlling for sociodemographic variables (step 1) and access variables (step 2). For the multivariate analyses, data were available for 5,805 persons in the NCS data set and for 4,220 persons in the NCS-R data set.
Mental health providers. In the NCS data set, the need model (step 3) was significantly associated with mental health provider visit counts ( χ 2 =40.49, df=12, p<.001), contributing incrementally over the access model (likelihood ratio: χ 2 =30.87, df=5, p<.001). Significant final model variables were older age, having more education, being Caucasian, possessing health insurance, and having a psychiatric disability.
In the NCS-R, the need model (step 3) was significantly associated with mental health provider visit counts ( χ 2 =22.84, df=12, p<.05), contributing incrementally over the access model (likelihood ratio: χ 2 =14.06, df=5, p<.05). However, only higher education level was significant in the final model.
Social service providers. In the NCS data set, the need model (step 3) was significantly associated with social service provider visits ( χ 2 =31.24, df=12, p<.01), contributing incrementally over the access model (likelihood ratio: χ 2 =24.57, df=5, p< .001). Being younger, being female, and having an anxiety or substance use disorder were significant.
In the NCS-R data set, the access model (step 2) incrementally enhanced predictions over the sociodemographic model for visits to social service providers (likelihood ratio: χ 2 =10.29, df=3, p<.05), but the need model (step 3) did not contribute additional variance. Lacking health insurance was the only significant variable.
Medical providers. In the NCS, the access model (step 2) incrementally contributed variance over the sociodemographic model (likelihood ratio: χ 2 =23.56, df=3, p<.001), but the need model (step 3) did not contribute incrementally. However, in the final model only having a substance use disorder was significant.
In the NCS-R data set, the need model (step 3) was significantly associated with medical provider visit counts ( χ 2 =61.84, df=12, p<.001), contributing incrementally over the access model (likelihood ratio: χ 2 =54.33, df=5, p<.001). Older age, less education, rural residence, and having an anxiety or mood disorder were significant.
Service use versus service use intensity
We next assessed whether the predictor variables performed differently when using ZINB univariate and multivariate analyses to model service use (service use versus nonuse) versus service use intensity. We found across NCS and NCS-R analyses that variables representing all three factors in the behavioral model of health care use (that is, sociodemographic, access, and need factors) were more consistently significant in predicting service use (especially in the NCS-R) than in predicting treatment intensity (results not displayed; available by request). One exception to this general finding was that some sociodemographic variables (that is, age, gender, race, and education) were nonsignificant in predicting service use, but they became significant in predicting treatment intensity (as noted above). However, this occurred only for NCS multivariate analyses and not for any NCS-R analyses.
More specifically, in the NCS data set, psychiatric disability and perceived need were associated with both use and intensity of mental health care services across multivariate and univariate analyses. Both psychiatric disability and perceived need also were associated with use, but not intensity, of social and medical services. Employment, urban residence, and mood disorder presence were associated with use, but not intensity, of mental health and social services. In the NCS-R data set, disability again was a consistent univariate correlate of both use and intensity across all three service types. On a multivariate basis, other need variables (mood, anxiety, and substance use disorders and perceived need) were associated with use of mental health specialty and social services, as were demographic variables (that is, age and race) and access variables (that is, insurance and employment); however, these variables were not associated with service use intensity.In the medical services domain, however, both service use and intensity had a similar number of correlates in the NCS-R data set, particularly the need variables (anxiety and mood disorders, disability, and perceived need).