Despite the existence of effective, research-supported treatments for adults with severe mental illness, these practices are rarely implemented and sustained in real-world settings (
1). Over the past several decades, research has identified a number of interventions that can provide significant symptom relief and improve overall functioning (
2,
3). All too often effective medication and psychosocial treatment options do not find their way to those who could benefit from them. Although our knowledge of best practices for individuals with serious mental health problems is impressive and continues to grow, our understanding of how to promote the widespread adoption of new practices that are sustainable over time lags far behind (
4).
The challenges faced by mental health systems to implement, sustain, and spread high-quality practices are numerous and daunting. Challenges include staff turnover, demands on workforce competencies, inadequate clinical supervision, fiscal viability, real or imagined risks associated with change, competing role demands, and a lack of accessible and practical resources (
5,
6). The past decade has witnessed an increase in efforts to address a number of these challenges and explore strategies to bring recovery-oriented best practices to the field. One example is the National Implementing Evidence-Based Practices Project sponsored by the Substance Abuse and Mental Health Services Administration (SAMHSA). The project began in 2001 with eight states, including New York State (
7).
The New York State experience
From 2002 to 2005, the New York State (NYS) Office of Mental Health (OMH) participated in the national SAMHSA pilot initiative to study the impact of a specific implementation strategy for promoting the adoption of best practices. This strategy involved the use of consultant-trainers and resource kit materials. One of the best practices selected by OMH to pilot in NYS was illness management and recovery (IMR) (
8). IMR is a curriculum-based treatment using research-informed psychosocial approaches that help adults to manage serious mental health problems successfully and make progress toward specific goals.
NYS implemented IMR in three community agencies and a mental health unit in a prison in the New York City metropolitan area. As these sites implemented IMR, the consultant-trainers observed the implementation process and gathered feedback from practitioners, consumers, and program leaders. Overall, stakeholders reported that IMR added value to the quality of services. Administrators and staff commented that the structured materials and handouts, along with a manual that emphasizes core clinical competencies, was a useful resource. Feedback also suggested ways in which IMR could be expanded and adapted to increase its widespread usability and sustainability, especially when delivered in groups. Although IMR may be employed in a group modality, it was primarily designed to be used in individual sessions. The importance of adapting IMR for group work was based on two considerations: the recognized benefits of group treatment and peer learning for people with serious mental health problems and the fact that group treatment is a mainstay for most mental health programs in NYS.
The consultant-trainers engaged a NYS-operated facility (Hudson River Psychiatric Center) and ten member agencies of the Urban Institute for Behavioral Health, a consortium of New York City providers committed to implementing evidence-based practices, to explore field testing and evaluating adaptations of IMR that were based on our observations and stakeholder experiences. This process led to adaptations in the IMR program and ultimately to a new name: Wellness Self-Management (WSM) (
9). [An expanded description of the WSM program is available in an online supplement to this column at
ps.psychiatryonline.org.]
WSM and IMR: similarities and differences
WSM has much in common with IMR, including the use of a structured comprehensive curriculum that addresses recovery, relapse prevention, coping and stress management, social supports, practical facts about mental health problems, medication information, problem solving, and personal goal development. WSM and IMR both place an emphasis on assisting participants to apply their learning in vivo. Both approaches reflect recovery-oriented values and principles involving self-direction, choice, and shared decision making.
WSM departs from IMR in several ways: the entire curriculum is organized into a workbook that belongs to the participants, a physical health chapter was added, self-directed action steps are used, the process is organized around a specific group facilitation format, and core competencies are embedded within the workbook. These adaptations were designed to facilitate use of the curriculum in a group modality and promote widespread implementation and sustainability of these services across NYS. [An expanded description of the differences between WSM and IMR is available in the online supplement at
ps.psychiatryonline.org.]
Methods to promote widespread use of WSM
After a yearlong field test of the WSM workbook and group format (July 2006–September 2007), OMH funded the Center for Practice Innovations at Columbia Psychiatry under the leadership of Susan Essock, Ph.D., director of the Division of Mental Health Services and Policy Research. The center designed a statewide effort to promote adoption and sustained use of WSM. The center employed a formal learning collaborative methodology that is based on the quality improvement approach of the Institute for Healthcare Improvement (
10). A total of 105 mental health service agencies voluntarily joined this effort and all except government-run programs contributed $500 each toward the purchase of WSM workbooks, which cost approximately $10 each. The range of programs involved is extensive and includes virtually every type of mental health treatment setting, including mental health units located in prisons. WSM workbooks were also translated into Spanish, Chinese, and Korean to accommodate programs serving these populations.
All agencies agreed to implement WSM and report data related to key performance indicators, including attendance, discontinuation and reasons why, client self-assessment of progress, and group leader ratings of each participant's degree of involvement and goal progress. Data were reported for the period April 2008 to March 2010. In addition, practice fidelity was determined in two ways: ratings of WSM group leaders by supervisors and ratings by an independent research assistant. [An expanded description of practice fidelity and measurement methods is available in the online supplement at
ps.psychiatryonline.org.]
Evaluation
Findings for the period evaluated indicated that the 212 WSM groups were well attended and that the most common reason for participants to discontinue was discharge from the agency. Group leaders generally implemented the group with fidelity. Across the state, the median fidelity rating provided by program supervisors was 50 out of a possible total score of 58. With a sample of the WSM programs, we also used a separate independent fidelity measure that focused on group skills. These ratings (median score of 18 out of a maximum score of 24) further indicated that most practitioners employed the workbook and group format at a satisfactory level.
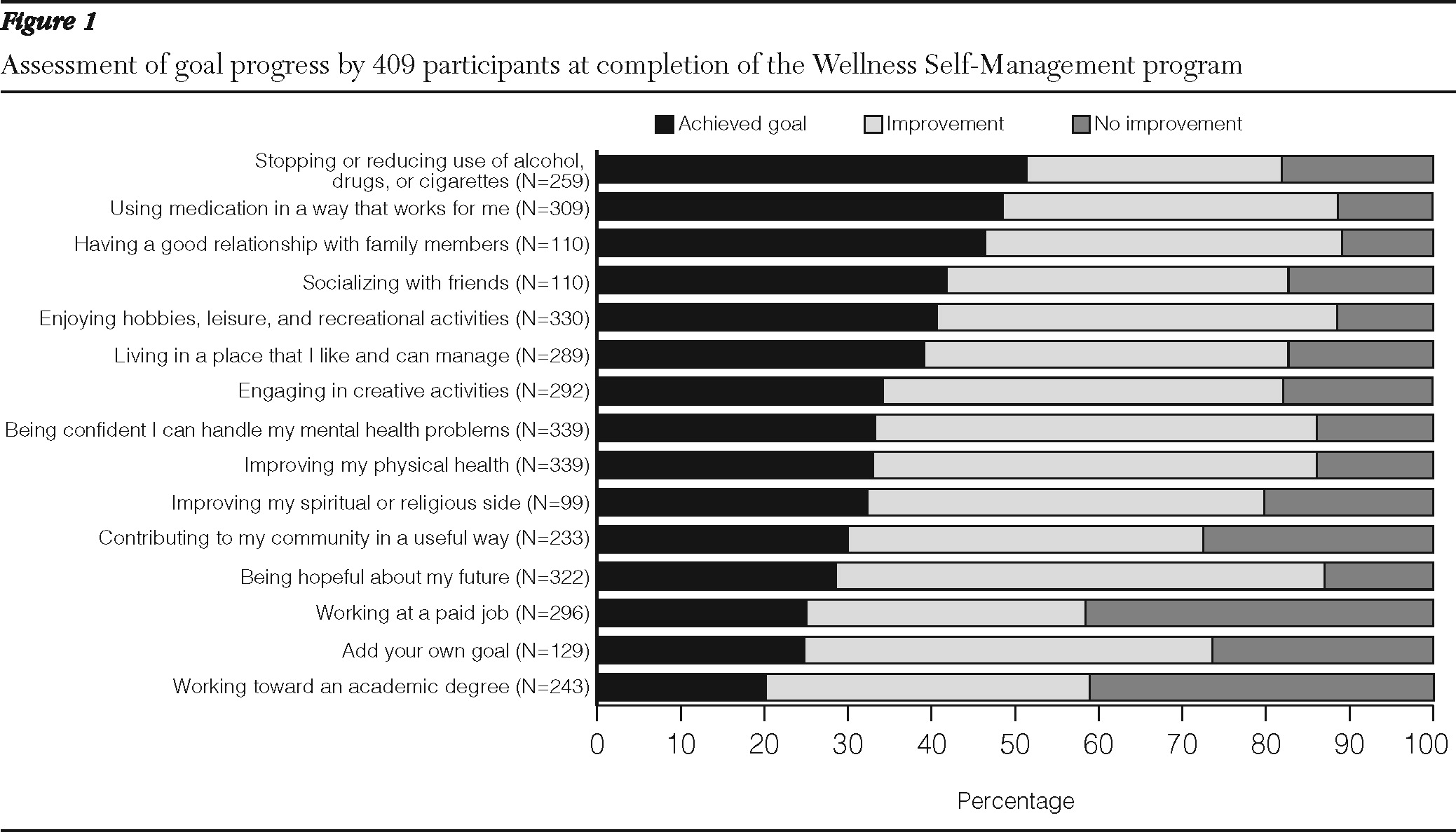
At the beginning of the group, participants identified personally meaningful goals. At program completion, participants rated their progress in terms of how well they improved or attained their goals (
Figure 1). Reports from 409 participants and their group leaders indicated that 75% of participants demonstrated significant progress with respect to their identified goal areas over the course of the program.
An important part of this initiative was to determine the sustainability of WSM after conclusion of the formal learning collaborative in October 2009. A survey conducted ten months later garnered responses from 87 of the original 105 participating agencies. The responses indicated that 85% continued to provide WSM groups; 13% described plans to offer WSM in the near future, and only one program reported difficulty sustaining WSM (because of serious client transportation problems).
Empowering agencies to sustain WSM on their own was accomplished by creating inexpensive and easily accessible staff training resources, such as a free online course on how to conduct a WSM group program, promotional and training DVDs, downloadable workbooks, group leader training guides, and informational brochures. The positive response of agencies to the WSM initiative has also resulted in numerous requests from providers for additional curriculum-based resources addressing the needs of adolescents and young adults, adults with co-occurring substance use disorders, and prison inmates with mental illness. Several initiatives are currently under way to field test WSM-related workbooks designed to address the needs of these three populations. We expect to report on the outcomes of these efforts in the coming year.
The Center for Practice Innovations Web site at
www.practiceinnovations.org provides interested practitioners, programs, or agencies the information, tools, and resources needed to successfully implement WSM in groups.
Conclusions
New York's statewide initiative built upon and reflected the core principles of a recognized best practice while making adaptations and creating tools and resources in response to multistakeholder feedback that promote widespread adoption and sustained use of this practice. New York's aim is to go beyond the initial implementation phase and design strategies to empower organizations to sustain and spread a practice that adds value to the mental health system and is applicable across clinical conditions, cultural populations, and program types. Developing and evaluating user-informed adaptations, along with the creation of easily accessible tools and resources, may point the way to closing the research-to-services gap.
Acknowledgments and disclosures
The WSM initiative was primarily funded by the New York State Office of Mental Health. The Urban Institute for Behavioral Health (UIBH) was an instrumental partner in this initiative by identifying and engaging the ten agencies involved in the initial pilot project and involving the UIBH director Andrew Cleek, Psy.D., as a coauthor of the WSM workbook.
The authors report no competing interests.