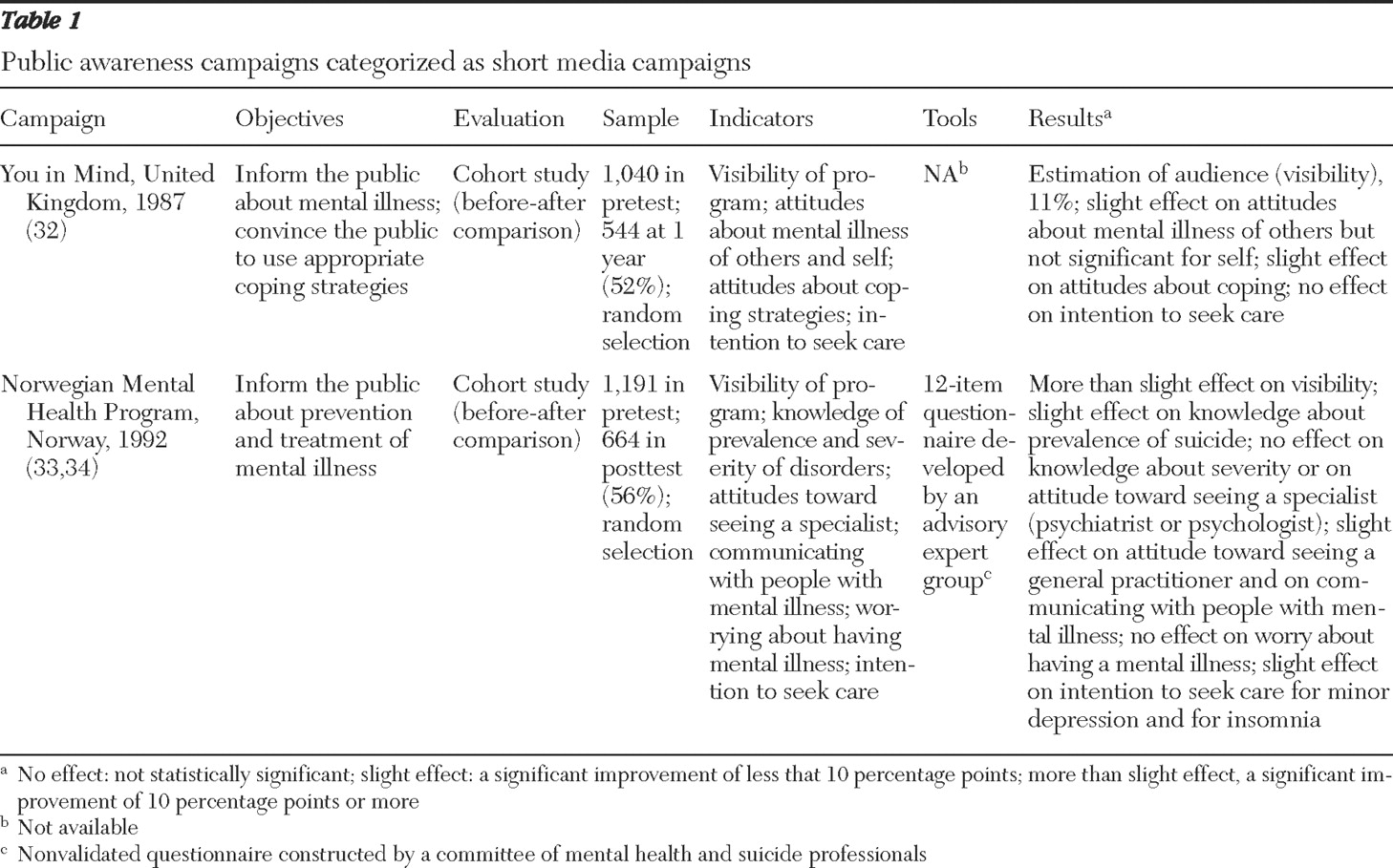
The search yielded 200 reference citations, and 43 of the cited publications met our inclusion criteria. They covered 15 programs in eight countries. We found publications describing U.S. programs, but we did not include them in the review because they did not meet our inclusion criteria. We classified the programs into four categories: short media campaigns, which involved a single exposure (
32,
33,
34 ) (
Table 1 ); gatekeeper training programs (
35,
36,
37,
38,
39,
40,
41,
42,
43 ) (
Table 2 ); and long programs involving repeated exposures, conducted on either a national scale (
44,
45,
46,
47,
48,
49,
50,
51,
52,
53,
54,
55,
56,
57,
58,
59,
60,
61,
62 ) (
Table 3 ) or a local scale (
63,
64,
65,
66,
67,
68,
69,
70,
71,
72 ) (
Table 4 ). In addition to describing the programs, the tables present evaluation information. Almost all the programs sought to improve knowledge about depression or suicidal crises—that is, at a minimum the program had one or both of these specific aims—and to reduce discrimination, counter misconceptions, and enhance help seeking. Only three programs, all local, were aimed specifically at reducing suicide risks (
67,
68,
71 ).
Gatekeeper training
Gatekeeper training—training community members to identify people with problems and direct them toward assistance—has been applied in the workplace, in the military, (
35,
36,
37 ), and among police officers (
38 ). It has been shown to reduce suicide rates (
35,
36,
38 ) and suicide risks (
37 ). Because these programs targeted specific occupations, they are not described in
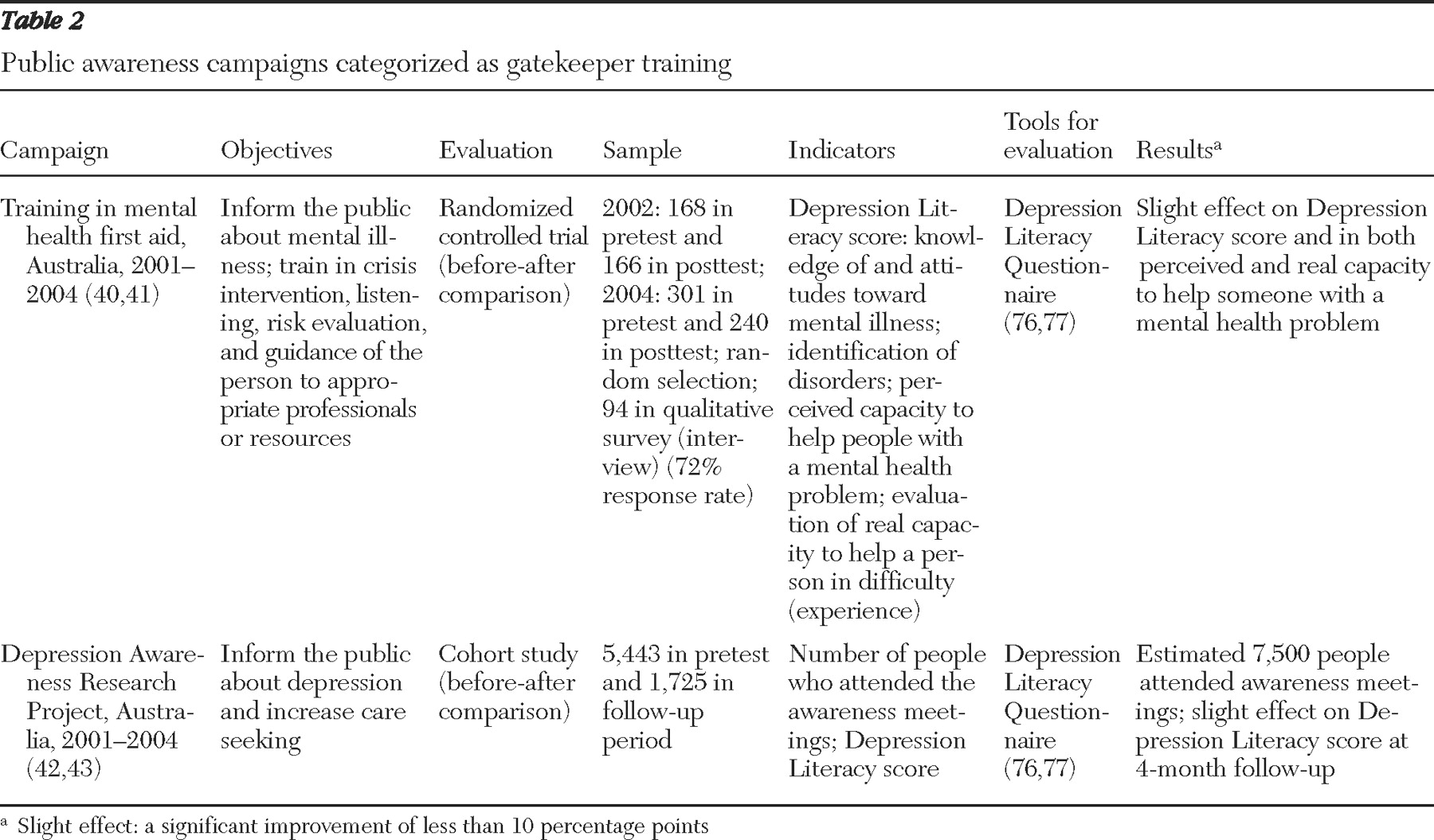
Table 2, which presents information on programs in the gatekeeper training category.
The 1997 Australian Survey of Mental Health and Wellbeing showed that a substantial proportion of individuals did not know how to behave with people who have mental illness, especially during crises (
39 ). The "mental health first aid" program was set up in 2001 in Australia to teach professionals and the general population how to help "a person developing a mental health problem or in a mental health crisis … until appropriate professional treatment is received or until the crisis resolves." The course, initially nine hours long and subsequently expanded to 12 hours, described steps for providing early help to adults in crisis situations or developing a mental illness: assess the risk level, listen nonjudgmentally, reassure and inform, and encourage the person to see a professional. By the end of 2007 a total of 600 instructors had been trained in Australia. The program has been replicated in numerous countries. Successive assessments suggest that the training increases participants' capacity to recognize mental illness, raising their knowledge to a level close to that of mental health professionals, and reduces stigmatizing attitudes and social distance between participants and people with mental illness (
40,
41 ). After training, participants reported increased confidence that they could help people in crisis. The improvements continued to be evident at six-month follow-up (
40 ). A qualitative study of former participants' experiences showed that 78% had used what they learned in the mental health first aid program to help people and 79% were sure that they had been able to help people with problems (
41 ).
A program of this type was set up in the Australian state of Victoria from 2001 to 2004. The Depression Awareness Research Project sought to make communities aware of depression and to reduce its associated stigma (
42,
43 ). The principle was to recruit and train "educators"—more than 200 in three years—who were then assigned to lead awareness meetings within their communities. The following key messages were delivered: depression is common, it is a disease and not a charactertrait, and it is a serious but treatable disease. The evaluation indicated that among people who attended the community meetings, mental health education levels remained significantly elevated four months later.
Long national programs
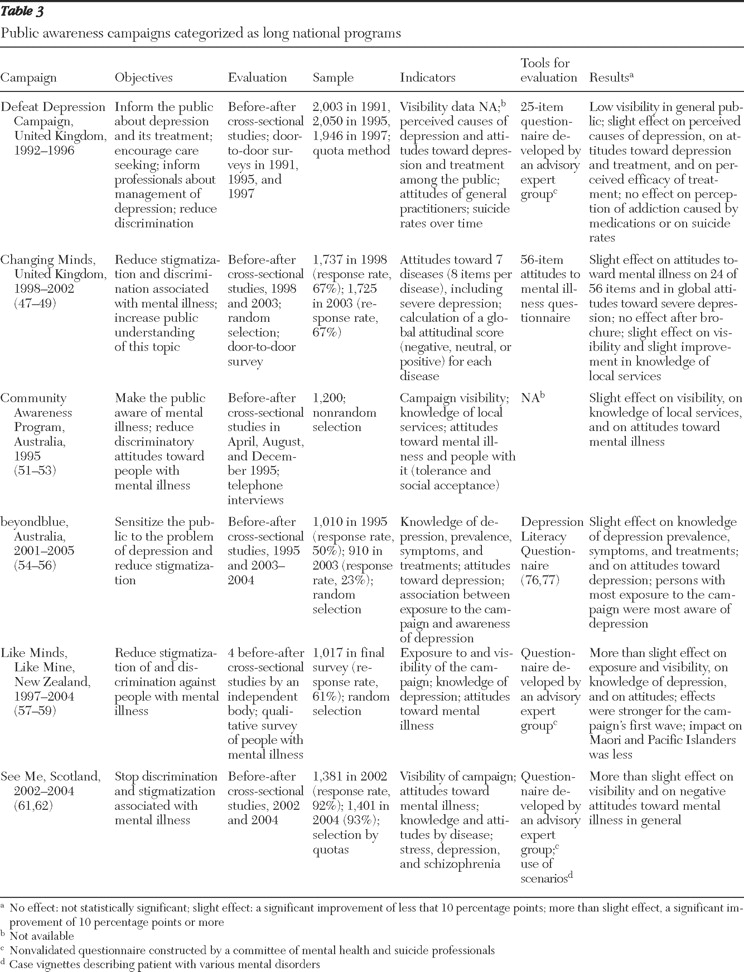
Table 3 provides information on long national programs. Most long programs used several concomitant strategies, including, for example, screening, professional training, media education, and restriction of access to lethal means.
In the United Kingdom, the Royal College of Psychiatrists implemented the Defeat Depression Campaign in 1992 (
44,
45,
46 ). It lasted five years and had three principal objectives: educate health care professionals, especially general practitioners, to recognize and manage depression; make the public aware of depression and of various treatment options to encourage early care seeking; and reduce discrimination associated with depression. The key message—that depression is a common disease, serious but treatable—was disseminated to the public in a three-week media campaign each year in 1994, 1995, and 1996. More detailed messages were disseminated by use of audio- and videocassettes and books aimed at several population subgroups, and these messages were debated during seminars and conferences. Brochures addressing certain aspects of depression (for example, among elderly persons, among coworkers, or among postnatal women) were translated into several languages and made available at the campaign's Web site.
Evaluations indicated that this program was barely visible to the public; it was estimated that 5% of the public were aware of the campaign in 1995 and 2% in 1997 (
44,
45 ). The Defeat Depression Campaign increased population awareness of depression and various treatment options only slightly. For example, from 1991, before the campaign began, to 1997, a year after it ended, the proportion of respondents who recognized that depression is a disease increased by less than 10%. The perception of available treatments also changed little: in both 1991 and 1997 most respondents considered both antidepressants and tranquilizers to be addictive. Finally, suicide rates did not change significantly.
The Royal College of Psychiatristslaunched its next program, Changing Minds, in 1998 (
47,
48,
49 ). Over a five-year period, the program addressed six of the most common mental disorders, including depression, in order to reduce the stigma and discrimination associated with them. The campaign relied on distribution of educational material in various formats for each disorder. They included a book of first-hand accounts by people with mental illness, brochures and books aimed at various target populations, and a scientific report on attitudes and behaviors among health care professionals that maintained discrimination and stigmatization (
50 ). Several media campaigns were conducted simultaneously. The evaluation of this program indicated a significant reduction of several percentage points in the proportion of people expressing negative attitudes toward individuals with mental illness. Nineteen percent of interviewees in 2003 reported that persons with severe depression were dangerous, compared with 23% in 1998. In addition, 56% reported in 2003 that it was difficult to talk with severely depressed persons, compared with 62% in 1998.
A mental health educational campaign, the Community Awareness Program, was launched in April 1995 in Australia to inform the public about mental illness, including depression, and reduce discrimination toward people with these illnesses (
51,
52,
53 ). The program included a campaign that presented advertisements on television and in movie theaters as well as on a billboard and in other types of displays. The campaign involved two successive phases of exposure, two months apart, and distribution of an information kit for mental health professionals, general practitioners, and schools. It delivered the following key messages: anyone can have a mental illness, mental illness is a disease like any other, help is available for people with mental illnesses, and mental illnesses can be cured. Brochures were edited to address the various mental illnesses targeted in the campaign.
Assessments indicated that awareness of mental illness among persons who were questioned increased: before the campaign 61% reported having seen, heard, or read something about mental health, and after the first and the second waves of the campaign, the proportions were 66% and 70%, respectively. People who were exposed to the campaign were more likely than those who were not to report that they would be willing to engage in social or work relationships with people with mental illness. A slight increase in knowledge of available services was also observed after the campaign. However, to the best of our knowledge, no specific results about depression were published.
In 2001 Australia launched the national "beyondblue" project to increase the population's ability to prevent and respond to depression (
54,
55,
56 ). This program combined various levels of actions and aimed especially to create community awareness and mobilization about depression, reduce discrimination, and improve support of people with mental illness. A media campaign presented the experiences of Australians affected by depression and delivered the following message: depression is a major health problem in Australia that can be recognized by specific signs and symptoms. The presentations also explained how to react to a person with depression and how to find help. People with mental illness participated in the project's design and implementation. The evaluation showed improvements in public knowledge and attitudes about depression (for example, fewer false beliefs), especially in the states where the campaign was most active (
56 ).
The Like Minds, Like Mine project began in 1997 in New Zealand to change attitudes about and behavior toward people with mental illness, including depression, by reducing negative stereotypes (
57,
58,
59 ). People with mental illness participated in all stages of the program, which combined regional and community action, training and education of professionals and media, and a media campaign (waves of exposure in 2000, 2002, and 2004) with other communication strategies—for example, a Web site and four newsletters a year. The first wave of the media campaign presented accounts by celebrities and "ordinary"people who had had a mental illness. During the second wave, well-known personalities talked about the importance of social support. The last wave challenged some common ideas about people with mental illness and disseminated the slogan "Learn to know people before you judge them." Specific ads were addressed to different communities (Maori, Pacific Islanders, and Pakeha).
In evaluations half of the people questioned reported that they had seen or heard at least one of the campaign's ads after the first wave of exposure, and the proportion was 75% after the second wave. Recall of the principal messages about support and discrimination increased with the number of waves of exposure (from 32% to 50%), as did recall of the availability of help (from 7% to 17%). The results also suggested improvement in knowledge of mental illness and attitudes toward people with mental illness. In particular, awareness of depression increased from 28% to 49% between the first and fourth surveys. The impact was smaller in some ethnic communities, such as the Maori and Pacific Islander communities. An evaluation in which people with mental illness were interviewed found that 85% considered the campaign to have "helped a little or a lot to reduce the stigmatization and discrimination associated with mental illness"(
58 ).
At the end of 2002 Scotland launched a national suicide prevention plan, Choose Life (
60 ). A key activity was a media campaign against stigmatization, See Me, which was based on accounts of people with mental illness (
61,
62 ). This campaign, organized in four waves, included a billboard and display campaign, distribution of educational materials, and creation of a Web site. Evaluations showed that the program increased the general public's awareness of mental health. Seventy-two percent of those questioned in 2004 reported having seen, heard, or read something about mental health during the year, compared with 43% in 2002. Television was the campaign's most effective and visible medium. Moreover, 60% of those questioned believed that the campaign was likely to modify their attitudes toward people with mental illness. Over two years, a significant reduction was noted in reported negative attitudes. For example, the proportion of people who agreed with the following statement fell by 5 percentage points: "If I had a mental illness, I would not want anyone to know," and the proportion who agreed that "people with mental illness are often dangerous" fell by 17 percentage points. A very slight increase in positive attitudes was also found.
Local and community programs
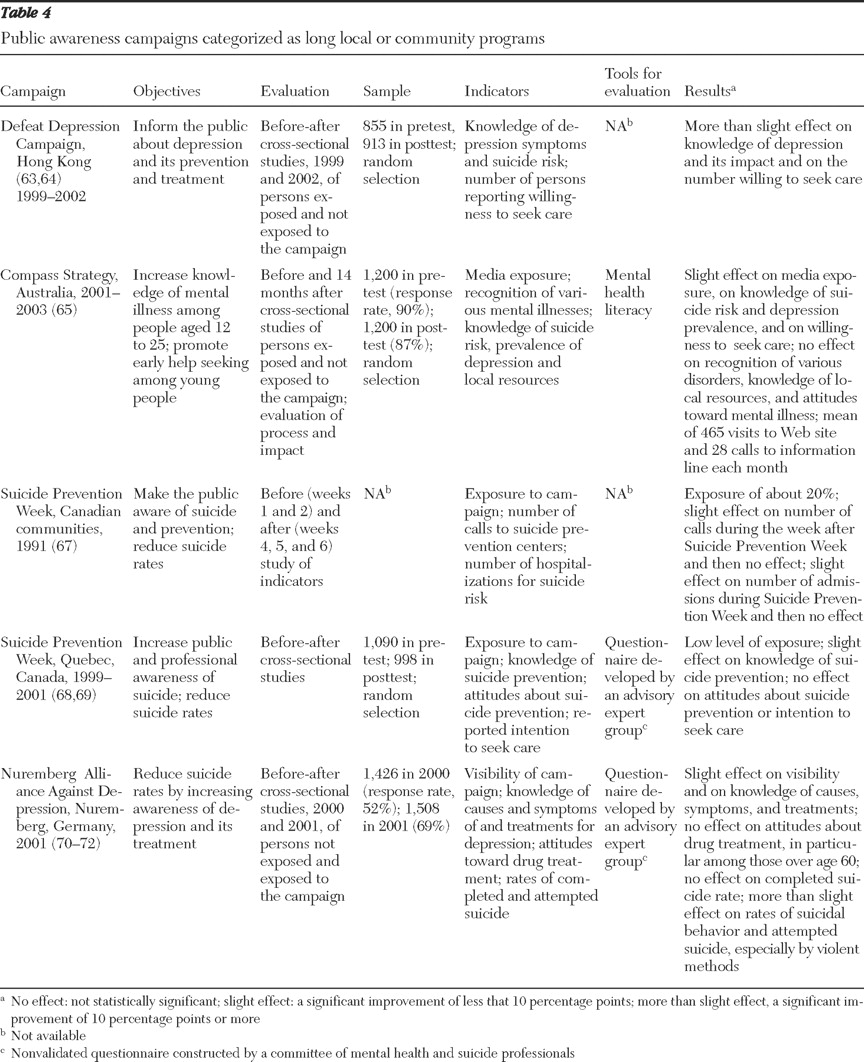
Table 4 presents information on local and community programs. The Defeat Depression Campaign was a four-year program established in 1999 in western Hong Kong to inform Chinese-speaking communities about depression and its prevention and treatment (
63,
64 ). After a preliminary study of inhabitants' needs, it distributed educational material, in particular brochures from the U.K. Defeat Depression Campaign that were translated into Chinese. With the help of local media and a Web site, the campaign also organized more than 30 events on the topic of depression, including road shows and exhibitions. In 2001 and 2002 a radio series broadcast 20-minute case studies about depression in several at-risk groups. A training kit was also distributed to professionals, particularly to physicians. The pre-post evaluation study showed a significant improvement in public knowledge about depression; 54% of respondents understood that depression was a mental illness in 1999, compared with 77% in 2002 (p<.01). Moreover, more people reported seeking formal treatment—2.1% in 1999, compared with 9.1% in 2002 (p<.01).
The Compass Strategy program, conducted in the Melbourne, Australia, region from 2001 through 2003, targeted the population aged 12 to 25 years to promote early diagnosis and treatment of mental illness (
65 ). It was based on the Precede-Proceed health promotion model (
66 ) and on a detailed study of the epidemiologic, environmental, cultural, and social context in which the program was to be implemented and used a variety of media: a large billboard campaign, distribution of educational material, a Web site, and a telephone information service. The evaluation indicated that in the exposed region, knowledge of suicide risks associated with depression and of the prevalence of mental illness improved, negative attitudes toward help seeking were reduced, perception of treatments and their effectiveness became more positive, the proportion of people who considered themselves depressed increased slightly but significantly, help-seeking behavior increased significantly but not among those who perceived themselves as depressed, and knowledge of resources and recognition of various mental illnesses did not improve.
Local and community programs to reduce suicide rates
Thematic days or weeks organized each year in various countries, such as international suicide day and mental health information week, aim to increase population awareness and mobilize professionals around the issue of suicide—and mental illness more broadly—to reduce stigmatization and promote care seeking. More specifically, Suicide Prevention Week (SPW) is an annual event organized to reduce suicide rates over the long term. Generally, the broad themes are decided upon each year at the national level, and local or community implementation is then organized. As part of SPW in Canada, assessments were conducted locally in 1991 (
67 ) and in Quebec province from 1999 to 2001 (
68,
69 ). Suicide prevention centers prepare and distribute promotional material and organize local media campaigns, training workshops, and seminars. The 1991 evaluation indicated that the number of calls and visits to suicide prevention centers increased, as did hospital admissions for mental illness, but only in the week following SPW. From 1999 to 2001 evaluations in Quebec revealed the poor visibility of SPW: knowledge about suicide crises improved but not negative attitudes toward people who are suicidal. Statements of intent to seek help and the number of calls and visits to suicide prevention centers did not change.
The Nuremberg Alliance Against Depression was launched in 2001 in Germany for two years to improve the identification and management of depression and to reduce suicide rates (
70,
71,
72 ). It combined a public awareness campaign, cooperation with general practitioners, gatekeepers (for example, teachers, priests, and police officers), and support of self-help activities by people with mental illness. The evaluation of the awareness campaign found improved knowledge about depression and its treatment; a significant reduction—approximately 20%—in suicidal behavior (attempted and completed suicides) in Nuremberg compared with Wurzburg, a city that was not exposed to the program; and no significant effect on negative public attitudes about antidepressants (
70 ). The project was replicated in several regions of Germany and served as a model for the European Alliance Against Depression, a project launched in 16 European regions in 2004 (
73 ).