Federal law prohibits prison inmates from enrolling in Medicaid while they are incarcerated. Consequently, many inmates with mental illness, including those with serious mental illness, leave correctional facilities without health insurance and therefore without financial access to the treatment they need to live successfully in their communities (
1,
2). They may be eligible for Medicaid on the basis of their disability or other factors, but complex rules and complicated application procedures for both Medicaid and federal disability benefits create barriers to Medicaid enrollment at discharge. In states (such as Oklahoma) where Supplemental Security Income recipients are not automatically eligible for Medicaid, people with serious mental illness may find obtaining coverage particularly challenging.
Reducing barriers to Medicaid enrollment is likely to increase access to health services and reduce subsequent admissions to prisons, hospitals, or other institutions (
3–
5). Difficulties in obtaining needed medications and mental health services have been associated with high risk of diminished quality of life, increased visits to emergency departments, further criminal behavior, and readmission to prisons, hospitals, or psychiatric institutions (
6–
10).
As in many states, an increasing number of adults with mental illness have entered prisons in Oklahoma. In 2002 approximately 26% (about 5,000 male inmates and 1,000 female inmates) of the 23,000 incarcerated individuals under the jurisdiction of the Department of Corrections had a history of mental illness or had exhibited some form of mental illness (
11). By 2006 the percentage of inmates with a history or current symptoms of mental illnesses had grown to almost 50% (about 11,900 inmates), and the number with current symptoms of serious mental illness reached 6,000 (
12). Staff in Oklahoma's Department of Corrections and the state's mental health agency (Oklahoma Department of Mental Health and Substance Abuse Services) believed that a large percentage of inmates potentially eligible for Medicaid were being released without any health insurance and consequently were unable to obtain the mental health treatment they needed as they reentered their communities. Although state officials were unable to stratify historical data by severity of mental illness, they were particularly concerned about inmates discharged with a history of serious symptoms because this group is likely to be at especially high risk of rearrest.
With support from Mathematica Policy Research and the Substance Abuse and Mental Health Services Administration in the U.S. Department of Health and Human Services, a steering committee made up of staff from relevant Oklahoma stakeholder agencies (corrections and the mental health, Medicaid, human services, disability determination, and Social Security agencies) designed and implemented a program to identify inmates with serious mental illness who were eligible for Medicaid and ensure that they were enrolled on the day of discharge or soon thereafter. This article presents the results of an evaluation of the program. Specifically, our study addressed this question: What was the impact of Oklahoma's program for eligible inmates with serious mental illness on their Medicaid enrollment and mental health service use on the day of release and 30, 60, and 90 days after release?
Methods
Oklahoma's discharge planning program
In January 2007, as a result of special appropriations from the Oklahoma state legislature, three discharge managers (one in each of three correctional facilities) were hired by the mental health agency to improve discharge planning for inmates with serious mental illness. As part of their responsibilities, the discharge managers work with other members of the prison mental health treatment teams to ensure that inmates with serious mental illness are enrolled in Medicaid by the time of their release. The discharge managers are especially well suited to bridge the gap between prison teams and community-based services because they are employees of the state mental health agency (and therefore have credibility with community-based providers) but have offices in the Department of Corrections facilities (and therefore have access to clinical information needed to identify the target population and provide them with disability benefit application assistance).
The program involves identifying inmates with serious mental illness who are likely to be eligible for Medicaid and obtaining their signed consent for application assistance about six to nine months before their release, helping them apply for federal disability benefits four months before their release, and assisting them with subsequent Medicaid applications two months before their release. Program implementation included training staff in application procedures for federal disability benefits and Medicaid as well as extensive interagency collaboration that enabled staff at the correctional facilities and local disability determination, disability benefit, and Medicaid eligibility offices to exchange application information more efficiently and effectively.
Because inmates in state prisons are not eligible for benefits during their incarceration and are typically incarcerated for more than a year, those with Medicaid coverage at entry rarely are able to complete the annual or semiannual Medicaid redetermination process to re-enroll before release. Therefore, Oklahoma's program focused on obtaining Medicaid eligibility at discharge instead of on reinstating eligibility for those who had had it at entry. In addition, state officials believed that potentially eligible inmates would need assistance with the application process regardless of their Medicaid enrollment status at entry, and setting up a system for “suspending” Medicaid eligibility would create substantial technical, logistic, and policy problems. Additional details regarding this decision and overall program operations are available elsewhere (
13).
Eligible population
The target population included adults aged 18 or older who met specific diagnostic and service needs criteria as indicated by a C1 mental health service classification in Oklahoma's correctional system (
11). Inmates who met these criteria had been diagnosed as having major depression, bipolar disorder, or a psychotic illness and had been identified as requiring intensive treatment, but not 24-hour monitoring, to adjust to incarceration. Many had a history of repeated stays in prison or inpatient treatment settings or were at high risk of rearrest and reincarceration. Inmates meeting these criteria who were released from one of the three correctional facilities in Oklahoma between July 1, 2007, and March 31, 2008, were identified as eligible for program services.
The three correctional facilities that hosted the program were the Joseph Harp Correctional Center (a 1,400-bed medium-security facility for men, with designated units for inmates with mental illness), the Mabel Bassett Correctional Center (a 1,000-bed maximum-security facility for women with units for inmates with mental illness), and the Oklahoma State Penitentiary (a 2,000-bed maximum-security prison with a mental health unit). These facilities contain three of the largest Department of Corrections mental health units in the state and represent almost a quarter (23%) of all inmates in Oklahoma correctional facilities and about 36% of the state's inmates with serious mental illness.
Seventy-seven individuals in the three hosting prisons were identified as eligible for the program, although 23 (30%) did not receive program services for various reasons. For example, they were discharged earlier than anticipated or refused to participate.
Evaluation design
The evaluation of program effects was based on repeated cross-sectional data and a comparison group design that enabled us to calculate a difference-in-difference estimate of the effect of the program on each outcome. The design strategy enabled us to compare outcomes for inmates eligible for the program (the treatment group) with outcomes for inmates with the same mental health classification in three comparison groups: inmates released from the same project facilities during the previous three baseline years (2004–2006), those released from other Oklahoma correctional facilities during the project period, and those released from other Oklahoma correctional facilities during the previous three baseline years. The treatment group included all inmates eligible for the program, whether or not they received program services. Because the program focused on inmates with serious mental illness and high service needs as determined by the Department of Corrections, the results of the analysis cannot be generalized to all inmates with mental illness.
Outcome variables and analytic approach
The analysis assessed the effects of the program on the likelihood that inmates enrolled in Medicaid and then used Medicaid mental health services on the day of release and within 30, 60, and 90 days of release. The difference-in-difference estimates measure the difference between the change in average predicted outcomes between baseline and the program period for the three project facilities and a similar measure of the change in outcomes for other Oklahoma correctional facilities. Standard errors were computed with the delta method (Stata “inteff” command) (
14). This approach to assessing program effects assumed that changes in Medicaid enrollment and Medicaid mental health service use over time would have been the same for inmates in the project facilities and those in the comparison group facilities had the program not been implemented. The analyses controlled for age, race and ethnicity, gender, education level, Medicaid status at entry, and length of incarceration.
Source of data
The data used in these analyses were based on administrative records obtained from the state's Department of Corrections, the mental health agency, and the Oklahoma Health Care Authority (the state's Medicaid agency). Oklahoma staff assembled a database of person-level records by combining information from relevant administrative files. Individuals' identifying information was removed, and the deidentified database was provided to us for analysis. The data and data collection procedures were approved by two institutional review boards (one in Oklahoma's mental health agency and another independent one).
Results
Sample characteristics
Seventy-seven inmates were in the treatment group; the size of the comparison groups ranged from 130 to 284 (
Table 1). More than 70% of inmates in each of the four groups were under age 45 at release, a majority were white, and most were male. Inmates with a serious mental illness typically scored in the 0–5.9 range on the Test of Adult Basic Education (TABE), indicating that they had only basic literacy skills. Most had prior or current felony convictions, and a quarter or more had violent felony convictions. More than 70% were incarcerated for less than five years.
Compared with inmates released from the comparison group facilities, inmates from the three project facilities tended to have lower TABE scores and a lower rate of prior felony convictions. They also had longer incarcerations—26% were incarcerated for five years or more, compared with about 20% of inmates released from nonproject facilities during the baseline and project periods. Furthermore, 9% of inmates in the targeted population during the project period were enrolled in Medicaid at entry, compared with only 3%–6% in the comparison groups. Because education level, length of incarceration, and Medicaid enrollment before incarceration were associated with the study outcomes, we controlled for these factors in our estimates of program effects. We present both unadjusted outcomes (rates of Medicaid enrollment for each subgroup) and regression-adjusted estimates of program effects.
Although inmates released from project facilities were more likely than other inmates to be enrolled in a Reentry Intensive Care Coordination Team (RICCT) program, RICCT enrollment was not associated with subsequent Medicaid enrollment after analyses controlled for other variables and was not included in our final model. The RICCT program, which was expanded during the same period, had broader program goals that included finding housing and income supports for clients. Helping participants find such services may have been prioritized over Medicaid enrollment by RICCT.
Effects on Medicaid enrollment and mental health service use
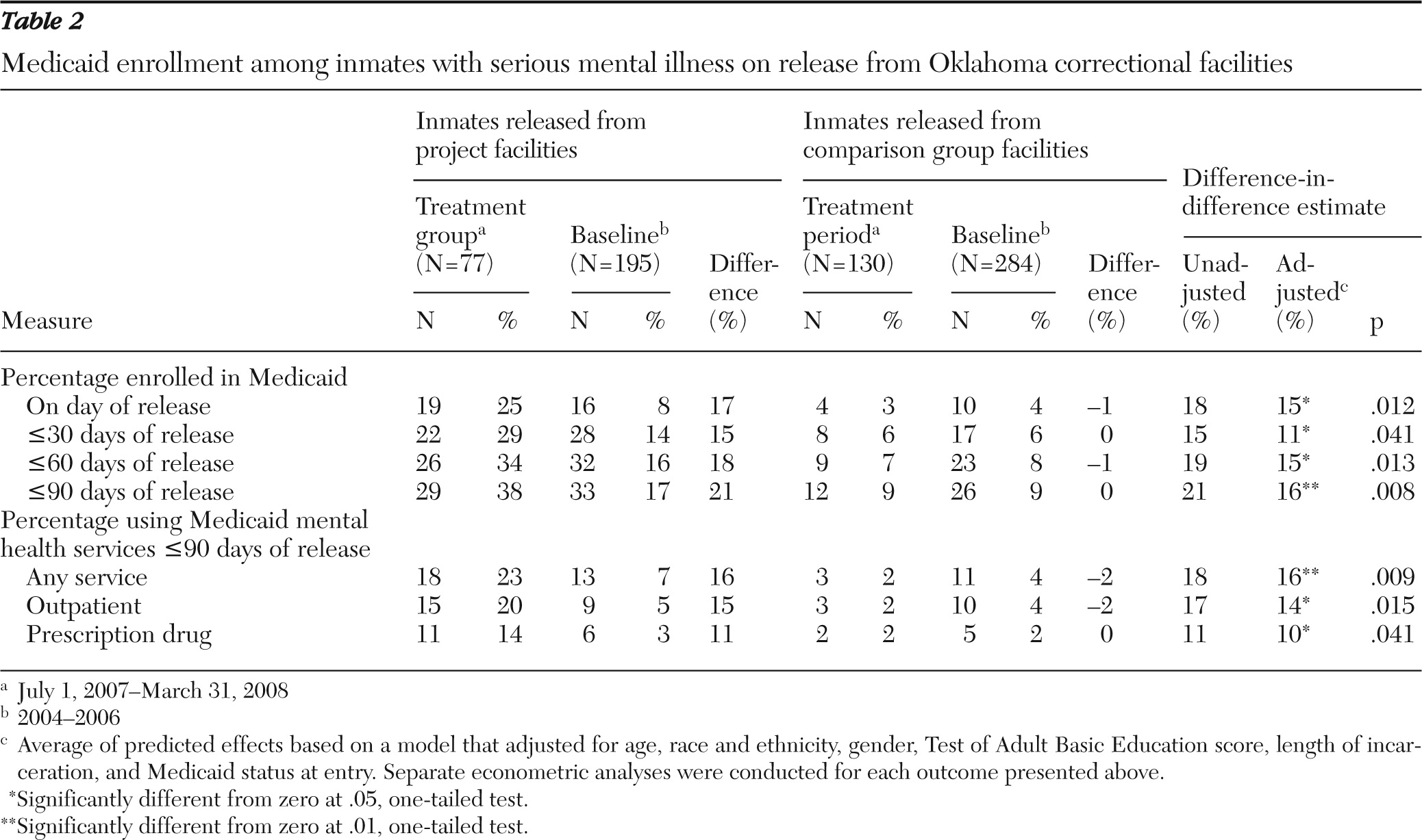
The program had significant positive effects on Medicaid enrollment of inmates with serious mental illness released from Oklahoma prisons (
Table 2). On the day of release, 25% of inmates who received program services were enrolled in Medicaid, compared with 8% of inmates at the same facilities in the two years before the implementation of the new program and 4% at baseline and 3% during the project period for inmates in comparison facilities. After adjustment for Medicaid enrollment at entry and other variables, the analyses indicated that the program increased Medicaid enrollment among eligible inmates on the day of release by 15 percentage points (p=.012). The measured effect within 90 days of release was slightly higher, at 16 percentage points (p=.008), suggesting that the effects of the program extended for at least three months after release from prison.
Although our overall estimated effects are significant, subgroup analyses suggest that the effects of the program on Medicaid enrollment strengthened as the program matured. Among the group of inmates released during the last three months of the intervention, the program effect on enrollment in Medicaid on the day of release was 28 percentage points (p=.028), almost double the effect estimated for the full project period (data not shown).
The increase in Medicaid enrollment associated with the program was paired with an increase in use of Medicaid mental health services. The program was associated with a 16-point increase in use of any Medicaid-financed service within 90 days of release (p=.009), including a 14-point increase in outpatient service use (p=.015) and a 10-point increase in Medicaid prescription drug use (p=.041). That is, the program not only increased the likelihood of obtaining Medicaid coverage on release, but people eligible for program services were also more likely to obtain Medicaid-covered mental health care.
Robustness testing
We tested the robustness of our findings by applying the same model to preintervention data, assuming that the program had been implemented in the three facilities in 2006. The estimated effects were expected to be zero, and indeed, the estimates indicated no effect (.02 percentage points) on Medicaid enrollment on the day of discharge. Additional tests excluded inmates who were known to have transferred between facilities in the year before release to ensure that our findings were not affected by changes in the distribution of inmates across facilities. The estimated effect of the program remained significant at 17 percentage points (p=.017). We also compared our results with those of propensity score matching methods that compared program participants with a matched comparison group of inmates from other facilities released during the project period. The approach produced significant and somewhat higher program effect estimates (23 percentage points; confidence interval 8–39 with nearest-neighbor matching). However, these estimates were sensitive to the selected matching algorithm and did not control for preprogram differences between the treatment and comparison groups. Finally, to better control for gender and other differences across facilities, we used difference-in-difference methods to estimate the program's effect for a subgroup of 383 male inmates released from a treatment facility or one of seven matched comparison facilities. The estimated effect of the program on Medicaid enrollment on the day of release was 14 percentage points (p=.042), similar to the 15-point estimate produced by our original specification.
Discussion
Although people with serious mental illness leaving correctional facilities have urgent and diverse needs for health care, they may not have the skills to independently negotiate the complex steps necessary to complete the Medicaid enrollment process, especially if an individual must first apply for federal disability benefits. Most community providers of mental health services do not have the specialized knowledge or the time needed to assist populations with a history of incarceration, help this population navigate complex application processes, or work closely with prison-based treatment teams. It is important for institutions, to the extent possible, to facilitate these inmates' access to treatment before discharge because potential delays in receiving mental health services can have costly consequences, such as increased probability of relapse, recidivism, or admission to psychiatric facilities (
6–
10).
This study demonstrated that when assistance in gaining access to Medicaid coverage was provided to a group of inmates with serious mental illness before their release from state prisons, the proportion who subsequently enrolled in Medicaid increased significantly. We also found corresponding increases in their use of Medicaid mental health treatment services and prescription medications. Although further research is needed to determine whether the program has significant effects on overall health service use (including use of services not covered by Medicaid) and other long-term outcomes, previous research suggests that an increase in access to Medicaid among program participants will be associated with lower readmission and recidivism rates (
3–
5).
Several factors limited the measured effectiveness of the program. Because of delays in program startup, staffing constraints, and earlier-than-expected discharges, up to 30% of people eligible for the program did not receive program services. Also, two inmates refused assistance and seven inmates were rearrested within 90 days of release (thereby making Medicaid enrollment unlikely). Nevertheless, by the end of the intervention period, discharge managers had addressed many barriers to program implementation, and the program's effectiveness appeared to be increasing.
Recent statistics on the number of adults with serious mental illness leaving state correctional facilities (where prison terms almost always exceed 12 months) suggest that Oklahoma's program may be helpful to other states experiencing similar problems with ensuring that such inmates have access to health insurance at discharge. The U.S. Department of Justice estimates that 1.3 million individuals with mental illness were in state or federal prisons or local jails in 2005 (
15). At least 100,000 individuals who left correctional facilities in 2004 had a mental illness (
1). Although these studies do not provide information specifically for prison inmates with serious mental illness, many such inmates are likely to be included in these figures.
Health care reform legislation passed in early 2010 may lead to Medicaid expansions that make Medicaid eligibility less dependent on documenting the presence of a disability or otherwise reduce barriers to Medicaid enrollment. However, individuals in state prisons are likely to remain ineligible for Medicaid coverage while incarcerated; therefore, special efforts to enroll eligible inmates at discharge will continue to be needed to ensure that these inmates will have access to the treatments and services that minimize risk of relapse and recidivism. This project provides an example of an effective discharge planning program that may be relevant to other states as they work to address this important challenge.
Conclusions
This study showed that a prison discharge planning program characterized by extensive interagency collaboration and dedicated staff trained in disability benefit and Medicaid application procedures was successful in increasing Medicaid enrollment among people with serious mental illness released from Oklahoma prisons. The study also showed that the program's effectiveness appeared to increase after the first six months of its implementation. Finally, the program not only increased Medicaid enrollment, but inmates with serious mental illness and eligible for program services were also more likely to obtain Medicaid-covered mental health care, including prescription drugs.
Acknowledgments and disclosures
This research was conducted under contract with the Substance Abuse and Mental Health Services Administration (SAMHSA) of the U.S. Department of Health and Human Services as part of a larger collaboration with Oklahoma to develop, implement, and evaluate a program to ensure that eligible individuals with mental illness were enrolled in Medicaid at discharge from state institutions. Special thanks go to the project's advisor, Jeff Buck, Ph.D., at SAMHSA. The authors also thank the project's steering committee members for their assistance in developing the program and their advice on the design for its evaluation. For assistance in the collection of administrative data, particular thanks go to Phyllis Abbot, M.S., Ray Bottger, Jin-Song Chen, Ph.D., Tracy Leeper, M.A., Randy May, L.P.C., and David Wright, Ph.D., at the Oklahoma Department of Mental Health and Substance Abuse Services and Mike Connelly, Ph.D., and Courtney Charish, M.A., at the Oklahoma Department of Corrections. Insightful comments by Margo Rosenbach, Ph.D., and Matthew Hodges, M.P.P., on drafts of this article are gratefully acknowledged.
The authors report no competing interests.