Although psychotherapy is clearly an effective treatment for depression (
1,
2,
3,
4 ), it reaches only a fraction of those who might benefit. Guidelines endorse psychotherapy as a first-line treatment for outpatients with depression (
5,
6,
7 ), and surveys of people with depressive disorders have found that 50%–60% prefer psychotherapy for initial treatment (
8,
9,
10 ). Nevertheless, only half of depression treatment episodes in the United States include any psychotherapy (
11 ), and only 14% of adults with a depressive disorder make four or more counseling visits over one year (
12 ). The rate of depression treatment has doubled over the past 15 years, but use of psychotherapy has remained flat or decreased (
13,
14,
15 ). Given this disparity between need, preference, and actual use, it is essential to understand why people with depressive disorders start and continue psychotherapy.
A surprisingly small body of literature has examined dropout before the first psychotherapy visit. Zivin and colleagues (
16 ) examined initial visit attendance in a university-based managed mental health care organization. Over the 90 days after a screening telephone call to request an initial psychotherapy visit, 85% of callers attended at least one mental health visit. Attendance was positively associated with self-rated family support, previous mental health treatment, and recent alcohol use, and it was negatively associated with a past suicide attempt, self-reported legal problems, and recent use of medical services. Attendance was not related to severity of depression, but the sample included members seeking treatment for a wide range of problems. Other studies have found no-show rates of 25%–40% for initial appointments at community mental health centers serving populations that were more disadvantaged or severely ill (
17,
18,
19 ). In those samples, dropout was typically associated with younger age, minority race or ethnicity, no previous mental health treatment, and a longer time between screening and the initial visit. Previous studies have all examined dropout for mental health visits in general and have not specifically examined psychotherapy for treatment of depression.
A moderate body of literature has considered dropout after an initial psychotherapy visit. In a sample identified from insurance claims, only 55% of adults starting psychotherapy for depression continued for at least four visits (
11 ). Other research regarding adherence to psychotherapy has been conducted in less representative settings, such as clinical trials (
20 ), academic centers (
21 ), or student clinics (
22 ). Those studies, however, all indicate high rates of early dropout. Studies examining mental health treatment in general (including psychotherapy and other treatments) have found that dropout is associated with younger age, lower income and educational attainment, lower social support, and substance use disorders (
20,
21,
22,
23,
24,
25 ).
This study examined probability of early dropout in a community-based sample of insured adults calling to request psychotherapy for depression. We focused on three groups of predictors for early dropout: demographic characteristics, clinical characteristics (severity of depression and perceived need for treatment), and health system characteristics.
Methods
Group Health Cooperative is a not-for-profit health system serving approximately 600,000 members in Washington and Idaho. Members are enrolled through private employers (53% of members), state and federal employers (22% of members), individually purchased plans (5% of members), a capitated Medicare plan (12% of members), and publicly funded plans, such as Medicaid, for low-income residents (8% of members). Group Health members are similar to the area population in income, educational attainment, and racial-ethnic composition. Members may directly request specialty mental health care without referral or other authorization. Copayments for outpatient psychotherapy vary by source of insurance coverage and are similar to national averages (
26 ): $10 or less for approximately 35% of members, $15 or $20 for approximately 45% of members, and greater than $20 for approximately 20% of members.
All members requesting mental health services call a centralized screening program. Physician referrals for mental health services are routed to this screening program, and screening specialists initiate outgoing calls. All screening specialists are master's-level and licensed mental health providers. Each screening contact (incoming or outgoing) includes a structured assessment of the member's primary problem, current or recent mental health treatment, perceived urgency, screening for substance use disorders, and risk of harm to self or others. In most cases, callers request a specific service (for example, individual psychotherapy, medication evaluation, or chemical dependency treatment). In the remaining cases, the screening specialist describes available services and clarifies the caller's needs and preferences. The screening unit completes approximately 20,000 assessments each year. In 2008 the most common presenting problems were depression (34%), adjustment or interpersonal problems (19%), anxiety (14%), and attention deficit disorder (7%). The average length of a screening contact is approximately ten minutes.
Group Health provides specialty mental health care using both salaried internal or group-model providers and a network of contracted external fee-for-service providers. Seven group-model mental health clinics in Washington serve members in or near the cities of Bellevue, Bremerton, Olympia, Seattle, Spokane, and Tacoma, and they have a combined staff of approximately 15 psychiatrists, ten doctoral-level psychologists, and 60 master's-level psychotherapists. For internal providers, guidelines and training emphasize cognitive-behavioral therapy for treatment of depression. The network of contracted fee-for-service health providers includes over 300 providers (psychiatrists, doctoral-level psychologists, and master's-level psychotherapists throughout Washington and northern Idaho. Visits to network providers are reimbursed on a fee-for-service basis at contracted rates.
At the end of each screening call, the screening specialist offers either a referral to a contracted network provider or an appointment with a group-model provider according the caller's geographic location and the availability of appointments with group-model providers. All callers residing outside the service areas of group-model clinics (primarily more suburban and rural members) are offered referrals to network providers. Callers residing within the service areas of group-model clinics are generally offered appointments with group-model providers, but may be offered referrals to network providers if no appropriate group-model appointments are available within two weeks. Callers directed to group-model providers are offered a specific appointment during the screening call. Callers referred to network providers are given contact information for three or more contracted network providers in the caller's area and advised to call back once an in initial appointment is scheduled (to allow a formal authorization for payment). Approximately 85% of appointments or referrals for psychotherapy involve master's-level therapists, approximately 15% involve doctoral-level psychologists, and fewer than 5% involve psychiatrists. Callers requesting psychotherapy might be already receiving pharmacotherapy or might initiate pharmacotherapy (from a psychiatrist or primary care physician) after the screening call.
For this research, screening staff were asked to offer study participation to every adult caller requesting psychotherapy for treatment of depression. Eligible callers were asked to respond to additional research questions at the end of the screening call and to give permission to use records for research. Additional questions for this research included the two-item screening version of the Patient Health Questionnaire depression scale (PHQ-2) (
27,
28,
29 ), as well as self-ratings of the perceived importance of initiating psychotherapy at the time of the call and the caller's confidence that therapy would be helpful. The latter two items were rated on a scale as being not at all important, a little important, moderately important, very important, and extremely important. Possible PHQ-2 scores range from 0 to 6, with scores of 2 or less indicating mild symptoms of depression, scores of 3 or 4 indicating moderate symptoms, and scores of 5 or 6 indicating severe symptoms.
For all consenting participants, data collected during the screening call were linked to insurance claims data to identify all psychotherapy visits to group-model or network-model providers during the following 90 days.
All study procedures were reviewed and approved by the Group Health Human Subjects Review Committee. Because of the minimal risk to participants, the committee approved a documented oral consent procedure in lieu of written consent. Each participant listened to a script describing study procedures and risks and provided documented oral consent to participate.
Results
Participants were enrolled between July 2008 and October 2008. Of 318 eligible callers, 238 (75%) agreed to complete survey items and gave permission to use records for research. Participants had a mean age of 40±17 years, and 70% were female. Symptoms of depression were mild for 22%, moderate for 35%, and severe for 43% (
Table 1 ).
No identifying information was retained for the 80 callers who declined participation, and no additional information is available regarding nonparticipants. We were, however, able to compare study participants to the entire population of callers in 2008 who met our eligibility criteria (adults calling to request an initial psychotherapy visit for a chief complaint of depression). Study participants did not differ significantly from the entire population in mean age, sex distribution, or the proportion attending an initial psychotherapy visit.
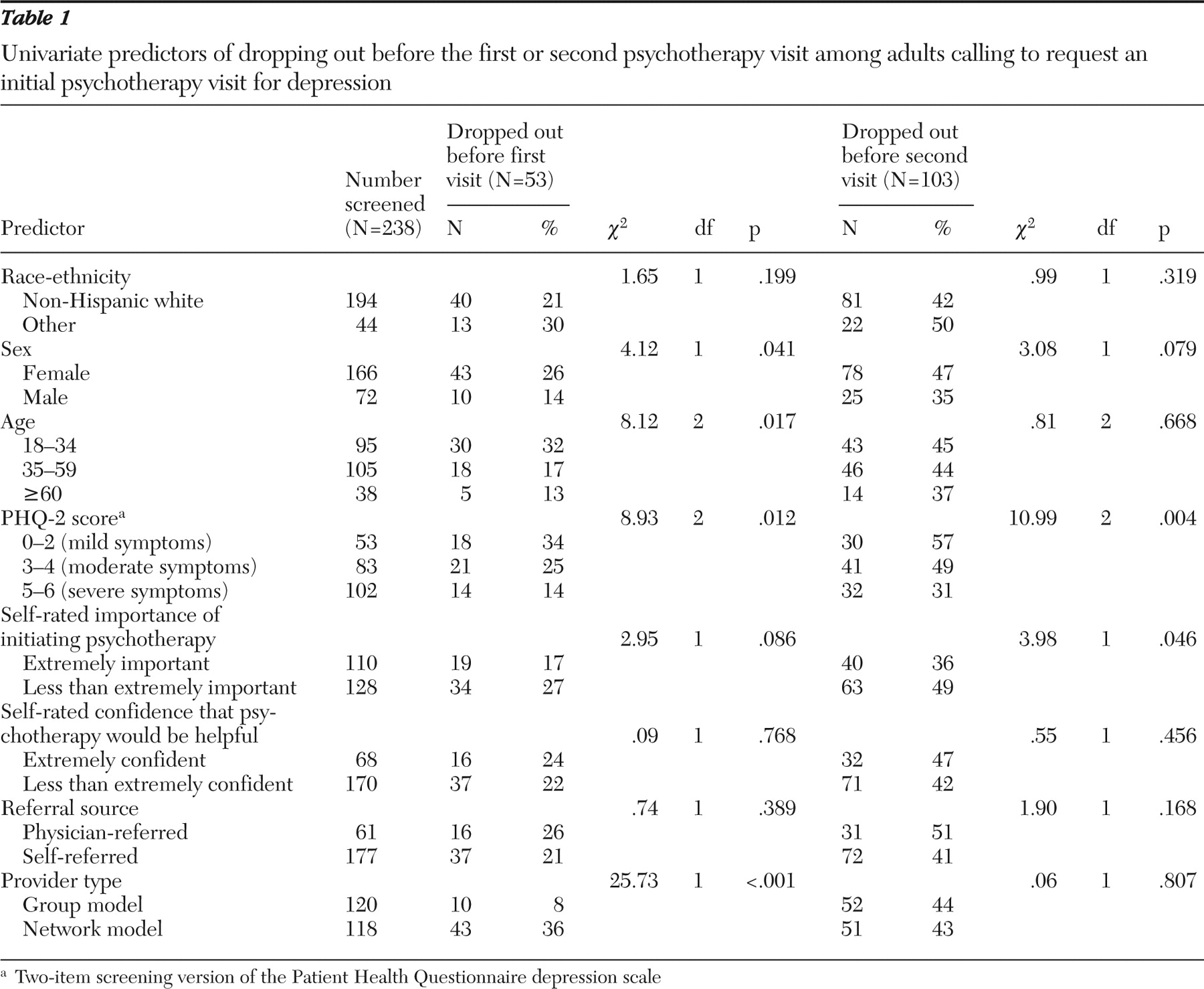
Over the 90 days after the screening call, 53 (22%) dropped out before the first visit, 50 (21%) attended only one visit, 36 (15%) had two visits, 29 (12%) had three visits, 21 (9%) went to four visits, and 49 (21%) went to five or more visits.
Table 1 displays the proportion of participants dropping out before the first visit and the proportion dropping out before the second visit according to various predictors. Dropout before the first visit was significantly related to younger age, female sex, and lower PHQ-2 scores at time of screening. Dropout before the first visit was most strongly related to provider type (only 8% of callers referred to group-model providers dropped out compared with 36% of those referred to network-model providers). Probability of dropping out before the second visit was significantly related to lower PHQ-2 scores and lower self-rated importance of starting therapy.
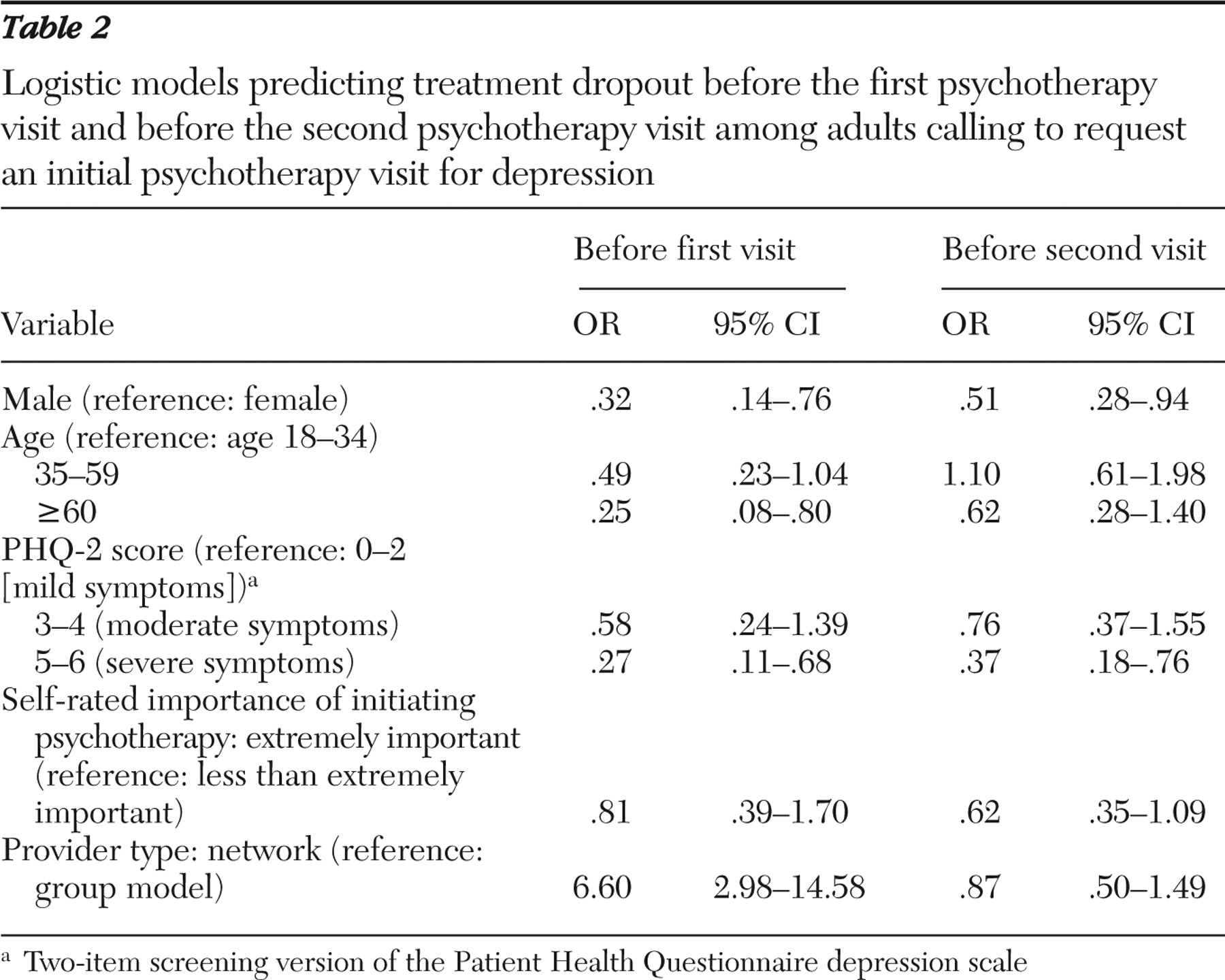
Two logistic regression models were used to examine the joint effects of demographic characteristics, clinical characteristics, and health system factors on likelihood of dropout before the first or second visit (
Table 2 ). Predictors in each model included age, sex, race-ethnicity, and clinical or health system characteristics were found to be marginally significant (p<.10) in univariate analyses. Probability of dropout before the initial visit was significantly related to younger age, female sex, lower PHQ-2 scores, and referral to a network-model therapist. The cumulative probability of dropout before the second visit was somewhat lower among men and much lower among those with more severe depression at screening.
Secondary analyses examined possible interactions between the two strongest predictors of attendance, severity of depression and provider type.
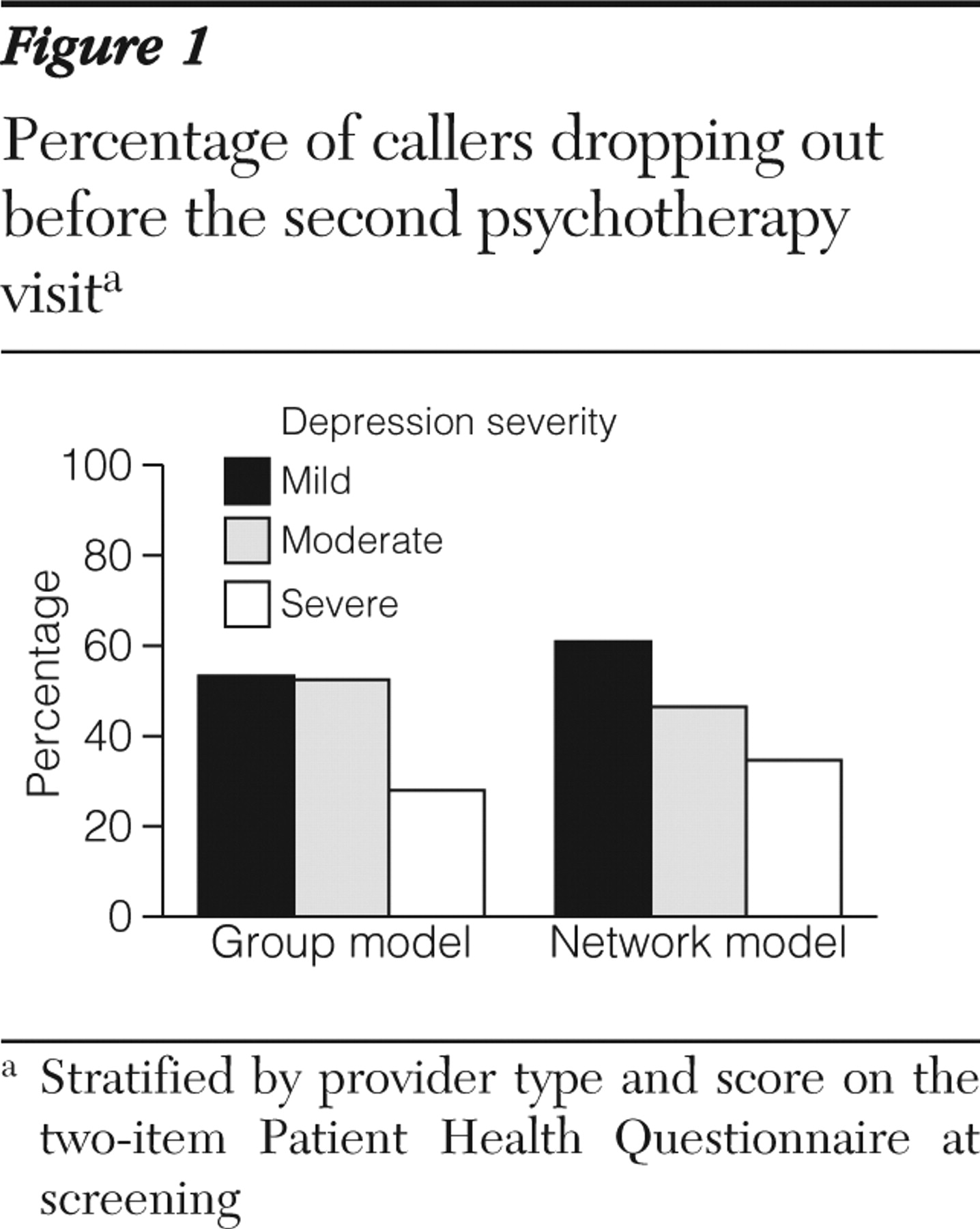
Figure 1 displays the proportion of callers dropping out before the second visit according to provider type and severity of depression score at screening. For both group- and network-model practice, probability of dropout before the second visit was lower among those with more severe depression, and the strength of this association appeared generally similar for the two types of providers. This impression was confirmed in a logistic regression model predicting probability of dropout before the second visit as function of provider type, depression severity at screening, and the interaction of the two (Wald test for interaction effect=.969, df=2, p=.62).
Because attendance differed markedly between callers referred to group- and network-model providers, additional analyses described visit patterns in these two categories. The mean number of visits over 90 days was 2.2±1.5 among those referred to group-model providers, compared with 2.3±2.1 for those referred to network-model providers. When the sample was restricted to those making at least one visit, however, the mean visit count was 2.4±1.4 among those referred to group-model providers and 3.7±1.4 for those referred to network-model providers. Among the 118 callers referred to group-model providers, 43 attended only a single visit, accounting for 36% of all callers and 17% of all visits provided to this group. Among the 120 callers referred to network-model providers, ten attended only a single visit, accounting for only 8% of all callers and only 3% of all visits.
Discussion
Among insured adults calling to request an initial psychotherapy visit for depression, 22% did not attend a single visit over the following 90 days. Dropout before the first visit was significantly associated with being younger, being female, having less severe symptoms of depression, and being referred to a network-model therapist (compared with a group-model therapist). Only 57% attended two or more visits, and dropout before the second visit was significantly associated with less severe depression at the time of the screening telephone call.
In our sample, demographic characteristics were modestly related to dropout. Male sex was significantly associated with a lower rate of dropout before the first or second visit, and older age was significantly associated with a lower rate of dropout before the first visit. Probability of dropout was slightly higher among callers from minority racial or ethnic groups, but this association was not statistically significant (possibly reflecting reduced statistical power because of the relatively small proportion of callers from minority racial or ethnic groups). The direction of each of these relationships, however, was consistent with previous research (
17,
18,
19,
20,
21,
25 ).
Dropout was strongly related to severity of depression at the time of the screening call. This finding is not consistent with the one previous study examining this relationship (
16 ), but our sample included a larger proportion of callers with moderate or severe symptoms of depression. Because the study by Zivin and colleagues (
16 ) included all callers requesting any type of mental health service, findings may not be comparable to those in our sample of callers requesting psychotherapy for depression.
Our most striking finding was the difference in visit attendance patterns between callers referred to group-model providers and those referred to network-model providers. Probability of dropping out before the first visit was more than four times as high for callers referred to network-model providers, and this was not accounted for by any confounding factors that we were able to measure. This difference may be explained by unmeasured differences between these groups of callers. For instance, callers from rural areas were more likely to be referred to network-model providers. We believe, however, that this striking difference in attendance is more likely due to the distinct difference in care processes. Callers referred to group-model providers were offered specific appointments, whereas those referred to network-model providers faced several additional steps before receiving a specific appointment.
Those additional steps may be significant barriers for persons with depression. The marked difference in dropout rates before the first visit was almost exactly balanced by higher dropout after the first visit for group-model providers. Several explanations for this difference seem plausible. Members referred to group-model providers may be less satisfied with the initial visit or may have more difficulty scheduling a second visit at a convenient time. Or this difference may simply reflect a selection effect: members with lower motivation for treatment face higher barriers to an initial visit with network-model providers, so they drop out before the first visit. And the same less-motivated members referred to group-model providers might drop out after the first visit. Ongoing research will examine these alternative explanations. For the time being, any comparison of treatment quality, costs, or outcomes for group-model and network-model psychotherapists should consider the population seeking services rather than the smaller population attending an initial visit.
Closer inspection of visit patterns for group-model and network-model providers indicated markedly different patterns of resource allocation in these two models of care. When we considered all members calling to request psychotherapy, the mean number of visits per caller was approximately equal for group- and network-model providers. But when we considered only those attending an initial visit, the mean number of visits provided was approximately 50% higher for network-model providers than for group-model providers. Among group-model providers, 17% of all visits were by members making only one therapy visit, compared with only 3% of visits for network-model providers. Despite these marked differences in service delivery, group and network models of care had similar proportions of callers attending a second therapy visit and similar relationships between attending a second visit and severity of depression at screening. Our data did not allow us to determine whether these different care models led to differences in clinical outcomes or satisfaction with treatment.
We believe that these findings would likely generalize to psychotherapy provided through other large managed care health systems. The Group Health membership is generally representative of people covered by managed mental health systems, including persons enrolled through Medicare, Medicaid, and state-subsidized programs. The telephone screening process described above is similar to those in most managed care systems. Rates of dropout before and after the initial therapy visit are similar to those in the limited data available from other settings. Our findings regarding demographic predictors of dropout are similar to those in earlier research. We are not aware of any previous research examining differences between group-model and network-model mental health providers. The proportion of services provided by group-model therapists in this sample is higher than in most managed care systems.
We should, however, acknowledge some important limitations of these data. Only 75% of those eligible agreed to participate in the research, and screening staff may not have offered participation to all eligible callers. We do know, however, that demographic characteristics and visit patterns of participants in this study are similar to those in the entire population of interest. This sample size does not allow us to accurately detect relatively weak predictors of visit attendance. For example, the 12% difference between men and women in attendance at the second visit was not statistically significant in this sample. We have no data regarding the type of quality of psychotherapy provided. Therapists' training, theoretical orientation and alliance-building skills may have differed significantly between group- and network-model therapists. We should add that persons with depression may experience barriers to seeking treatment, and our data considered only those who actually called to request services. Most important, we lack data on changes in depression severity necessary to evaluate the clinical importance of early dropout. Some callers may have experienced enough improvement that early dropout might be appropriate.
Conclusions
Our findings offer some reassurance regarding early dropout from psychotherapy for depression. Dropout before the second visit was clearly lower among those with severe depression at time of screening than among those with mild symptoms (31% versus 57%). Still, nearly one-third of those with severe depression dropped out before the second visit, and this group represented one-eighth of all callers. This group should be a priority target for outreach and quality improvement.
Acknowledgments and disclosures
The authors report no competing interests.