Implementation research is devoted to identifying methods that promote the application of new clinical research findings in routine clinical practice (
1 ). Reviews in general medicine (
2 ) and in psychiatry (
3 ) report a considerable time-lag between the discovery of evidence-based practices and their application in practice settings. Although organizational and financial factors account for some of this delay (
4,
5 ), the ongoing education of direct care staff is also a contributing factor. More precisely, the methods that are employed in the continuing education of these staff may be critical. This is the province of implementation research.
An axiom of adult continuing education is that knowledge dissemination alone does not ensure knowledge application and changes in practice behavior. The introduction of motivational theories into the design of continuing education classes has been recommended to overcome this in health care in general (
6 ) and psychiatry in particular (
7 ). The theory of planned behavior is one motivational theory that has recently received attention in implementation research. This theory focuses on the link between intentions and subsequent, deliberate behavior. The theory describes the key variables that affect the strength of our intentions to execute a deliberate behavior. According to this theory, the variables that influence intentions to engage in the behavior are personal beliefs about the outcomes of a behavior, social norms regarding the behavior, and the degree of perceived control over executing the behavior (
8,
9 ). Two meta-analyses have reported that strategies related to the theory of planned behavior were effective in changing a variety of behaviors in clinical populations (
10,
11 ).
The theory has also been shown to predict practice behavior among health care practitioners (
6 ) and mental health practitioners (
7 ). However, only a few implementation research studies have demonstrated that continuing education classes designed according to the principles of the theory of planned behavior were effective in modifying health care staff's intentions to apply new techniques (
12,
13,
14,
15 ). Furthermore, in these studies the magnitude of the relationship between intentions and behavior has been moderate at best. So although the theory of planned behavior specifies variables that are relevant to the intentions-behavior relationship, the identification of additional methods to enhance that relationship has become the focus of implementation research. One possible method that may mediate the intentions-behavior relationship is implementation intentions.
Implementation intentions are plans that we create to initiate our goal-directed behavior in order to achieve our intended goals (
16 ). Implementation intentions comprise a specific goal-directed behavior and the environmental conditions under which this behavior will be initiated. Intentions as described by the theory of planned behavior include some specific goal-directed behavior that is believed to achieve some specified goal. Implementation intentions describe the environmental situations in which we shall initiate the goal-directed behavior. Thus implementation intentions link our chosen goal-directed behavior (the "how") to promising environmental opportunities (the "where" and "when") to initiate our goal-directed behavior. Implementation intentions may strengthen the intentions-behavior relationship by increasing the likelihood of initiating the goal-directed behavior.
Enhanced goal attainment that is associated with the creation of implementation intentions enjoys empirical support (
16,
17,
18,
19,
20,
21,
22,
23,
24,
25 ). Mentally linking our goal-directed behaviors to specific environmental situations reduces the need for effortful thinking, sustained motivation, and even conscious control. A mental connection between behavior and environmental cues establishes an automated link that ensures prompt, efficient execution of goal-directed behavior. There is also empirical support that implementation intentions embrace a preconscious, distinctive mindset (
26,
27,
28 ).
Augmenting with implementation intentions a continuing education class that is designed according to theory of planned behavior principles may enhance the intentions-behavior relationship. The study presented here compared a continuing education class that incorporated implementation intentions with one that did not in order to examine mental health practitioners' practice behavior. The class topic was psychiatric advance directives. The behavior of interest was practitioners' use of a practitioner-guided procedure to assist consumers to complete a psychiatric advance directive. Practitioners were randomly assigned to one of the two conditions, both of which applied the principles of the theory of planned behavior to the classroom format. Accordingly, practitioners' intentions along with their attitudes, subjective norms, and perceived control regarding psychiatric advance directives were assessed before and immediately after both classes. Differences in intentions between the two groups after completion of the class were evaluated via analysis of covariance. No differences in postclass intentions were expected, because both conditions used the same intention-enhancing formats. This analysis was conducted to ensure the functional equivalency of the two conditions in participants' postclass intentions to utilize the practitioner-guided procedure.
Three months after the class the participants anonymously completed an electronic survey about their use of the staff-guided procedure. Comparisons between the two class conditions on this variable employed chi square analysis. It was expected that compared with practitioners in the control class, those in the experimental class that created implementation intentions would exhibit greater utilization of the practitioner-guided procedure with their consumers.
Methods
Setting and participants
Faculty of Drexel University College of Medicine's Department of Psychiatry conducted the classes. Pennsylvania's Office of Mental Health and Substance Abuse Services contracted with Drexel to provide continuing education classes to mental health practitioners throughout the state. Participants were Pennsylvania-based mental health practitioners who elected to register for the class. Drexel's institutional review board approved this study, and registrants were advised in advance that this particular class involved research participation.
Class topic
Psychiatric advance directives are legal documents that stipulate a consumer's treatment preferences or a surrogate decision maker in advance of the consumer's incapacity to make care decisions. In addition to protecting consumers' civil rights, psychiatric advance directives are believed to promote treatment adherence and recovery and to reduce involuntary treatment and costs. Twenty-one states have enacted statutes that describe the rights and responsibilities of consumers and practitioners regarding psychiatric advance directives. However, a recent survey of five major cities (
29 ) found that 66% to 77% of consumers wanted an advance directive, but implementation was at only 4% to 13%.
In January 2005 Pennsylvania's statute on psychiatric advance directives became effective. This continuing education class was created to ensure that practitioners knew about the law and would implement it. The didactic component of this class described the rights and responsibilities of consumers and practitioners under this law. In addition, the class reviewed Pennsylvania's forms for a declaration, for a power of attorney, and for a combined declaration and power of attorney. These forms provided a comprehensive overview of all of the possible elements described in the psychiatric advance directive law. The use of these forms by the practitioners to discuss psychiatric advance directives with consumers was the practitioner-guided procedure. This was the major dependent variable of this study. The selection of this approach as the dependent variable was motivated by a recent study that found that a practitioner-guided approach substantially increased the completion of psychiatric advance directives by consumers, compared with an approach that involved referring consumers to other external agencies (
30 ). The practitioner-guided approach used in this study was modeled after that of the cited study.
The class's interactive component presented selected research from the Web site of the National Resource Center on Psychiatric Advance Directives (
31 ) and selected testimonials from national and local mental health organizations. The selection and presentation of these materials were guided by the participants' attitudes, norms, and perceived control regarding psychiatric advance directives. This information was obtained from the participants' responses to the theory of planned behavior elicitation study that was conducted before the class.
Elicitation study of the theory of planned behavior
The theory details how people's behavior can be modified by the use of communication strategies that alter people's attitudes, norms, and perceived control regarding the targeted behavior. Elicitation studies are surveys that are employed to acquire this information and guide the creation of the communication strategies.
In this study the interactive component of the class was the communication strategy. It was developed in response to an elicitation study that the class registrants completed via e-mail two months before the class. This elicitation study followed the recommendations of Francis and colleagues (
32 ). Registrants were asked to consider the following statement as a personal commitment pronouncement: "I shall in the next three months assist consumers to complete a psychiatric advance directive." They were asked to list the advantages and disadvantages, persons and groups who would approve and disapprove, and the conditions that would make it easy and the ones that would make it difficult when they acted according to the statement. In each of the three response categories, the selection and presentation of the research and testimonial class materials were guided by the responses that were provided by more than 50% of the participants. During this interactive phase, the entire elicitation survey results were presented and discussed with the participants. Participants had the opportunity to confirm or deny the survey findings. Then research findings and testimonials were presented to either counter or support their responses.
Implementation intentions
Implementation intentions were the major independent variables in this study and were created only by the participants in the experimental condition. At the class's conclusion participants in the experimental condition were told that implementation intentions would help them initiate this goal-directed behavior. Implementation intentions were described, and examples were provided. Participants were instructed to create implementation intentions by identifying the best time and place (the "when" and "where") to use the staff-guided procedure (the "how") with consumers. Participants read their implementation intentions aloud, and the instructor provided feedback.
Participants in the control condition spent the remaining time after class by discussing how their intentions to act according to the elicitation study statement had been affected by the class materials.
Instruments
A survey on participant characteristics determined the educational degree, mental health discipline, service role, and years of experience of the participants. Participants also reported whether they had prior training in psychiatric advance directives. A knowledge test comprising 20 multiple-choice questions was constructed for this class. Fifteen items were devoted to the law, and five items focused on the research findings that were presented.
Scales measuring intentions, attitudes, norms, and perceived control were developed according to the principles of the theory of planned behavior that were described by Francis and colleagues (
32 ). The survey comprised 34 items that were rated on a 7-point scale. The intentions scale consisted of eight items. Four of these items described consumers of varying sexes, ages, and treatment adherence. The respondents rated their agreement with assisting these hypothetical consumers to complete a psychiatric advance directive. The attitudes, norms, and perceived control scales comprised ten, eight, and eight items, respectively. These items were derived from the results of the elicitation study.
The follow-up survey was sent electronically to the participants three months after the class. Participants were told to reply by providing their class code number only if they had used the practitioner-guided procedure with any of their consumers. Nonimplementers were instructed not to reply.
Procedures and analyses
The six-hour, one-session class was advertised in print and online at four Pennsylvania population centers. Two months before the class presentations, the registrants were sent the elicitation study survey via e-mail. The elicitation study results were used to design the interactive portion of the class and to create the survey instrument for the theory of planned behavior. Registrants were randomly assigned to one of the two class conditions that were offered during April and May of 2007. Participants anonymously completed the knowledge test and survey at the beginning and again at the completion of each class. The survey on participant characteristics was anonymously completed at the beginning of each class. Three months after the class, the follow-up survey was e-mailed to the participants. Participants' anonymous follow-up survey results were linked to their in-class surveys by a numerical coding system.
Analysis of covariance was applied to pre-post class comparisons between the two class conditions on the knowledge test and intentions scale. This determined the postclass equivalency of the two conditions on these variables. Chi square analysis compared the two class conditions on the follow-up survey variable. This assessed the effect of the implementation intentions on the practitioners' use of the practitioner-guided procedure.
Results
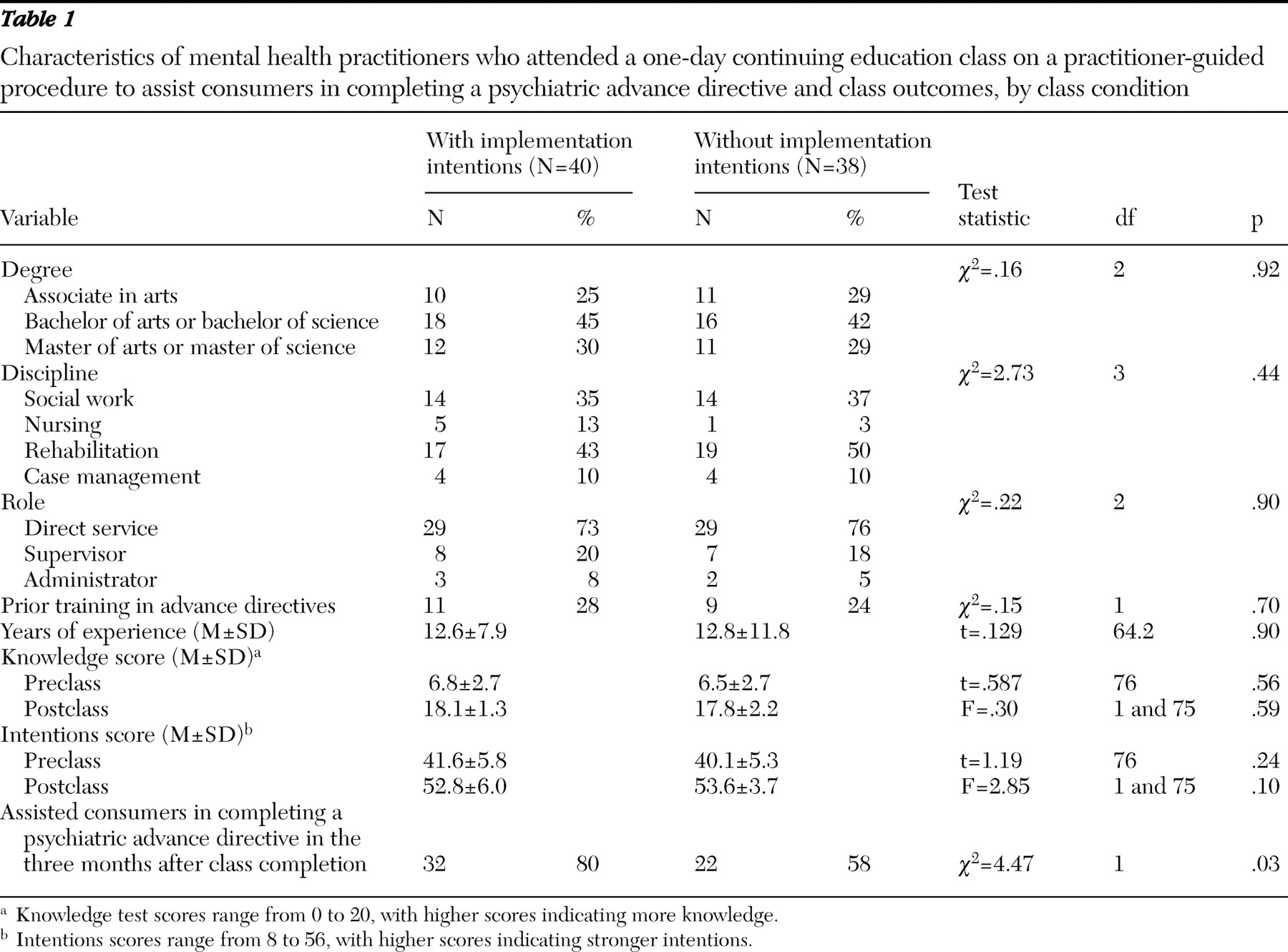
Of the 92 registrants, 78 (85%) attended so that the experimental and control classes comprised 40 and 38 practitioners, respectively. The participants' characteristics are reported in
Table 1 . There were no statistically significant differences between the two class conditions in participant characteristics or preclass knowledge and intentions. These practitioners possessed low levels of knowledge of the psychiatric advance directive law, but they exhibited positive intentions toward assisting consumers to complete a directive.
Preclass attitudes, norms, and perceived control accounted for 66% (R=.81) of the preclass variance in intentions. This is consistent with theory expectations. Another regression analysis that included these three variables along with the participant characteristics and preclass knowledge variables revealed that the variables for the theory of planned behavior accounted for 45% of the preclass variance in intentions, compared with 28% for the other variables (R=.86). The elicitation study appeared to provide valid information regarding the factors associated with these practitioners' intentions to assist consumers to complete a psychiatric advance directive.
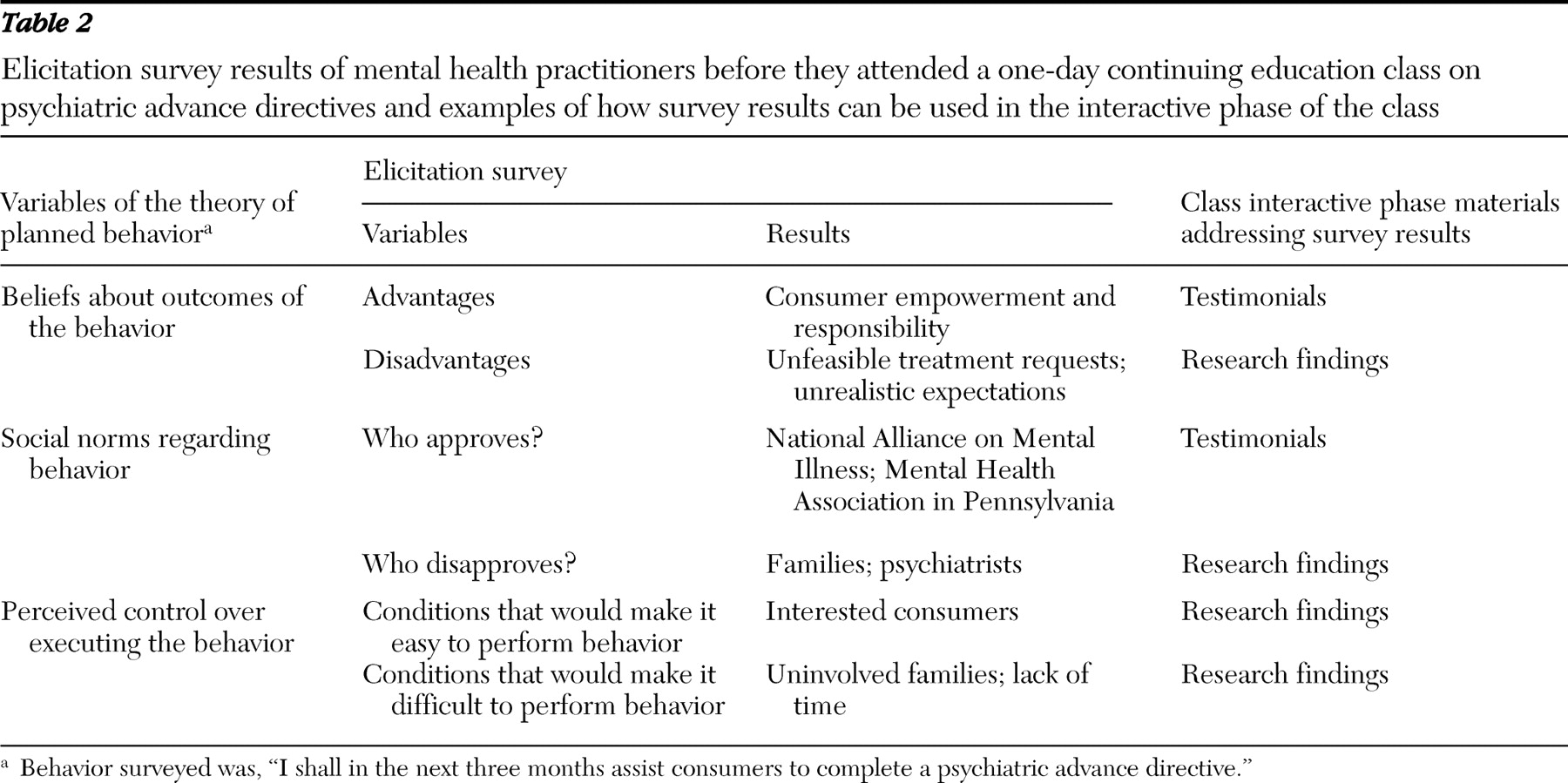
Table 2 reports the results of the elicitation study.
Table 1 also shows that both class conditions achieved substantial increases in both knowledge and intentions at the conclusion of each class. However, the two conditions did not differ significantly in the postclass knowledge or intentions of participants. A panel analysis of the postclass intentions for the total sample (R=.64) found that changes in attitudes, norms, and perceived control accounted for 12% of the variance, whereas knowledge changes accounted for only 1% of the variance. The effectiveness of the elicitation-guided class design in altering practitioners' intentions appeared to be confirmed by this finding.
Despite the equivalent postclass intentions and knowledge of the two class conditions, practitioners who attended the class with implementation intentions reported significantly more cases of practitioner-guided procedure implementation (
Table 1 ) during the follow-up period. Overall postclass intentions were robustly associated with implementation (
η =.70). The effect of implementation intentions on utilization of the practitioner-guided procedure was evident among practitioners whose postclass intentions were high but below the median for the overall sample (
χ 2 =7.1, df=1, p<.01). Implementation rates among practitioners with the highest postclass intentions were equivalent in the two class conditions.
Discussion
Implementation intentions were shown to increase the use of a practice behavior among practitioners who attended a one-day continuing education class. This effect exceeded that caused by knowledge gains or enhanced intentions that were produced by the class. This finding suggests that even well-motivated practitioners can benefit from direct instruction in the use of implementation intentions.
Implementation intentions increased practice use only among practitioners with high but less than maximal scores on the intentions scale. This suggests an interaction between implementation intentions and goal intentions. Previous research found a positive correlation between implementation intention-induced practice rates and intention levels (
25 ). Implementation intentions have little effect on practice when intentions are extremely low. This study suggests the same is true when intentions are extremely high. However, implementation intentions may have a beneficial and unique effect on practice, because not even classes following principles of the theory of planned behavior are likely to yield maximal positive intentions among all participants. Yet, as demonstrated here, the theory of planned behavior substantially enhances intentions among most class participants. Continuing education classes that are designed according to the principles of the theory of planned behavior may be the best candidates for augmentation with implementation intentions.
This study also demonstrated the value of the principles of the theory of planned behavior to design continuing education classes. These results show that the theory specifies the critical factors that were associated with intentions, and intentions were substantially related to practice behavior. The elicitation study provided a valid assessment of these critical factors. As
Table 2 reveals, the elicitation study yielded specific empirical data that may not have been routinely obtained. In addition to identifying practitioners' personal obstacles, elicitation study findings can also reveal organizational and systemic obstacles that affect practice patterns. Making productive use of this type of information may be beyond the scope of traditional continuing education classes. A continuing education class that is informed by the theory of planned behavior would incorporate this information into its design and content.
For example,
Table 2 reveals that the participating practitioners felt that families and psychiatrists would disapprove of their directly assisting consumers with deliberations in regard to psychiatric advance directives. Current research findings suggest that this is a misperception by these practitioners, and these findings were shared with the classes. This was accomplished during the presentation of the elicitation survey findings in the interactive phase of the class. However, this perception could have been based upon actual experiences of these practitioners with some local representatives of these two stakeholder groups. In that case, testimonials or policy positions that offered a broader consensus from these local stakeholders could have been gathered during the class preparation period and then presented during the class. Local, personal views may have more impact on practitioners' intentions than distant and impersonal research findings. The principles and metrics of the theory of planned behavior would routinely provide the opportunity to empirically evaluate this hypothesis. Traditional continuing education formats could not.
This study's findings are limited by its modest sample size and its reliance on self-report measures of the dependent variable. The sample size was adequate to perform the major comparisons. Replication with other types of practitioners and more complex skills are needed to generalize these findings. Self-report data are generally less reliable than independent, objective measures. However, practitioners' replies were anonymous, and there were no benefits or sanctions associated with responding or not. The design of the follow-up survey equated nonresponse with nonimplementation. This may not have been justified in all cases. The observed high positive correlation between responding and postclass intentions provides some justification for this equation. Future research should also explore the long-term effects of implementation intentions on practice and examine what worksite conditions enhance or hinder those effects.
Conclusions
Implementation intentions appear to increase the initiation of practices among mental health practitioners who attend continuing education classes that are guided by the theory of planned behavior. More research should be done to measure the long-term effect of instructing class participants in the formation of implementation intentions.
Acknowledgments and disclosures
The author reports no competing interests.