With recognition of the schism between expectations placed on law enforcement officers and the minimal training they typically receive for dealing with psychiatric crises, the crisis intervention team (CIT) program was developed in Memphis, Tennessee, in 1988 (
1). CIT has since been recognized as an exemplary collaboration between local mental health professionals, police officers, and advocacy groups (
2–
4). This program provides officers 40 hours of specialized training consisting of classroom lectures, visits to local mental health services, and performance-based exercises for mastery of deescalation techniques (
5). However, it is increasingly noted that the CIT model is “more than just training” (
2), meaning that other aspects of the CIT model—in addition to the curriculum—must be in place for communities to benefit from embracing the model. As stated in the Core Elements published by national leaders of CIT, the model comprises ongoing elements (such as partnerships, community ownership, and law enforcement policies and procedures), operational elements (training of officers and dispatchers), and sustaining elements (including evaluation and research, advanced in-service training, and outreach to other communities) that are essential to the program's success (
6). Over 1,200 CIT programs are estimated to be in operation in cities and counties across the United States (personal communication, Dupont R, Oct. 18, 2010).
It has been assumed that self-selection of officers into CIT training is a crucial aspect of the program. As stated in the operational core elements pertaining to the CIT officer (
6), “officers within a patrol division should voluntarily apply for CIT positions.” A number of authors cite self-selection as a key feature of their local programs (
2,
7–
9), and some have proposed the presence of a desired “selection bias,” meaning that officers' attributes predispose them to seeking—and subsequently effectively incorporating into their fieldwork—CIT training (
10–
12). That is, officers who self-select into CIT may be characterologically different from, and better suited than, those who do not volunteer for CIT training, although no previous research has examined this assumption. Furthermore, it has been noted that compared with non-CIT-trained officers, CIT-trained officers are more likely to report having a family history of psychiatric treatment or knowing someone in the mental health profession (
12,
13), which may represent another aspect of the desired “selection bias” for officers opting into the training.
This study was conducted to provide the first empirical examination of several potential “behind the scenes” characteristics involved in volunteering for CIT training. Two key characteristics of interest were empathy and psychological mindedness. The latter can be understood as an individual's capability and interest to be in touch with and reflect on one's range of psychological states (
14). One's aptitude for psychological mindedness tends to be a fairly stable personality characteristic (
14,
15). In relation to CIT training, officers' ability to empathize, along with their awareness of their own psychological state, should make for a successful CIT officer. In addition, in a recent qualitative study, officers suggested that empathy is a character trait needed for success as a CIT officer (
16). The primary hypotheses of this study were that officers entering CIT training—particularly those volunteering for it—would have a higher likelihood of past exposure to and experience with mental health issues and greater empathy and psychological mindedness. A secondary hypothesis was that the four measures of empathy and psychological mindedness represent stable traits (as opposed to changing after CIT training). These hypotheses were tested with data from 177 police officers, 109 of whom were non-CIT officers and 68 of whom were officers entering CIT training (24 via assignment and 44 through volunteering).
Methods
Data were collected in 2009 and 2010 from a sample of police officers attending non-CIT and CIT classes from various counties in Georgia. The non-CIT officers attended training on topics such as sexual assault, domestic violence, and supervision at the Georgia Public Safety Training Center. The officers receiving CIT training were recruited from six municipalities. The assessment was administered twice, on Monday mornings (initial assessment) and Friday afternoons (posttraining assessment). The Emory University Institutional Review Board approved the informed consent forms, which were signed by all participants. The overall self-administered, anonymous survey, embedded with the measures described below, required approximately one hour to complete.
A detailed, self-administered form to capture demographic characteristics was completed by participants at the beginning of the survey. It assessed for important covariates, such as age, gender, and years of service as a police officer, as well as several other basic sociodemographic variables. The question “Are you a crisis intervention team (CIT) officer?” was included to assess the CIT status of officers in the non-CIT group, and 16 officers who identified themselves as CIT officers were excluded from the analyses, resulting in the 109 non-CIT officers whose data are reported herein. For officers who were to receive CIT training, participants were asked how they entered the training program (“volunteered/self-selected” or “was assigned/told to do it”). Four variables, used in prior survey-based research with police officers (
10,
12,
13), assessed the officers' personal history of exposure to and experience with mental health issues. Specifically, officers were asked, “Have any of your family members ever received or are they currently receiving treatment for a mental health problem (such as therapy, counseling, or medicine for mental or emotional problems)?” “Have you known someone within your circle of friends who has been or is currently undergoing treatment for a mental health problem?” “Have you ever received or are you currently receiving treatment for a mental health problem?” and “Have you or any members of your family or any of your friends been active as either a professional or volunteer helper in the field of counseling, therapy, psychiatry, psychology, or social work?”
Empathy was measured with two instruments. First, the Empathy Quotient (EQ) was initially developed as a 60-item measure in which responses are given on a 4-point Likert scale ranging from “strongly agree” to “strongly disagree” (
17). To minimize participant burden, 28 items previously examined in a principal-components analysis—which derived cognitive empathy, emotional reactivity, and social skills factors (
17)—were included in this study. As in the prior report (
17), participants received 0 points for a nonempathic response, whatever the magnitude, and 1 or 2 points for an empathic response; thus, the total score across the 28 items could range from 0 to 56, with higher scores representing more empathic responses. EQ total scores showed good internal consistency, with a Cronbach's alpha of .88 at the initial assessment (
α=.87 for non-CIT officers and
α=.89 for officers receiving CIT training). As noted below, an exploratory analysis also examined cognitive empathy, emotional reactivity, and social skills domains, which include items such as “I can tell if someone is masking their true emotion,” “I tend to get emotionally involved in a friend's problems,” and “I don't tend to find social situations confusing,” respectively.
Second, the empathic concern subscale of the Interpersonal Reactivity Index (IRI-EC) was used to further assess empathy (
18). Responses to the seven self-report items of the IRI-EC are given on a 5-point Likert scale ranging from “does not describe me well” to “describes me very well.” Constructs measured include experiences of feeling warmth, compassion, and concern for others enduring negative experiences. Total scores range from 0 to 28, with higher scores indicating a greater tendency to experience feelings of warmth and concern for others. Sample items include “I would describe myself as a pretty soft-hearted person” and “Other people's misfortunes do not usually disturb me a great deal”; the latter item is reverse-scored. The instrument has acceptable test-retest reliability (
18). The IRI-EC showed moderate internal consistency in the study sample, with a Cronbach's alpha coefficient of .62 at the initial assessment (
α=.57 for non-CIT officers and
α=.66 for officers receiving CIT training), although it should be noted that the subscale has only seven items, and alpha is influenced by the number of items.
Psychological mindedness was also assessed with two measures. First, the Balanced Index of Psychological Mindedness (BIPM) is a self-report measure consisting of 14 items scored on a 5-point Likert scale, with response options ranging from 0, “not true,” to 4, “very much true.” Sample items include “I am often not aware of my feelings” (reverse-scored) and “I am better off when being in touch with my feelings.” The scale comprises “interest” and “insight” subscales, and total scores indicate an average of the two subscale scores. Total BIPM scores can range from 0 to 28; higher scores indicate greater interest and insight and higher psychological mindedness (
14). Internal consistency has been demonstrated in adult community samples and in psychiatric samples (
14), and in this study sample the Cronbach's alpha was .71 at the initial assessment (
α=.69 among non-CIT officers and
α=.71 among officers in the CIT training group).
The second measure of psychological mindedness, the Psychological Mindedness Scale (PMS), measures one's ability to see relations among thoughts, feelings, and actions, with the goal of learning the meanings and causes of experiences and behavior (
19). The PMS is a self-report measure that includes 45 items scored on a 4-point scale, with response options ranging from “strongly disagree” to “strongly agree.” Sample items include: “Usually, if I feel an emotion, I can identify it,” and “I am always curious about the reasons people behave as they do.” Twenty items are reverse-scored, and the total PMS score (ranging 45–180) is the sum of individual item responses, with higher scores indicating greater psychological mindedness. The instrument has good internal consistency in psychiatric (
19) and nonclinical samples (
20). In this study the Cronbach's alpha was .88 at the initial assessment (
α=.86 among non-CIT officers and
α=.89 among officers in the CIT training group).
Basic sociodemographic characteristics of the three groups of officers (also referred to as “officer status”; non-CIT officers, officers assigned to CIT training, and officers who had self-selected into CIT training) were compared. Intercorrelations among the psychological variables of interest were examined with Pearson product-moment correlation coefficients. Associations between officer status and past exposure to or experience with mental health issues or professionals, empathy, and psychological mindedness were examined by using chi square tests of independence and analyses of variance. As necessary, these tests were followed by logistic regression models and analyses of covariance (ANCOVAs) to control for the effects of potential confounding variables. The secondary hypothesis, pertaining to stability of empathy and psychological mindedness, relied on paired-samples t tests. All analyses were conducted with SPSS, version 16.0, and all hypothesis tests were two-tailed with a significance criterion of p<.05.
Results
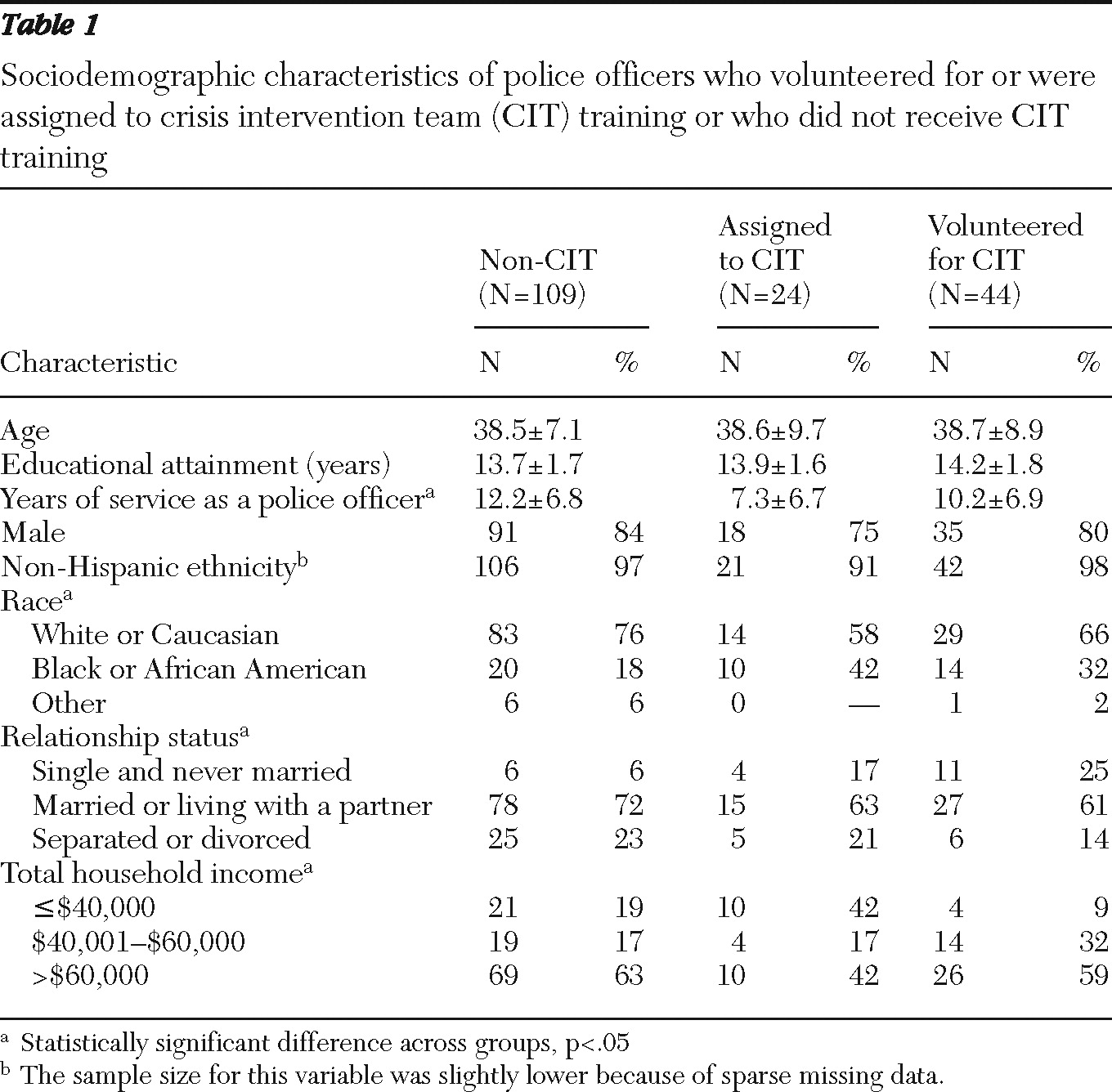
The three groups of officers did not differ with respect to age or years of education (
Table 1). Officers assigned to CIT training had served as a police officer for fewer years than the non-CIT officers (F=5.40, df=2 and 171, p=.005). The three groups did not differ with respect to gender or ethnicity, although when we excluded the “other” race category (because of small samples), non-CIT officers were more likely than those assigned to CIT to be white or Caucasian and were less likely to be black or African American (
χ2=6.36, df=2, p=.04). Furthermore, as shown in
Table 1, there were statistically significant differences in relationship status (
χ2=12.04, df=4, Fisher's exact p=.01) and total household income (
χ2=13.27, df=4, p=.01) across the three groups.
The IRI-EC score was only modestly correlated with BIPM and PMS scores (r=.29 and r=.28, respectively), and it was moderately correlated with EQ scores (r=.43). The EQ score was also moderately correlated with the BIPM score (r=.44). The strongest correlations were between the PMS score and the EQ and BIPM scores (r=.62 and r=.57, respectively). Because high correlations (r>.70) were not observed, subsequent analyses proceeded by considering each of the four empathy and psychological mindedness variables as nonredundant, somewhat separate constructs.
Given that officers in the three groups differed with respect to years of service as a police officer, race, relationship status, and total household income, associations between these four sociodemographic variables and the four empathy and psychological mindedness variables were examined. Whereas race, relationship status, and total household income were not significantly associated with any of the four psychological characteristics, years of service was modestly but significantly (p<.05) inversely correlated with IRI-EC (r=−.17), BIPM (r=−.21), and PMS (r=−.16) scores.
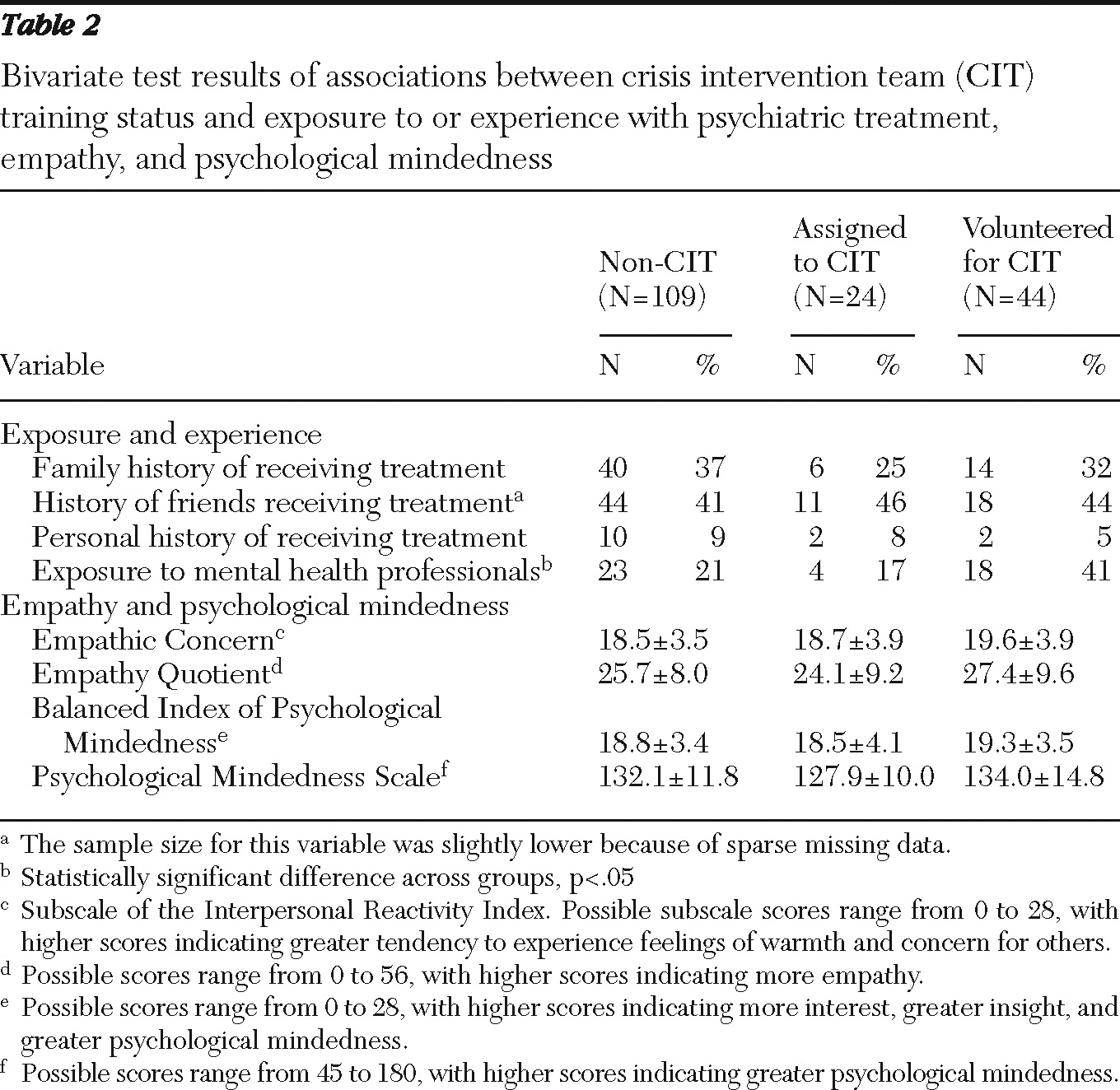
The three groups did not differ with respect to three of the four exposure and experience variables (
Table 2). However, compared with the other officer status groups, a higher proportion of officers who self-selected for CIT training responded affirmatively to the question, “Have you or any members of your family or any of your friends been active as either a professional or volunteer helper in the field of counseling, therapy, psychiatry, psychology, or social work?” Specifically, 41% of the officers who volunteered for CIT training reported this type of exposure to mental health professionals, compared with only 17% of officers assigned to CIT training and 21% of non-CIT officers. This association was obscured (no longer significant) when the two CIT training groups were combined and compared with the non-CIT group.
Exposure to mental health professionals was unrelated to years of service as a police officer, relationship status, and total household income, which ensured that the association was not confounded by these variables. However, race (dichotomized as white or Caucasian race or black or African-American race) was significantly associated with exposure to mental health professionals (60% of white or Caucasian officers compared with 40% of black or African-American officers;
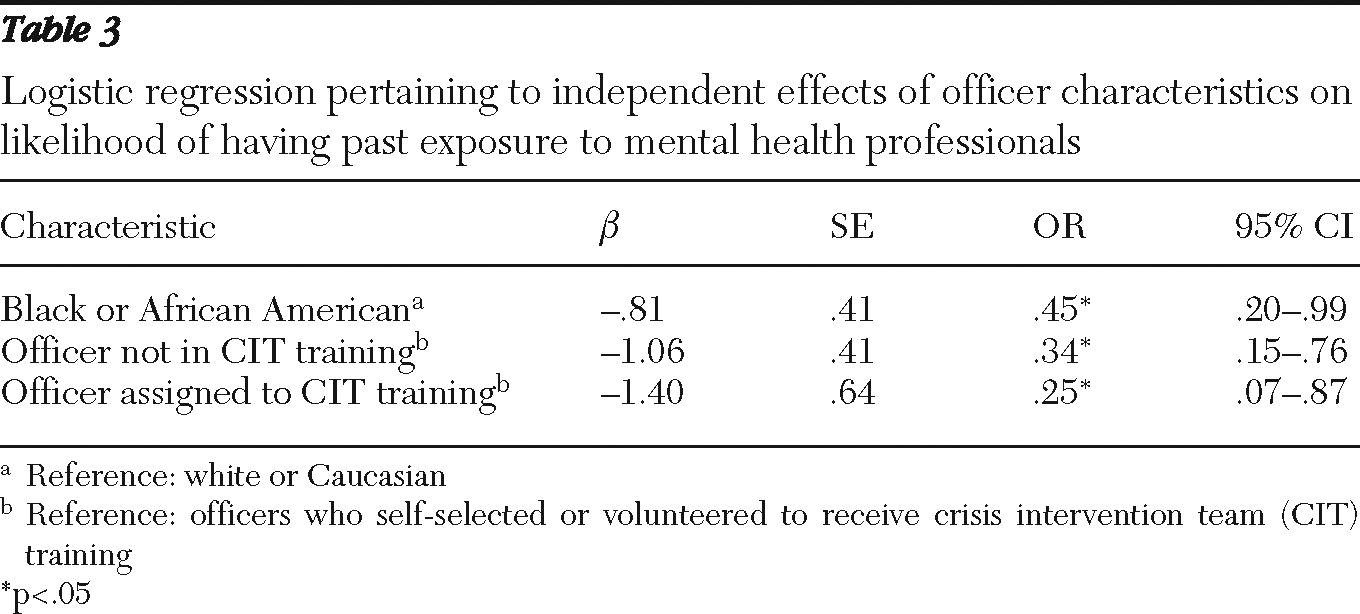
χ2=4.19, df=1, p=.04). Thus, to examine the association of officer status and exposure to mental health professionals while controlling for the effects of race, we used a binary logistic regression model (recoding the three-level officer status variable into two dummy variables). Model results are shown in
Table 3. Being black or African American, being a non-CIT officer, and being assigned to CIT training (relative to volunteering for it) were independently associated with lower odds of having been exposed to mental health professionals.
Although officers volunteering for CIT training had higher scores on all four measures of empathy and psychological mindedness, none of these modest differences were statistically significant. The cognitive empathy, emotional reactivity, and social skills subscales of the EQ also did not differ. The results did not change when the two CIT training groups were combined and compared with non-CIT officers. Because the number of years of police service was significantly inversely correlated with IRI-EC, BIPM, and PMS scores as noted above, we used ANCOVAs to reassess differences in mean scores across the three groups while controlling for the effects of this covariate (to exclude any possible negative confounding). In all three instances, when the effect of years of service as a police officer was removed, the three groups of officers did not differ on empathy or psychological mindedness.
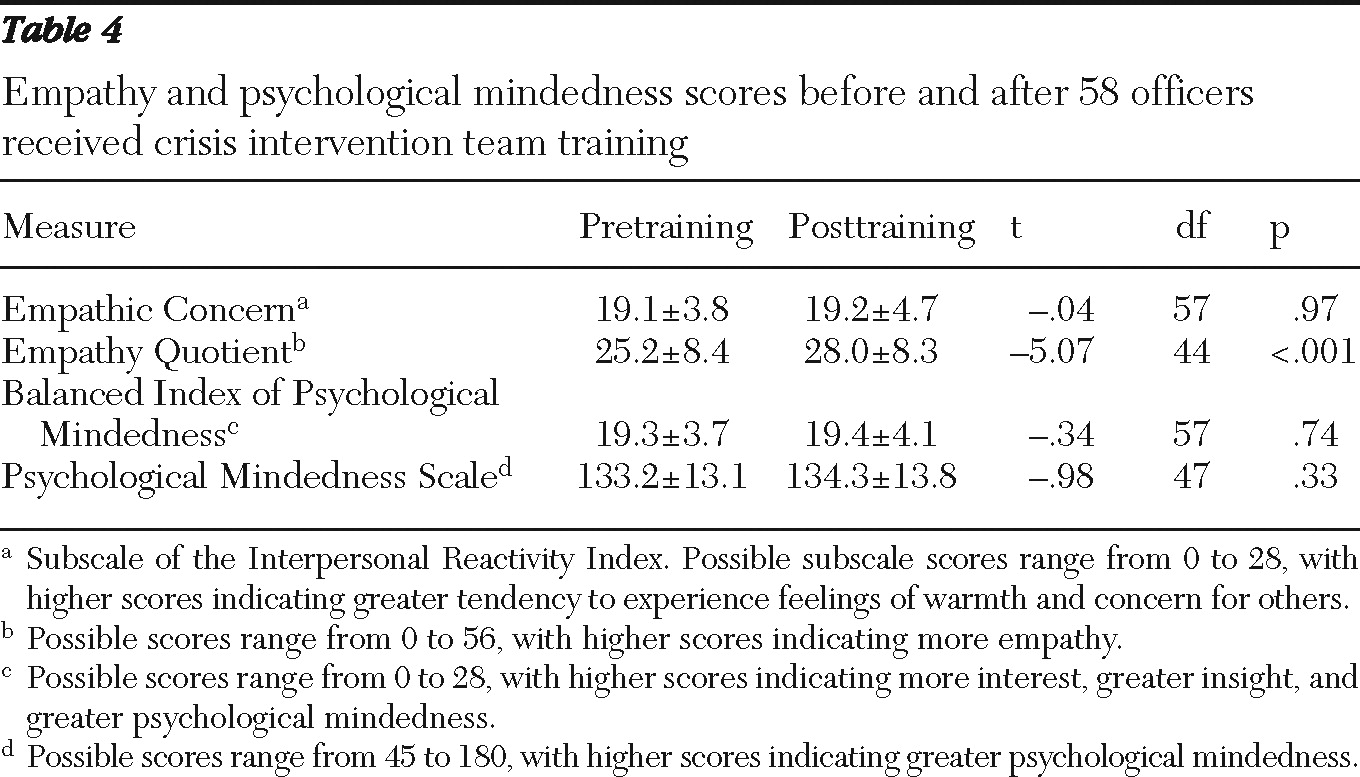
Analyses were then conducted to test the secondary hypothesis that the four measures of empathy and psychological mindedness represent stable traits (as opposed to changing after CIT training). For these analyses, data were available from both the initial assessment and the posttraining assessment of 58 officers participating in CIT training. Two officers who had been assigned to the training did not participate in the posttraining assessment, and one officer who had volunteered did not participate in the posttraining assessment; thus differences in demographic variables among those included and not included in the follow-up assessment could not be evaluated. As shown in
Table 4, values on one measure of empathy (IRI-EC) and both measures of psychological mindedness (BIPM and PMS) did not change after the week-long CIT training course. However, scores on the other measure of empathy (EQ) significantly increased after the training (from 25.2 to 28.0, p<.001). Of note, these findings did not change when data from 22 assigned officers and 36 self-selecting officers were examined separately. In an exploratory analysis, the three subscales of the EQ were then examined; the cognitive empathy and emotional reactivity subscale scores differed significantly after CIT training (p<.001), although the social skills subscale score did not (p=.07).
Data were available from both the initial assessment and posttraining assessment of 59 non-CIT officers. Given that posttraining data could not be collected from 50 non-CIT participants, we examined potential differences between those who did and did not provide follow-up data. The two groups did not differ with respect to age, years of educational attainment, years having served as a police officer, race, gender, ethnicity, relationship status, and income. However, officers who did not complete the posttraining assessment were more likely to indicate that they had a family member who had received or was currently receiving mental health treatment (50% compared with 26%; χ2=6.71, df=1, p=.010) and were more likely to report having known someone within their circle of friends who had been or was currently in mental health treatment (52% compared with 31%; χ2=4.89, df=1, p=.03). However, non-CIT officers from whom posttraining data could not be collected did not differ on the four variables of interest (pertaining to empathy and psychological mindedness) compared with those who completed the posttraining assessment. For the 59 non-CIT officers with available data at both assessments, scores on all four measures remained stable from the initial assessment to the posttraining assessment (for example, EQ scores were 26.0±9.1 and 25.9±9.5, respectively).
Discussion
Several demographic characteristics differed across the three groups of officers, which likely reflects variation in CIT implementation across police departments involved in the study, rather than broadly generalizable differences between officers who do or do not receive CIT training. For example, CIT uptake may differ across municipalities that have different salary structures. Differences in salaries may also be related to differences in years of service. Sociodemographic variables should be assessed in future studies of CIT- and non-CIT-trained officers given that such variables may represent important covariates. With regard to the primary hypotheses, self-selected pre-CIT officers were roughly twice as likely to report having had some exposure to mental health professionals, which remained true even after analyses controlled for a potential confounder, race.
However, contrary to our hypothesis, the three groups did not differ with respect to empathy or psychological mindedness. In terms of the secondary hypothesis, three psychological variables remained stable before and after CIT training (suggesting that they are, in fact, traits), although one measure of empathy did change after CIT training. There may be two reasonable explanations for why scores on that particular empathy measure improved after CIT training. First, several items of the EQ could pertain to some of the active listening and verbal deescalation skills that officers acquire during their CIT training—for example, “I am good at predicting how someone will feel,” “I can sense if I am intruding, even if the other person doesn't tell me,” and “I can easily work out what another person might want to talk about.” Second, because of a larger range of scores, the EQ scale has greater variability than our other measures, which may have allowed changes to be more easily detectable (although differences in the other measures were negligible).
Although many CIT officers in our sample reported volunteering into the CIT training program, others had been assigned to it by their respective department, which deviates from the recommendation that officers should ideally volunteer (
6). This reality, in conjunction with the lack of differences in empathy and psychological mindedness among the three officer groups at baseline, raises questions about the assumption that officers who volunteer for CIT training are inherently more suited for the program. In fact, the lack of differences in these key characterological attributes may support some police departments' practices to train all officers or to assign officers to CIT training on the basis of departmental needs and preferences.
However, the lack of distinction between the three groups of officers in empathy and psychological mindedness does not necessarily negate the merit of the argument that officers volunteering for CIT are in some way more appropriate for the program. In fact, the significant difference in exposure to mental health professionals by group could indicate that volunteering officers are more in tune with CIT's tenet of “responsibility and accountability to consumers of mental health services, their relatives, and the community” (
2). Considering that officers' characteristics are thought to be important determinants of effective CIT implementation (
21), one could argue that these findings justify closer scrutiny of departmental requirements and selection procedures for enrollment into CIT training. Officers who self-selected into CIT training were more likely to report on the survey that they had been exposed to or had experience with mental health professionals, which may be an influential factor in these officers' decision to volunteer for CIT training and may be indicative of their suitability for training.
Several methodological limitations of this study warrant discussion. First, a number of police departments were represented, and sample sizes from the individual departments were too small to allow subanalyses. Second, among the diverse characterological variables that could have been examined, we assessed only the two deemed to be most salient (given that officers' interactions with individuals with mental illnesses would obviously benefit from empathy and psychological mindedness). Before firm conclusions can be drawn in this arena, further research should examine other characteristics of officers, perhaps including conscientiousness and altruism.
Third, given that self-selecting officers had numerically higher scores on the four measures of empathy and psychological mindedness, and in light of the fact that sample sizes in the three groups were modest (N=109, N=24, and N=44), it could be argued that a much larger sample may reveal significant effects. However, given the modest magnitude of these effects (the largest effect was seen in PMS scores between officers assigned to and self-selected for CIT training, with a Cohen's d of .45, representing a small to medium effect, although most effects were much smaller), such differences between groups are unlikely to be practically meaningful in routine interactions between officers and individuals with mental illnesses who are in crisis. Also, measurement limitations could play a role in the findings. Perhaps the empathy most relevant to CIT officers is context or target specific, and a measure of empathy related to persons with mental illnesses would be more appropriate to discern differences between groups.
Fourth, some classes attended by non-CIT officers focused on topics of domestic violence or sexual assault, which may attract officers whose degree of empathy is similar to that of CIT officers. However, these classes did not specifically address mental health, and most non-CIT officers were in a class on supervision—a managerial issue quite distinct from crisis intervention.
Conclusions
Although there may be other justifiable reasons to argue for the importance of volunteering, characterological empathy and psychological mindedness do not appear to be greater among officers self-selecting into CIT. It is noteworthy that empathy (measured with the EQ) significantly improved after CIT training, and to our knowledge, this is the first demonstration of changes in empathy during CIT training, although the magnitude of the effect was small. As research on the very widely disseminated CIT model continues to advance, a greater understanding of the factors that attract certain police officers into CIT training, and the practices of various police departments in selecting officers for it, is warranted.
Acknowledgments and disclosures
This research was supported by grant R01 MH082813 from the National Institute of Mental Health. The authors greatly appreciate the support and assistance provided by Ms. Letheshia Husbands, Ms. Harriett Laurence, and Ms. Pat Strode in the study implementation and collection of data.
The authors report no competing interests.