Depression disorders, one of the major causes of disability-adjusted life years (DALY) (
1 ), have been shown to be underdiagnosed and undertreated and are associated with worse physical health (
2 ), increased health care utilization (
3 ), increased medical costs (
4 ), and high out-of-pocket expenditures (
5 ). Despite the fact that a high financial burden may prevent access to health care, little is known about the financial burden of people with depressive symptoms. This is of particular importance because health care professionals rarely discuss costs issues with their patients (
6 ) and because high health care costs may represent a barrier to treatment compliance (
7 ). In this study, we sought to examine the associations between the presence or absence of depressive symptoms and an individual's financial burden, as well as whether the person forwent care because of costs they would have to pay.
We used baseline (2004) self-reported data from the Survey of Health, Ageing, and Retirement in Europe (SHARE) (
8 ), which included noninstitutionalized individuals 50 years or older. Methodological details of SHARE have been published previously (
9 ). The analytic sample consisted of 16,696 individuals ages 50–79 years. Out-of-pocket payments ("About how much did you pay for all your outpatient care/prescribed drugs, during the last 12 months?") did not include health insurance premiums and reimbursements from employers (
10 ). In order to gather data on the financial burden of out-of-pocket medical expenses, we expressed out-of-pocket expenditures as a percentage of household income. We also analyzed whether individuals forwent medical care because of costs during the past 12 months ("During the last 12 months, did you forgo any types of care because of the costs you would have to pay?"). The presence or absence of clinically significant depressive symptoms was defined by a score <3 on the European Depression (EURO-D) scale, a validated 12-item instrument (
11 ). Possible scores on this scale range from 0 to 12, with higher scores indicating increased severity of depressive symptoms. We performed logistic regressions adjusting for age, gender, marital status, education, subjective health, and chronic diseases.
The overall prevalence of depressive symptoms was 26%. Countries' prevalence varied between a low of 17%–18% in Denmark, Austria, and Switzerland and a high of 31%–35% in Italy and Spain.
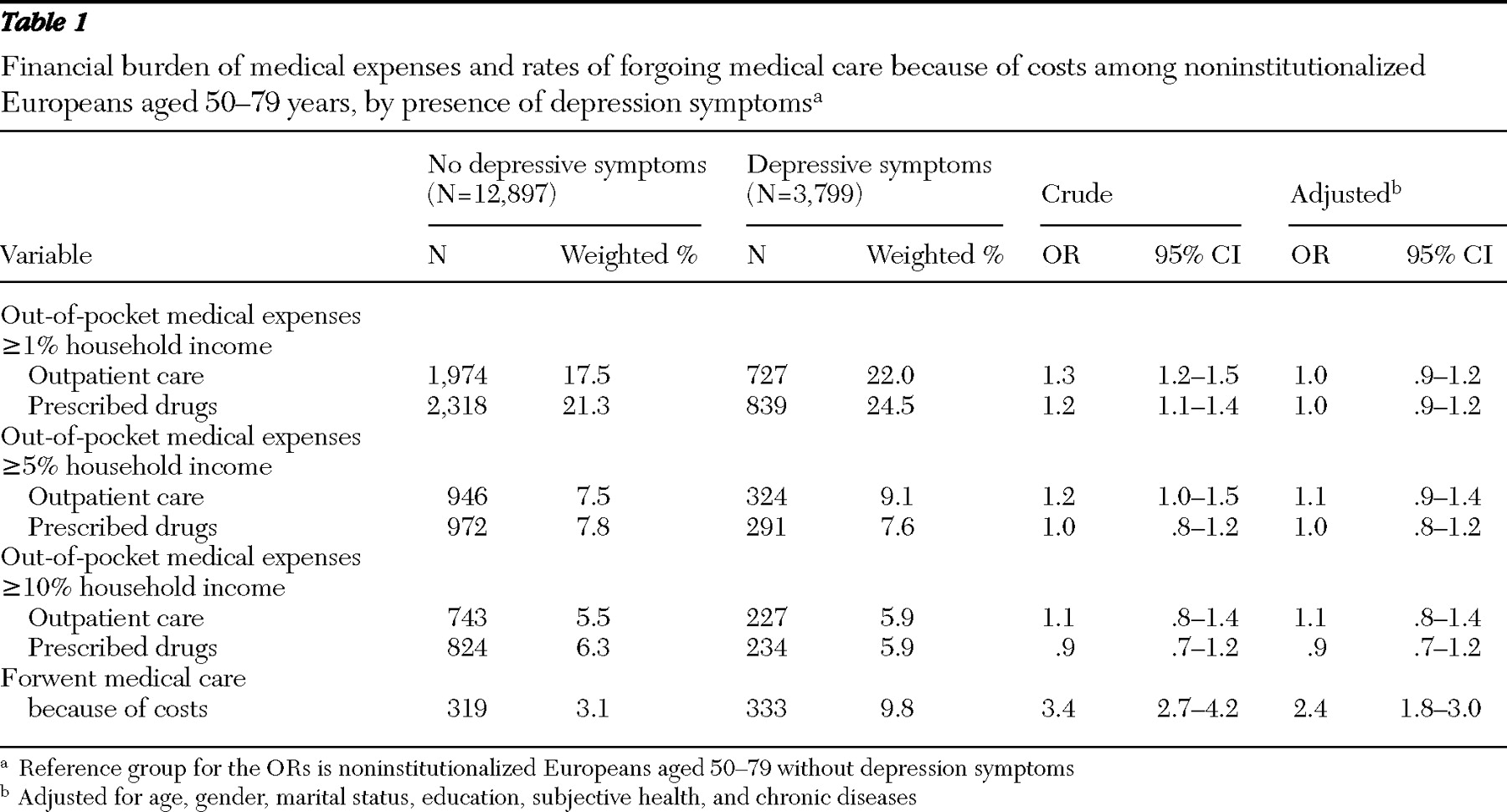
The data on out-of-pocket medical expenses as a percentage of household income across the two groups show that individuals with depressive symptoms were significantly more likely than those without such symptoms to have out-of-pocket expenses ≥1% of their income (
Table 1 ). The presence of depressive symptoms also tripled the proportion of people who forwent health care because of costs (9.8% for persons with depression, and 3.1% for those without depression (
Table 1 ). The crude odds of spending ≥1% of income for outpatient care and prescribed drugs were 32% (odds ratio [OR]=1.3, 95% confidence interval [CI]=1.2–1.5) and 15% (OR=1.2, 95% CI–1.1–1.4) higher, respectively, for people with depressive symptoms, compared with those without such symptoms (
Table 1 ). However, these associations did not remain significant after adjustment for potential confounders (
Table 1 ). Having depressive symptoms increased the risk of forgoing medical care because of costs, even after adjustment for confounding variables (adjusted OR=2.4, 95% CI=1.8–3.0) in all countries except Sweden. Country-level ORs ranged from 1.9 in Germany (95% CI=1.1–3.1) to 4.1 in Greece (95% CI=2.4–6.8).
Discussion
Even though persons with depressive symptoms and those without such symptoms bore a similar financial health care burden, individuals with depressive symptoms were at increased risk of forgoing care because of costs they would have to pay.
Patients with chronic diseases have been shown to pay substantial portions of total income for out-of-pocket health expenses (
12 ). Therefore, it is encouraging to remark that the presence of depressive symptoms did not seem to impose a high burden on the household income of those with depression. However, because individuals with depression reported forgoing care because of costs, we might hypothesize that our results reflect decisions to give up health care. Assessment of depressive status relied on a population-based questionnaire. Therefore, refusal to provide care or reimbursement for care among individuals with depressive symptoms was unlikely; in most cases both respondents and their health care professionals were probably not aware of the presence of depressive symptoms. In fact, individuals with depressive symptoms might have used health care as long as they were responsible for only a small portion of the financial contribution. However, if they had to pay a higher portion of their health care, they would have been inclined to forgo care because of costs. In fact, many studies have shown that out-of-pocket expenses could lead to decreased health care utilization and subsequent deterioration of health status (
13 ).
The strengths of our study include the availability of a large data set representative of noninstitutionalized individuals from ten European countries and the availability of data on the financial burden of individuals. The latter is interesting because it includes information on the persons' ability to pay. However, the study has potential limitations. There is evidence suggesting that although self-reported income is generally underestimated, both over- and underestimation of out-of-pocket expenses may lead to misreporting. However, if both types of misreporting remain constant across groups, "comparisons across groups remain valid even if the total estimates of burden are biased" (
14 ). Also, we were unable to distinguish between care for health, in general, and care for depressive symptoms. Finally, we may have underestimated our variances because we could not appropriately account for SHARE's complex survey design. Because adjusted ORs for out-of-pocket medical expenses as a percentage of household income were not significant, and because adjusted ORs for forgoing medical care were largely significant, our results and discussion should be robust to slightly larger variances.
Conclusions
Our results suggest that, regardless of the country considered, individuals with depressive symptoms and those without such symptoms bear similar financial burdens. However, the fact that persons with depressive symptoms reported an increased risk of forgoing any type of medical care because of costs may worsen their health and financial situation. To facilitate the development of suggestions for policy implications, additional research is needed to understand how out-of-pocket expenses influence access to care for individuals with depressive disorders, to investigate more precisely which types of care were forgone, and to examine whether forgoing care was related to patients', providers', or health care systems' characteristics. In the meantime, health care professionals should be aware that health care costs may represent a barrier to care for individuals with depressive symptoms, even in European countries with almost universal health insurance coverage.
Acknowledgments and disclosures
This study used data from the early release I of the 2004 Survey of Health, Ageing, and Retirement in Europe (SHARE). The SHARE data collection has been primarily funded by the European Commission through the 5th Framework Program (project QLK6-CT-2001-00360 in the thematic program Quality of Life). Additional funding came from the U.S. National Institute on Aging (U01-AG09740-13S2, P01-AG005842, P01-AG08291, P30-AG12815, Y1-AG-4553-01, and OGHA 04-064). Data collection was nationally funded in Austria (through the Austrian Science Fund, FWF [Fonds zur Förderung der wissenschaftlichen Forschung]), in Belgium (through the Belgian Science Policy Office), and in Switzerland (through BBW/OFES/ UFES [Bundesamt für Bildung und Wissenschaft/Office fédéral de l'éducation et de la science/Ufficio federale dell'educazione e della scienza]). The SHARE data set was introduced in a publication edited by Börsch-Supan and colleagues (
10 ); methodological details are available in a publication edited by Börsch-Supan and Jürges (
9 ).
The authors report no competing interests.